Care for All
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Physician Directory, Currently Licensed And
Physician Directory, Currently Licensed and Practising in the Province Information is accurate as of: Monday, July 16, 2018 8:00 am Name Office Address City Prov Postal Code CCFP Specialty Abara, Chukwuma Solomon Thompson Clinic, 50 Selkirk Avenue Thompson MB R8N 0M7 Abazid, Nizar Rizk Health Sciences Centre, Section of Neonatology, 820 Sherbrook Street Winnipeg MB R3A 1R9 Abbott, Burton Bjorn Seven Oaks General Hospital, 2300 McPhillips Street Winnipeg MB R2V 3M3 CCFP Abbu, Ganesan Palani Dr. C.W. Wiebe Medical Centre, 385 Main Street Winkler MB R6W 1J2 Abdelmessih, Mary Rose Maurice Virden Medical Associates, Box 730 Virden MB R0M 2C0 CCFP Yacoub Abdulrahman, Suleiman Yinka St. Boniface Hospital, Room M5038, 409 Tache Avenue Winnipeg MB R2H 2A6 Psychiatry Abdulrehman, Abdulhamid Suleman 200 Ste. Anne's Road Winnipeg MB R2M 3A1 Abej, Esmail Ahmad Abdullah Winnipeg Clinic, 425 St. Mary Ave Winnipeg MB R3C 0N2 CCFP Gastroenterology; Internal Medicine Abell, Margaret Elaine 134 First Street, Box 70 Wawanesa MB R0K 2G0 Abell, William Robert Rosser Avenue Medical Clinic, 841 Rosser Avenue Brandon MB R7A 0L1 Abidullah, Mohammad Westman Regional Laboratory, Rm 146 L, 150 McTavish Avenue Brandon MB R7A 7H8 Anatomical Pathology Abisheva, Gulniyaz Nurlanbekovna Pine Falls Health Complex, 37 Maple Street, Bo 1500 Pine Falls MB R0E 1M0 Ableman, Rami (RL) Resident - Pediatrics - Emergency Medicine Winnipeg MB (RL) Practitioners with a residency licence are fully registered and enrolled in a resident training program at the University of Manitoba. By agreement and in return for a reduced annual fee, their licence limits their practice to those duties directly related to the residency program. -

Main Estimates Supplement 2021-2022 | Manitoba Health and Seniors Care
Budget 2021 Main Estimates Supplement Budgets complémentaires 2021/22 MANITOBA HEALTH SANTÉ ET SOINS AND SENIORS CARE AUX PERSONNES ÂGÉES MANITOBA MAIN ESTIMATES BUDGET SUPPLEMENT COMPLÉMENTAIRE 2021-2022 2021-2022 Department of Ministère de la Health and Seniors Care Santé et des Soins aux personnes âgées Minister’s Message and Executive Summary This document has been produced by Manitoba Health and Seniors Care as a supplement to the Printed Estimates of Expenditure. It is intended to provide background information on the department and complements the information already contained in the Printed Estimates of Expenditure. The contents of this document are organized into five parts. The first part provides an overview of the ministry including its strategy roadmap, strategic priorities, objectives and initiatives. The second part provides financial information on staffing and expenditures. The third part provides information on the amount of money the department requires, the spending and allocation plan, and how expenses will flow throughout the fiscal year. The fourth part provides a risk analysis overview. The fifth part provides the statutory responsibilities of the minister and a standard glossary of terms. Recently implemented across the Manitoba government, balanced scorecards foster operational improvements by reinforcing transparency, urgency, alignment and accountability. They have been added to the redesigned Supplement to identify key priorities for each department that staff will work towards, with appropriate performance measures. With the Supplement redesigned to be a business plan that focuses on strategic priorities, departments can then take steps to create operating plans that further identify how strategic priorities will translate into day-to-day operations. -

Physician Directory
