State of Health in the EU Estonia Country Health Profile 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Stern Twin-Propeller Effects on Harbor Infrastructures. Experimental Analysis
water Article Stern Twin-Propeller Effects on Harbor Infrastructures. Experimental Analysis Anna Mujal-Colilles 1,* , Marcel· la Castells 2, Toni Llull 1, Xavi Gironella 1 and Xavier Martínez de Osés 2 1 Marine Engineering Laboratory, Department of Civil and Environmental Engineering, Universitat Politècnica de Catalunya, C/ Jordi Girona 1, 08034 Barcelona, Spain; [email protected] (T.L.); [email protected] (X.G.) 2 Department of Nautical Science and Engineering, Universitat Politècnica de Catalunya, Pla de Palau, 18, 08003 Barcelona, Spain; [email protected] (M.l.C.), [email protected] (X.M.d.O.) * Correspondence: [email protected]; Tel.: +34-93-401-7017 Received: 12 October 2018; Accepted: 30 October 2018; Published: 2 November 2018 Abstract: The growth of marine traffic in harbors, and the subsequent increase in vessel and propulsion system sizes, produces three linked problems at the harbor basin area: (i) higher erosion rates damaging docking structures; (ii) sedimentation areas reducing the total depth; (iii) resuspension of contaminated materials deposited at the seabed. The published literature demonstrates that there are no formulations for twin stern propellers to compute the maximum scouring depth. Another important limitation is the fact that the formulations proposed only use one type of maneuvering during the experimental campaign, assuming that vessels are constantly being undocked. Trying to reproduce the real arrival and departure maneuvers, 24 different tests were conducted at an experimental laboratory in a medium-scale water tank using a twin propeller model to estimate the consequences and the maximum scouring depth produced by stern propellers during the backward/docking and forward/undocking scenarios. -

Is the Greek Crisis One of Supply Or Demand?
YANNIS M. IOANNIDES Tufts University CHRISTOPHER A. PISSARIDES London School of Economics Is the Greek Crisis One of Supply or Demand? ABSTRACT Greece’s “supply” problems have been present since its acces- sion to the European Union in 1981; the “demand” problems caused by austerity and wage cuts have compounded the structural problems. This paper discusses the severity of the demand contraction, examines product market reforms, many of which have not been implemented, and their potential impact on com- petitiveness and the economy, and labor market reforms, many of which have been implemented but due to their timing have contributed to the collapse of demand. The paper argues in favor of eurozone-wide policies that would help Greece recover and of linking reforms with debt relief. reece joined the European Union (EU) in 1981 largely on politi- Gcal grounds to protect democracy after the malfunctioning political regimes that followed the civil war in 1949 and the disastrous military dictatorship of the years 1967–74. Not much attention was paid to the economy and its ability to withstand competition from economically more advanced European nations. A similar blind eye was turned to the economy when the country applied for membership in the euro area in 1999, becom- ing a full member in 2001. It is now blatantly obvious that the country was not in a position to compete and prosper in the European Union’s single market or in the euro area. A myriad of restrictions on free trade had been introduced piecemeal after 1949, with the pretext of protecting those who fought for democracy. -

21 Triglav Trophy ANNOUNCEMENT
