International Maritime Health Association
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Notes on Diving in Ancient Egypt
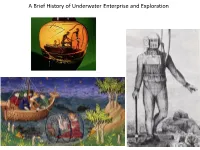
A Brief History of Underwater Enterprise and Exploration The incentives to risk one’s life underwater from the earliest records of diving: 1) Subsistence and general aquatic harvest 2) Commerce/salvage 3) Warfare A sponge diver about to take the plunge, Classical Greece ca. 500 BCE The beginnings: subsistence in Ancient Egypt: skin divers netting fish in the Nile th Tomb of Djar, 11 Dynasty (ca. 2000 BCE) ‘Pull out well! (It is) a Happy day! Measure you, measure you, for you, good great fishes’ Text and image from the tomb of Ankhtifi (ca. 2100 BCE) The beginnings: other kinds of aquatic/underwater harvest: mother of pearl (left) and sponge diving (right) Mesopotamia (southern Iraq, ca. 2500 BCE) Classical Greece (ca. 500 BCE) The so-called ‘Standard of Ur’: a mosaic of lapis lazuli A sponge diver about to take the (from the exotic region of Afghanistan) and mother of plunge with a knife and a sack, the pearl (from the exotic source of a seabed), deposited in jar was also deposited in an elite tomb an elite tomb in Mesopotamia The beginnings: in search of exotic and high value things (things difficult to access/procure) Epic of Gilgamesh (composed in Mesopotamia no later than ca. 2100 BCE) records a heroic dive after a ‘plant of immortality’ on the seabed ‘He tied heavy stones *to his feet+ They pulled him down into the deep [and he saw the plant] He took the plant though it pricked his hands He cut the heavy stones from his feet The sea cast him up upon the shore’ The value of mother of pearl and sea sponge resides, in part, in the process of procuring them The beginnings: salvaging lost cargoes (lost valuable things) Scyllias and his daughter Hydna: the first professional divers known by name, famed for salvaging huge volumes of gold and silver (tribute and booty) from a Persian fleet in the Aegean that lost many ships in a storm (ca. -

Sponge Fishing in Tarpon Springs, Florida Michael Suver University of South Florida, [email protected]
University of South Florida Scholar Commons Graduate Theses and Dissertations Graduate School January 2012 Environmental Change and Place-Based Identities: Sponge Fishing in Tarpon Springs, Florida Michael Suver University of South Florida, [email protected] Follow this and additional works at: http://scholarcommons.usf.edu/etd Part of the Geography Commons Scholar Commons Citation Suver, Michael, "Environmental Change and Place-Based Identities: Sponge Fishing in Tarpon Springs, Florida" (2012). Graduate Theses and Dissertations. http://scholarcommons.usf.edu/etd/4410 This Thesis is brought to you for free and open access by the Graduate School at Scholar Commons. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Scholar Commons. For more information, please contact [email protected]. Environmental Change and Place-Based Identities: Sponge Fishing in Tarpon Springs, Florida by Michael Suver A thesis submitted in partial fulfillment of the requirements for the degree of Master of Arts Department of Geography, Environment, and Planning College of Arts and Sciences University of South Florida Major Professor: Pratyusha Basu, Ph.D. M. Martin Bosman, Ph.D. Jayajit Chakraborty, Ph.D. Date of Approval: November 8, 2012 Keywords: climate change, Greek ethnicity, environmental geography, Gulf of Mexico Copyright © 2012, Michael Suver Acknowledgments I could not have completed this thesis without the strength of the Lord which has enabled me to lay aside all of my weight and finish the race set before me. I am also very thankful to Gabrielle, my fiancé who has been an encouragement and a comfort to get me through the writing process. -