Physician Directory, Currently Practicing in the Province Information is accurate as of: 9/24/2021 8:00:12 AM Page 1 of 97 Name Office Address City Prov Postal Code CCFP Specialty Abara, Chukwuma Solomon Thompson Clinic, 50 Selkirk Avenue Thompson MB R8N 0M7 CCFP Abazid, Nizar Rizk Health Sciences Centre, Section of Neonatology, 665 William Avenue Winnipeg MB R3E 0L8 Abbott, Burton Bjorn Seven Oaks General Hospital, 2300 McPhillips Street Winnipeg MB R2V 3M3 CCFP Abbu, Ganesan Palani C.W. Wiebe Medical Centre, 385 Main Street Winkler MB R6W 1J2 CCFP Abbu, Kavithan Ganesan C.W. Wiebe Medical Centre, 385 Main Street Winkler MB R6W 1J2 CCFP Abdallateef, Yossra Virden Health Centre, 480 King Street, Box 400 Virden MB R0M 2C0 Abdelgadir, Ibrahim Mohamed Ali Manitoba Clinic, 790 Sherbrook Street Winnipeg MB R3A 1M3 Internal Medicine, Gastroenterology Abdelmalek, Abeer Kamal Ghobrial The Pas Clinic, Box 240 The Pas MB R9A 1K4 Abdulrahman, Suleiman Yinka St. Boniface Hospital, Room M5038, 409 Tache Avenue Winnipeg MB R2H 2A6 Psychiatry Abdulrehman, Abdulhamid Suleman 200 Ste. Anne's Road Winnipeg MB R2M 3A1 Abej, Esmail Ahmad Abdullah Winnipeg Clinic, 425 St. Mary Ave Winnipeg MB R3C 0N2 CCFP Gastroenterology, Internal Medicine Abell, Margaret Elaine 134 First Street, Box 70 Wawanesa MB R0K 2G0 Abell, William Robert Rosser Avenue Medical Clinic, 841 Rosser Avenue Brandon MB R7A 0L1 Abidullah, Mohammad Westman Regional Laboratory, Rm 146 L, 150 McTavish Avenue Brandon MB R7A 7H8 Anatomical Pathology Abisheva, Gulniyaz Nurlanbekovna Pine Falls Health Complex, 37 Maple Street, Box 1500 Pine Falls MB R0E 1M0 CCFP Abo Alhayjaa, Sahar C W Wiebe Medical Centre, 385 Main Street Winkler MB R6W 1J2 Obstetrics & Gynecology Abou-Khamis, Rami Ahmad Northern Regional Health, 867 Thompson Drive South Thompson MB R8N 1Z4 Internal Medicine Aboulhoda, Alaa Samir The Pas Clinic, Box 240 The Pas MB R9A 1K4 General Surgery Abrams, Elissa Michele Meadowwood Medical Centre, 1555 St. -
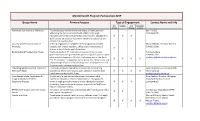
Mental Health Program Partnerships 2019 Group Name Primary Purpose
Mental Health Program Partnerships 2019 Group Name Primary Purpose Type of Engagement Contact Name and Info Info Feedback Joint Participant Sharing Planning Control Addictions Foundation of Manitoba To contribute to the health and well-being of Manitobans by Ben Fry CEO addressing the harm associated with addictions through 204-944-6200 education, prevention, rehabilitation and research. Collaborative X X X work focuses on co-occurring mental health and substance use disorders at a system level. Anxiety Disorders Association of Self-help organization committed to helping individuals who Mary Williams, Executive Director Manitoba struggle with anxiety disorders. Offers cognitive behavioural X 204-925-0600 groups, support groups and information. Block-by-Block Thunderwing Project The Block-by-Block Thunderwing project will bring multiple Pauline Jackson government and non-government agencies together, partnering to 204-938-7342 solve social problems in a 21-block, high-crime area of the North [email protected] X X X X End. This program is supported by the police, Manitoba Justice and a broad range of community-based agencies, helping families and the community become more resilient. CODI Program/River East & Transcona To provide enhanced consultation services on co-occurring Gale Colquhoun – CODI My Health My Health Team disorders to fee-for-service physicians signed on with the River X X X X Team Clinician East/Transcona My Health Team. [email protected] Coordinated Intake, Assessment & A coalition of organizations who support individuals who Brian Bechtel, Director, Winnipeg Triage Advisory Committee experience episodic or chronic homelessness. One goal is to Poverty Reduction Council (Doorways Project) create a single point of contact to assist individuals and those X X X 204-924-4295 supporting them to navigate supports as part of the Task Force Plan to End Homelessness. -