SLOVENE SKATING UNION FIGURE SKATING CLUB JESENICE Slovene Skating Union Figure Skating Club Jesenice e-mail: [email protected] e-mail: [email protected] 21st Triglav Trophy INTERNATIONAL FIGURE SKATING COMPETITION JESENICE, SLOVENIA, April 4th–8th, 2012 ANNOUNCEMENT Organizer: Figure Skating Club Jesenice Slovene Skating Union Ledarska 4, 4270 Jesenice Celovška 25, 1000 Ljubljana Slovenia Slovenia Venue: “Podmežakla” Ice Rink, Jesenice (indoor ice rink, size 30m x 60m) Time: April 4st- April 8th, 2012 Events: SINGLE SKATING: SENIOR – Ladies, Men JUNIOR – Ladies, Men ADVANCED NOVICE – Girls, Boys _________________________________________________________________ General note: The competition will be held in accordance with the ISU Regulations figure Skating 2010 and respective ISU Communications for Figure Skating. Competition will fulfil also Communication N. 1460 paragraph 2. - ISU World Standings. TRIGLAV TROPHY 2012 1 ANNOUNCEMENT SLOVENE SKATING UNION FIGURE SKATING CLUB JESENICE Technical panel will be from (3) different ISU countries. If there are minimum 8 single skaters out of four different ISU countries, points for World Standings will be awarded. Participation: ISU Members Each team may enter four competitors (two ladies, two men) in senior single skating events and four competitors (two ladies, two men) in each category in single skating of junior and novice events (unless the Organizing Committee decides otherwise). The entries that were placed the first three at the ISU Junior Grand Prix Final 2011/2012 and ISU Grand Prix Final 2011/2012 and the medallists of the World Junior Championships 2012, Europe and World Championships 2012, are not counted into the quota above. The Slovene Skating Union and the organiser reserve the right to enter additional teams and additional competitors in each category. -

European Views on the UK's Renegotiation: Spain, Finland
blogs.lse.ac.uk http://blogs.lse.ac.uk/europpblog/2015/10/29/european-views-on-the-uks-renegotiation-spain-finland-estonia-and-cyprus/ European views on the UK’s renegotiation: Spain, Finland, Estonia and Cyprus The success or failure of David Cameron’s planned renegotiation of the UK’s EU membership will depend to a large extent on how the other 27 EU member states respond to his proposals. But how do countries across the EU view the UK’s renegotiation? Building on a report published in 2014 by the German Council on Foreign Relations, EUROPP is running a series of overviews of the renegotiation from each of the EU’s member states. Compiled by the LSE’s Tim Oliver and written by authors based at universities and research institutions, the overviews will set out what discussion – if any – there has been about the renegotiation and the wider views within each country on the renegotiation and a potential Brexit. This post is the fifth in the series and gives views from Spain, Finland, Estonia and Cyprus. Spain: A flexible but Europeanist Response Finland: Supportive, but a wait-and-see approach Estonia: Brexit would be contrary to Estonia’s interests Cyprus: Special ties with the UK will determine Cyprus’s final stance Spain: A Flexible but Europeanist Response Europeanism still defines Spaniards’ attitudes on foreign policy. Unlike other EU countries, no Eurosceptic parties have emerged during the harsh years of the economic and financial crisis, nor have the main political parties or other social organizations developed any anti-European discourse. -
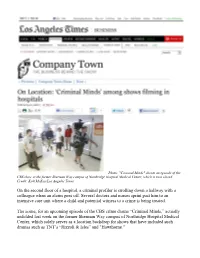
On the Second Floor of a Hospital, a Criminal Profiler Is Strolling Down a Hallway with a Colleague When an Alarm Goes Off
Photo: "Criminal Minds" shoots an episode of the CBS show at the former Sherman Way campus of Northridge Hospital Medical Center, which is now closed. Credit: Kirk McKoy/Los Angeles Times On the second floor of a hospital, a criminal profiler is strolling down a hallway with a colleague when an alarm goes off. Several doctors and nurses sprint past him to an intensive care unit where a child and potential witness to a crime is being treated. The scene, for an upcoming episode of the CBS crime drama “Criminal Minds,” actually unfolded last week on the former Sherman Way campus of Northridge Hospital Medical Center, which solely serves as a location backdrop for shows that have included such dramas such as TNT’s “Rizzoli & Isles” and "Hawthorne." The Northridge facility is among a dozen current and onetime medical centers and hospitals represented by Real to Reel Inc., a 30-year-old Van Nuys location agency that has built a successful niche supplying location managers with something they frequently seek: film-ready hospital settings. “Hospitals are a staple of crime dramas. Someone’s always getting shot, so we’re always going to the hospitals,” said Jeffrey Spellman, location manager for “Criminal Minds,” which plans to shoot its next episode at another closed hospital, St. Luke Medical Center in Pasadena. “To have a facility like this makes our job much easier.” Though Real to Reel books productions for a variety of commercial properties, including the popular Hollywood & Highland Center, at least 40% of its business comes from steering movies and TV shows to hospitals. -