Let Your Light Shine
The Lutheran Beacon Let your light shine . WWW.SELC.LCMS.ORG Published by the SELC District of the Lutheran Church - Missouri Synod MAY 2016 St. John (Cudahy WI) Celebrates Slovak Heritage Celebrating Our Life in Christ by Rev. Carl Krueger St. John, Cudahy WI is celebrating 110 years of Ministry! Founded in 1906 by Slovak Immigrants, St. John “kicked-off” this Anniversary observance year with English/Slovak Communion Worship Services led by the “last-remaining-100% Slovak Heritage-full-time-active- Slovak-Pastors”, and a Slovak menu dinner. At the turn of the 20th Century, Slovakia was ruled by the Hungarian Empire, and subjected to political, social, and religious oppression and persecution. The United States was seen as the land of freedom and opportunity. Slovak men made their way to the Milwaukee area Happy Mother’s Day and found work at the Patrick Cudahy Meat Packing Company May 8th slaughtering and processing beef and pork. The men worked long hours, saved money, then sent for their wives and families. Almost every Slovak adult packed their Slovak Bible and their Slovak Hymnal. First, families found homes, then they sought to establish a Church. “The Slovak Evangelical Lutheran Church of the Unaltered Augsburg Confession, St. John the Baptizer” was founded October 1906, with the city of Cudahy established the same year. The Pastor of a near- by German Lutheran Church provided pastoral care and worship services, along with visiting Slovak Pastors from Chicago IL and Whiting IN. To obtain their own Pastor from the Seminary, St. John needed to join the Slovak Evangelical Lutheran Church (SELC). -

|||GET||| Group Interaction in High Risk Environments 1St Edition
GROUP INTERACTION IN HIGH RISK ENVIRONMENTS 1ST EDITION DOWNLOAD FREE Rainer Dietrich | 9781351932097 | | | | | Looking for other ways to read this? Computational methods such as resampling and bootstrapping are also used when data are insufficient for direct statistical methods. There is little point in making highly precise computer calculations on numbers that cannot be estimated accurately Group Interaction in High Risk Environments 1st edition. Categories : Underwater diving safety. Thus, the surface-supplied diver is much less likely to have an "out-of-air" emergency than a scuba diver as there are normally two alternative air sources available. Methods for dealing with Group Interaction in High Risk Environments 1st edition risks include Provision for adequate contingencies safety factors for budget and schedule contingencies are discussed in Chapter 6. This genetic substudy included Two Sister Study participants and their parents, and some Sister Study participants who developed incident breast cancer invasive or DCIS before age 50 during the follow-up period. In terms of generalizability, our sample is predominantly non-Hispanic white women, and the results may not apply to other racial or ethnic groups. This third parameter may give some management support by establishing early warning indicators for specific serious risks, which might not otherwise have been established. ROVs may be used together with divers, or without a diver in the water, in which case the risk to the diver associated with the dive is eliminated altogether. Suitable equipment can be selected, personnel can be trained in its use and support provided to manage the foreseeable contingencies. However, taken together, there is the possibility that many of the estimates of these factors would prove to be too optimistic, leading. -

Survival and Growth of Cut Vs Hooked Commercial Sponges in the Florida Keys
Survival and growth of cut vs hooked commercial sponges in the Florida Keys Item Type monograph Authors Stevenly, John; Sweat, Don Publisher Florida Sea Grant College Download date 27/09/2021 22:47:01 Link to Item http://hdl.handle.net/1834/18012 Technical Paper No. 38 Survival and Growth of Cut vs Hooked Commercial Sponges in the Florida Keys by John Stevely and Don Sweat I"U)RIM =A GRANT COLL€G€ StEVIXU AM) GRCWTH OF CUT vs . HOOKED COMMERCIAL SPONGES IN THE FU3RIDA KEYS John Stevely and Don Sweat Florida Sea Grant Extension Program 117 Newins-Ziegler Hall University of Florida Gainemille, FL 32611 Project No. IR-82-15 Grant No. NA8OAA-D-00038 Technical Papers are duplicated in limited quantities for specialized audiences requiring rapid access to infonoation. They are published with limited editing and without formal review by the Florida Sea Grant College Program. Content is the sole responsibility of the author. This paper was developed by the Florida Sea Grant College Program with support frcm NQ7Ul Office of Sea Grant, U.S. Department of Ccmnerce, grant nwlber NA8OAA-D-00038. It was published by the Sea Grant Extension Program which functions as a aanponent of the Florida Cooperative Extension Service, John T. Woeste, Dean, in conducting Cmpxative Extension work in Agriculture, Hme Economics, and marine Sciences, State of Florida, U.S. Department of -ce, and Eoards of Cormty Ccmaissioners, cooperating. Printed and distributed in furtherance of the Acts of Congress of May 8 and June 14, 1914. The Florida Sea Grant College is an Equal Rployment-Affinoative Action employer authorized to provide research, educational infonoation and other services only to individuals and institutions that function without regard to race, color, sex, or national origin. -