CRASCO, Lauren
LAUREN CRASCO PRODUCTION DESIGNER crascodesign.com TELEVISION SKINNY DIP (Pilot) CBS TV/CW Prod: Garrett Lerner, Russel Friend Dir: Marc Buckland Dale Williams, Peter Traugott THE BRAVE (Pilot) Universal TV/NBC Prod: Richard Ross, Dean Georgaris Dir: Brad Anderson Ben Rimmer ZOO (Pilot, Seasons 1 & 2) CBS Television/CBS Prod: Michael Katleman, Grace Gilroy Dir: Brad Anderson Cathy Konrad Various THE RED ROAD (Season 2) Sundance TV Prod: Robin Sweet, Sarah Condon Dir: Randall Einhorn Jeremy Webb GRACELAND (Season 2) 20th Century Fox TV/USA Prod: Russell Fine, Jeff Eastin, Paul Marks Dir: Various RIZZOLI & ISLES (Seasons 3 & 4) Warner Horizon TV/TNT Prod: Michael Katleman, Janet Tamaro Dir: Various Kevin Cremin LOCAL TALENT (Pilot) Universal Cable Prod./USA Prod: Jonathan Starch, Nathan Lane Dir: Douglas McGrath MEMPHIS BEAT (Season 2) Warner Horizon TV/TNT Prod: Michael Katleman, Jan Nash Dir: Various THE WYOMING STORY (Pilot) Warner Bros. TV/CW Prod: Matt Nodella Dir: Amy Sherman-Palladino FAIRLY LEGAL (Pilot) Universal Cable Prod./USA Prod: Christine Sacani, Susan McConnell Dir: Bronwen Hughes (Art Director) SOLVING CHARLIE (Pilot) ABC Studios/ABC Prod: Randi Richmond, Susan McConnell Dir: Gregory Hoblit LEVERAGE (Pilot, Season 1) Electric Ent./TNT Prod: Marc Roskin, Phil Goldfarb Dir: Dean Devlin Gary Strangis Various THE CLOSER (Pilot, Seasons 1 & 2) Warner Bros. TV/TNT Prod: James Duff, Greer Shephard Dir: Michael Robin Various WANTED (Pilot) Warner Bros. TV/CBS Prod: Mychelle Deschamps Dir: Gregory Hoblit GILMORE GIRLS (Seasons 2 & 3) Warner Bros. TV/WB Prod: Amy Sherman-Palladino Dir: Chris Long, Jamie Babbit Patricia Palmer POPULAR (Pilot, Seasons 1 & 2) Touchstone TV/WB Prod: Michael Robin, Ryan Murphy Dir: Brian Robbins Greer Shephard Various BEYOND BELIEF (Season 3) Dick Clark Prod./Fox Prod: Butch Kaplan Dir: Various (Art Director) NYPD BLUE (Seasons 4 & 5) 20th Century Fox TV/ABC Prod: Bob Doherty, Steven Bochco Dir: Various (Asst. -

A Textual Analysis of the Closer and Saving Grace: Feminist and Genre Theory in 21St Century Television
A TEXTUAL ANALYSIS OF THE CLOSER AND SAVING GRACE: FEMINIST AND GENRE THEORY IN 21ST CENTURY TELEVISION Lelia M. Stone, B.A., M.P.A. Thesis Prepared for the Degree of MASTER OF ARTS UNIVERSITY OF NORTH TEXAS December 2013 APPROVED: Harry Benshoff, Committee Chair George Larke-Walsh, Committee Member Sandra Spencer, Committee Member Albert Albarran, Chair of the Department of Radio, Television and Film Art Goven, Dean of the College of Arts and Sciences Mark Wardell, Dean of the Toulouse Graduate School Stone, Lelia M. A Textual Analysis of The Closer and Saving Grace: Feminist and Genre Theory in 21st Century Television. Master of Arts (Radio, Television and Film), December 2013, 89 pp., references 82 titles. Television is a universally popular medium that offers a myriad of choices to viewers around the world. American programs both reflect and influence the culture of the times. Two dramatic series, The Closer and Saving Grace, were presented on the same cable network and shared genre and design. Both featured female police detectives and demonstrated an acute awareness of postmodern feminism. The Closer was very successful, yet Saving Grace, was cancelled midway through the third season. A close study of plot lines and character development in the shows will elucidate their fundamental differences that serve to explain their widely disparate reception by the viewing public. Copyright 2013 by Lelia M. Stone ii TABLE OF CONTENTS Chapters Page 1 INTRODUCTION .............................................................................................. -

TV to Die For: a Ranking of TV Shows by Dead Bodies
TV to Die For: A Ranking of TV Shows by Dead Bodies Is death entertaining? Is our popular culture obsessed with death? How do portrayals of death affect the popularity of entertainment programs? Who is most likely to be drawn to death- oriented programs? Funeralwise.com seeks to answer these and other questions about the role of death in popular culture. The objective is to create a dialogue contrasting our acceptance of death in the abstract, such as in entertainment programs, vs. how we deal with the reality of our mortality, such as our willingness to make funeral plans in advance. For purposes of this study, Funeralwise has chosen to focus on television because of its popularity with all age groups. The study will determine the presence of death in TV shows by counting dead bodies appearing in the shows. Forty (40) television series have been selected for analysis. The study will be conducted in the first quarter of 2012 and will analyze the most recent 8 original episodes of each series. About Funeralwise.com -- Providing “everything you need to know about funerals,” Funeralwise.com helps individuals and families navigate end-of-life experiences. Featuring an array of online funeral planning tools, Funeralwise.com is changing the way we deal with funerals in the digital age. The ease and convenience of online funeral planning helps people overcome their reluctance to plan ahead, and the availability of comparison shopping tools enables them to be smarter shoppers of funeral goods and services. How are we Conducting the Study? The television series selected for the study are those that regularly include portrayals of death in their story lines. -
Euro Changeover-Related Inflation in Estonia
WORKING PAPER SERIES NO 1732 / SEPTEMBER 2014 ONE CURRENCY, ONE PRICE? EURO CHANGEOVER-RELATED INFLATION IN ESTONIA Jaanika Meriküll and Tairi Rõõm GROCERY PRICES IN THE EURO AREA: FINDINGS FROM INFORMAL ESCB EXPERT GROUP SET-UP TO ANALYSE A DISAGGREGATED PRICE DATASET In 2014 all ECB publications feature a motif taken from the €20 banknote. NOTE: This Working Paper should not be reported as representing the views of the European Central Bank (ECB). The views expressed are those of the authors and do not necessarily refl ect those of the ECB. Grocery prices in the euro area: Findings from informal ESCN expert group to analsyse a disaggregated price dataset This paper was prepared as part of a Eurosystem project group established to analyse a large-scale disaggregated dataset on grocery prices in the euro area. This proprietary dataset was obtained as a follow up to the 2011 Eurosystem Structural Issues Report (SIR) entitled “Structural features of the distributive trades and their impact on prices in the euro area”. The main motivation for obtaining these data was to enable the analysis of a variety of issues that was previously not possible owing to data limitations. More specifi cally (i) analysis of Single Market issues and quantifi cation of border effects (ii) measuring the impact of competition – both at the producer and retail level – on consumer price levels and (iii) consider potential implications for infl ation measurement arising from structural changes in retail sector such as the growing importance of discounters and private label brands. The data were obtained from Nielsen, an international market information and measurement company. -
The Magazine of Memphis University School • November 2008 from the Editor It’S an Exciting Time at School As We Get Closer to the End of the First Semester
The Magazine of Memphis University School • November 2008 From the Editor It’s an exciting time at school as we get closer to the end of the first semester. Many thanks go to our teachers who do so much for our boys. Our seniors are busy applying to colleges across the United States, at ME M PHIS UNIVERSITY SCHOOL the same time our juniors start looking for the right Founded 1893 college. Our theater troupe just finished a well-attended, MISSION STATE M ENT four-performance run of Macbeth and are looking ahead Memphis University School is a to the spring performances of Thurber’s Carnival and college-preparatory school dedicated to Little Shop of Horrors. We also showcased student art, academic excellence and the development of well-rounded young men of strong photography, and