Sponges on Coral Reefs: a Community Shaped by Competitive Cooperation
Boll. Mus. Ist. Biol. Univ. Genova, 68: 85-148, 2003 (2004) 85 SPONGES ON CORAL REEFS: A COMMUNITY SHAPED BY COMPETITIVE COOPERATION KLAUS RÜTZLER Department of Zoology, National Museum of Natural History, Smithsonian Institution, Washington, D.C. 20560-0163, USA E-mail: [email protected] ABSTRACT Conservationists and resource managers throughout the world continue to overlook the important role of sponges in reef ecology. This neglect persists for three primary reasons: sponges remain an enigmatic group, because they are difficult to identify and to maintain under laboratory conditions; the few scientists working with the group are highly specialized and have not yet produced authoritative, well-illustrated field manuals for large geographic areas; even studies at particular sites have yet to reach comprehensive levels. Sponges are complex benthic sessile invertebrates that are intimately associated with other animals and numerous plants and microbes. They are specialized filter feeders, require solid substrate to flourish, and have varying growth forms (encrusting to branching erect), which allow single specimens to make multiple contacts with their substrate. Coral reefs and associated communities offer an abundance of suitable substrates, ranging from coral rock to mangrove stilt roots. Owing to their high diversity, large biomass, complex physiology and chemistry, and long evolutionary history, sponges (and their endo-symbionts) play a key role in a host of ecological processes: space competition, habitat provision, predation, chemical defense, primary production, nutrient cycling, nitrification, food chains, bioerosion, mineralization, and cementation. Although certain sponges appear to benefit from the rapid deterioration of coral reefs currently under way in numerous locations as a result of habitat destruction, pollution, water warming, and overexploitation, sponge communities too will die off as soon as their substrates disappear under the forces of bioerosion and water dynamics. -

Lessons from a Historic Example of Diving Safety Rules Violation: the Case of Greek Sponge Divers
Int Marit Health 2020; 71, 1: 28–33 10.5603/IMH.2020.0008 www.intmarhealth.pl REVIEW ARTICLE Copyright © 2020 PSMTTM ISSN 1641–9251 Lessons from a historic example of diving safety rules violation: the case of Greek sponge divers Costas Tsiamis , Georgia Vrioni , Athanassios Tsakris Department of Microbiology, Medical School, National and Kapodistrian University of Athens, Greece ABSTRact This study presents a historical example of systematic safety rules violations by professional sponge divers in Greece during the early 20th century. In light of absolute unaccountability in favour of economic competition and in the absence of state oversight, the profession of sponge diving had developed into a deadly undertaking. The study is based on a report compiled by Professor of Hygiene and Microbiology Konstantinos Savvas, which was addressed to the Ministry of Marine Affairs. Savvas’ report rested on data concerning hospitalised divers derived from the medical records of warship ‘Kriti’ (Crete), which escorted groups of Greek fishing vessels to four of their expedition in the Mediterranean over the period 1900–1903. Although the events explored herein took place at a time much different from the modern era with its nu- merous advancements in hyperbaric medicine, enhanced divers’ professionalism and the establishment of labour rights and strict safety regulations, we should not overlook the human factor of professional explo- itation that leads to the violation of safety rules. On the other hand, supervisory authorities entrusted with the responsibility of overseeing professional activities ought to be vigilant on a constant basis, especially in times of economic crisis that may lead to lax state functioning. -

Kontraindikace Pro Rekreační Potápění Z
MEZIOBOROVÉ PŘEHLEDY KKONTRAINDIKACEONTRAINDIKACE PROPRO REKREAČNÍREKREAČNÍ POTÁPĚNÍPOTÁPĚNÍ Z POHLEDUPOHLEDU PRAKTICKÉHOPRAKTICKÉHO LLÉKAŘEÉKAŘE prof. MUDr. František Novomeský, PhD.1, MUDr. Michal Palkovič, PhD.2 1Ústav súdneho lekárstva a medicínskych expertíz JLF UK, Martin International Association of Nitrox and Technical Divers, Central Europe Advisory Board (IANTD, USA) 2Ústav patologickej anatómie LF UK, Bratislava Professional Association of Diving Instructors (PADI, USA) Rekreační potápění se v posledních dvou desítiletích v České i Slovenské republice stalo významnou aktivitou volného času. V obou státech je vycvičeno a registrováno několik tisíc potápěčů, stovky z nich každoročně vyjíždějí na potápěčské destinace po celém světě. Vytvořila se tak rozsáhlá skupina osob s někdy i dosti vysokou hyperbarickou expozicí. Praktický lékař se obvykle dostane do kontaktu s potápěním ve dvou situacích: při žádosti o posouzení zdravotní způsobilosti uchazeče o potápěčský výcvik, nebo při průběžném posou- zení zdravotní způsobilosti již certifikovaného potápěče. Práce je zaměřena na poskytnutí základního přehledu zdravotních kontraindikací pro udělení lékařského souhlasu k rekreační potápěčské činnosti. Klíčová slova: potápění, kontraindikace, zdravotní způsobilost. Med. Pro Praxi 2008; 5(6): 265–269 Úvod do vraků či jeskyní bez možnosti přímého vynoření rozhodovacím algoritmu praktického lékaře, která Vynález těžkého skafandru s přilbou Angličanem na hladinu (8, 12). Jedná se zde sice o rekreační může vyústit buď do přílišné rigorozity (která ucha- Augustem Siebem v roce 1836 (6) znamenal překro- potápěče, avšak s významně vyšší hyperbarickou zeče o potápění odradí), anebo přílišné benevolence čení Rubikonu v pronikaní člověka do mořských hlu- expozicí, tomu odpovídající vysokou rizikovostí (která může adepta potápění ohrozit). bin. Desítky kilogramů vážící potápěčská souprava a náročností na medicínsky výběr zájemců o tech- Je zcela evidentní, že každý potápěč – rekreač- umožnila vykonat člověku na mořském dně první nické potápění. -

Shipwrecks Abc & Spice Islands
Deeplens.com SHIPWRECKS OF THE ABC & S PICE ISLANDS PETER COLLINGS INTERNATIONAL AWARD WINNING AUTHOR, PHOTOGRAPHER & WRECK HUNTER Celebrating 25 Years of the RSWA Forward by John Womack 1 Deeplens.com 2 Deeplens.com SHIPWRECKS OF THE ABC & SPICE ISLANDS Celebrating 25 years of THE RED SEA WRECK ACADEMY 3 Deeplens.com FORWARD by JOHN WOMACK I am John Womack Snr, BSAC First Class Diver, Advanced Instructor & owner of Otter Drysuits in Yorkshire, having dived the Britannic, Prince of Wales, Repulse and the Victoria plus many more over the last 40 years I would not go anywhere in the Red Sea without one of Peter's guide books. I have been on numerous successful trips of Peter's including wreck searching in Truk Lagoon. Peter's new book is awesome, there are so many wrecks and to give detailed descriptions of all the wrecks themselves is great, it makes you feel like you have dived them already. I remember doing a night dive on the Thistlegorm which was just fantastic it was pitch black with pin points of light from fellow divers lights.In the south, Peter, Tom and myself went looking for the wreck of the Maidan on Rocky Island, we followed the debris trail down to 65mtrs and there before us was the huge shadow of the wreck hanging over the abyss starting at 80 mtrs. We could only look down in wonder, but we had found what we were looking for after 10 years. Peter's trips are a must and very much like his trips his books are a must read, Peter is a walking encyclopaedia on all things diving and ship wrecks. -

Download PDF -.:: GEOCITIES.Ws
CHAPTER 11 Beneath the 12-Mile Reef: Archival curio of 20th century sponger culture Hannah Hjerpe-Schroeder [Emory University] Greetings! Kalispera. Thank you so much for being here, for having us. A big thank you to SOAS and Mr. Emery for putting together what will likely be the most unique conference I will ever attend. I believe academia is at its best and most vital when it seeks out similarities rather than staking out differences, and the interdisciplinary nature of this conference makes it truly something special. A little about myself. I am a PhD student in Literature at Emory University in Atlanta, Georgia, in the United States, where my primary focus is 20th and 21st century Caribbean fiction. I came across the call for papers for this conference on the website for the Caribbean Studies Association last autumn and knew I had to be here – and not just because it was here, on the beautiful island of Hydra. My interest in Caribbean literature is largely contingent on my interest in the ways in which island geography has the power to shape human narrative. So here is a bit of mine. I was born and raised in the city of Key West: a small island off the southern coast of Florida. Key West is the southernmost point of the continental United States, and is geographically closer to Cuba than it is to Miami. I grew up in and around the Gulf of Mexico, learning the names of the flora and fauna that called the ocean home. As a little girl, my parents would take me to the ocean and quiz me on what I saw – barracuda, tarpon, stingrays, corals, and yes – sponges. -