mosaic heads on Macbeth’s opening moral character, consistent with the night. We welcomed more than 400 guests at our Admissions Open House. school’s Christian tradition. As we went to press, eighth-grader Zach Olsen won the state golf championship, HEAD M ASTER our football team was undefeated, our cross country team placed ninth at state, Ellis L. Haguewood our swimming and bowling teams were in mid-season, and basketball was just beginning. It’s a busy time for everyone in the halls of MUS. BOARD OF TR U STEES Robert E. Loeb ’73, Chairman In this issue of MUS Today, you’ll read about Henry Klyce ’65 who has D. Stephen Morrow ’71, Vice Chairman spent his career inventing things to keep us healthy, and our first Olympian, Richard L. -

Adapting to Change UK Policy Towards the Arctic Polar Regions Department Foreign and Commonwealth Office, King Charles Street, London SW1A 2AH
Adapting To Change UK policy towards the Arctic Polar Regions Department Foreign and Commonwealth Office, King Charles Street, London SW1A 2AH © Crown copyright 2013. You may re-use this information (not Any enquiries regarding this including logos) free of charge in any publication should be sent to us format or medium, under the terms of at [email protected]. the Open Government Licence. To view this licence, visit www. This publication is available for download nationalarchives.gov.uk/doc/ at www.official-documents.gov.uk. opengovernment-licence/ or write to the Information Policy Team, The National Archives, Kew, London TW9 4DU,or email: [email protected]. Adapting To Change UK policy towards the Arctic i - Adapting To Change - UK policy towards the Arctic Mark Simmonds Minister for the Polar Regions Foreign and Commonwealth Office Adapting To Change - UK policy towards the Arctic - ii Foreword “There is no doubt that the Arctic is on the frontier of global climate change impacts. Temperatures are rising twice as fast in the Arctic as over the rest of the world.” The Arctic has proved, time and again, to be As this document sets out, the United Kingdom one of the most dynamic and influential regions will continue to support and respect the sovereign of the world, despite its remoteness from large rights of the Arctic States to exercise jurisdiction population centres and its often challenging over their territory; the people who live and work geographical and climatic conditions. in the Arctic; and the unique and fragile natural environment. At the same time it outlines the The United Kingdom is not an Arctic State, but United Kingdom’s legitimate interests in the we are the Arctic’s nearest neighbour. -
ICE Enforcement and Removal Operations Report
ICE Enforcement and Removal Operations Report Fiscal Year 2014 December 19, 2014 U.S. Immigration and Customs Enforcement . Enforcement and Removal Operations Table of Contents Background ...................................................................................................................... 1 Discussion ........................................................................................................................ 2 Appendix A ...................................................................................................................... 12 Appendix B ...................................................................................................................... 18 i I. Background This report summarizes U.S. Immigration and Customs Enforcement’s (ICE) Fiscal Year (FY) 2014 civil immigration enforcement and removal operations. ICE shares responsibility for enforcing the Nation’s civil immigration laws with U.S. Customs and Border Protection (CBP) and U.S. Citizenship and Immigration Services (USCIS). In executing its enforcement duties, ICE focuses on two core missions: (1) identifying and apprehending public safety threats—including criminal aliens and national security targets—and other removable individuals within the United States; and (2) detaining and removing individuals apprehended by ICE and CBP officers and agents patrolling our Nation’s borders. Each year, ICE immigration enforcement is impacted by operational factors, including the size of the removable population found in the interior and