October 2, 2018 Florida Division of Historical
October 2, 2018 Florida Division of Historical Resources State Historic Preservation Officer R.A. Gray Building 500 S. Bronough Street Tallahassee, FL 32399-0250 RE: Nomination of the Cycadia Cemetery to the National Register of Historic Places Dear State Historic Preservation Officer, The City of Tarpon Springs is a Certified Local Government. As such, the City is committed to an ongoing effort to preserve and protect its historical resources and cultural heritage. To that end, as Mayor of the City of Tarpon Springs, and on behalf of the Board of Commissioners and citizens, we enthusiastically support the nomination of the Cycadia Cemetery to the National Register of Historic Places. The Cycadia Cemetery is a significant historic cemetery. Although not physically contiguous with the Greektown Historic District, Cycadia Cemetery has always been an integral part of its cultural complex. The cemetery has remained in constant use into the present and consists of more than 3,166 grave plots of local Greek Americans. The site retains its historic design, setting and integrity to a high degree. It contributes to the sense of place, historic development and culture of the Greek community in Tarpon Springs. Cycadia Cemetery is nominated to the National Register of Historic Places for local significance under Criterion A in the areas of Ethnic Heritage/European-Greek, for its direct association with the Greek community and its cultural and religious practices and under Criterion C: Art, for the distinctive style of its Greek American funerary monuments. The City of Tarpon Springs Heritage Preservation Board approved the nomination at the September 10, 2018 regular meeting and made a recommendation to the Mayor and Board of Commissioners to support the nomination application. -

Spatial and Temporal Adaptation of a Traditional Mediterranean Fishery of Mortality and Changes in Pigmentation When Compared to A
10th World Sponge Conference Ecology Sacoleve - Spatial And Temporal Adaptation Of A Traditional Mediterranean Fishery of mortality and changes in pigmentation when compared to A. cauliformis and C. delitrix. However, a dis- Facing Regional Change: Combining History And Ecology To Study Past, Present And ease affected more fragments of A. cauliformis and C. delitrix under stress temperature. Tissue regeneration Future Of Sponge Harvesting occurred for all three species under both treatments. This experimental study shows that temperature affects sponge species differently, and suggests that C. delitrix and A. cauliformis fragments better tolerate short fluc- Maïa Fourt1, Daniel Faget2, Thierry Pérez1 tuations in seawater temperature than D. anchorata. 1 Institut Méditerranéen de Biodiversité et d’Ecologie marine et continentale, UMR CNRS 7263 / IRD 237 / Aix Marseille Univer- sité / Université d’Avignon. Station Marine d’Endoume, rue de la batterie des lions 13007 Marseille, France Geographic Variability in Antibacterial Chemical Defenses Among Branching 2 Temps, Espaces, Langage, Europe Méridionale et Méditerranée, UMR CNRS 7303 / Aix Marseille Morphotypes of Caribbean Aplysina Université. Maison Méditerranéenne des Sciences de l’Homme, 5 rue du Château de l’Horloge, BP 647, 13094 Aix-en-Provence Cedex 2, France Deborah Gochfeld1, 4, Savannah Stockton2, Claire Vickers2, Cole Easson3 & Marc Slattery4 The production of Mediterranean bath sponges collapsed during the past century as it is shown by Tunisian 1 National Center for Natural Products Research, University of Mississippi, Oxford, MS, USA catches which fell from 108 tons in 1920 down to 9 tons in 1988. Another example is given by the well-known [email protected] sponge fishing island of Kalymnos which lost about 90% of its active fishermen population in a century be- 2 Sally McDonnell Barksdale Honors College, University of Mississippi, Oxford, MS, USA tween 1858 and 1967.