Debates Proceedings ·:::
Second Session - Thirty-Sixth Legislature of the Legislative Assembly of Manitoba DEBATES and PROCEEDINGS (Hansard) Publishedunder the authorityof TheHonourable LouiseM. Dacquay Speaker .· · ... �·:::��-...:��� Vol. XLVI No. 21-1:30 p.m., Monday, April22, 1996 ISSN 0542-5492 MANITOBA LEGISLATIVE ASSEMBLY Thirty-sixth Legislature Members, Constituencies and Political Affiliation Name CnnstihJency � ASHTON, Steve Thompson N.D.P. BARRETI, Becky Wellington N.D.P. CERILLI, Marianne Radisson N.D.P. CHOMIAK, Dave K.ildonan N.D.P. CUMMINGS, Glen, Hon. Ste. Rose P.C. DACQUAY, Louise, Hon. Seine River P.C. DERKACH, Leonard, Hon. Robl in-Russell P.C. DEWAR, Gregory Selkirk N.D.P. DOER, Gary Concordia N.D.P. DOWNEY, James, Hon. Arthur-Virden P.C. DRIEDGER, Albert, Hon. Steinbach P.C. DYCK, Peter Pembina P.C. ENNS, Harry, Hon. Lakeside P.C. ERNST, Jim, Hon. Charles wood P.C. EVANS, Clif Interlake N.D.P. EVANS, Leonard S. Brandon East N.D.P. FILMON, Gary, Hon. Tuxedo P.C. FINDLAY, Glen, Hon. Springfield P.C. FRIESEN, Jean Wolseley N.D.P. GAUDRY, Neil St. Boniface Lib. GILLESHAMMER, Harold, Hon. Minnedosa P.C. HEL WER, Edward Gimli P.C. HICKES, George Point Douglas N.D.P. JENNISSEN, Gerard Flin Flon N.D.P. KOWALSKI, Gary The Maples Lib. LAMOUREUX, Kevin Inkster Lib. LATHLIN, Oscar The Pas N.D.P. LAURENDEAU, Marcel St. Norbert P.C. MACKINTOSH, Gord St. Johns N.D.P. MALOWAY, Jim Elmwood N.D.P. MARTINDALE, Doug Burrows N.D.P. McALPINE, Gerry Sturgeon Creek P.C. McCRAE, James, Hon. Brandon West P.C. McGIFFORD, Diane Osborne N.D.P. -
Legislative Assembly of Manitoba DEBATES and PROCEEDINGS
Fourth Session- Thirty-Sixth Legislature of the Legislative Assembly of Manitoba DEBATES and PROCEEDINGS Official Report (Hansard) Published under the authority of The Honourable Louise M. Dacquay Speaker Vol. XLVIII No. 14 .• 1:30 p.m., Thesday, March 10, 1998 ISSN 0542-5492 MANITOBA LEGISLATIVE ASSEMBLY Thirty-Sixth Legislature Member Constituency Political Aftlliation ASHTON, Steve Thompson N.D.P. BARRETT, Becky Wellington N.D.P. CERILLI, Marianne Radisson N.D.P. CHOMIAK, Dave Kildonan N.D.P. CUMMINGS, Glen, Hon. Ste. Rose P.C. DACQUAY, Louise, Hon. Seine River P.C. DERKACH, Leonard, Hon. Roblin-Russell P.C. DEWAR, Gregory Selkirk N.D.P. DOER, Gary Concordia N.D.P. DOWNEY, James, Hon. Arthur-Virden P.C. DRIEDGER, Albert Steinbach P.C. DYCK, Peter Pembina P.C. ENNS, Harry, Hon. Lakeside P.C. EVANS, Clif Interlake N.D.P. EVANS, Leonard S. Brandon East N.D.P. FAURSCHOU, David Portage Ia Prairie P.C. FILMON, Gary, Hon. Tuxedo P.C. FINDLAY, Glen, Hon. Springfield P.C. FRIESEN, Jean Wolseley N.D.P. GAUDRY, Neil St. Boniface Lib. GILLESHAMMER, Harold, Hon. Minnedosa P.C. HELWER, Edward Gimli P.C. HICKES, George Point Douglas N.D.P. IENNISSEN, Gerard Flin Flon N.D.P. KOWALSKI, Gary The Maples Lib. LAMOUREUX, Kevin Inkster Lib. LATHLIN, Oscar The Pas N.D.P. LAURENDEAU, Marcel St. Norbert P.C. MACKINTOSH, Gord St. Johns N.D.P. MALOWAY, Jim Elmwood N.D.P. MARTINDALE, Doug Burrows N.D.P. McALPINE, Gerry Sturgeon Creek P.C. McCRAE, James, Hon. Brandon West P.C. McGIFFORD, Diane Osborne N.D.P. -

Manitoba EIA Health Benefits Summary
Manitoba EIA Health Benefits Summary The Manitoba EIA program is a “program of last resort” for about 62,000 Manitoban’s who do not have any other financial support or income. Many of these individuals have disabilities and high health care needs. The program has a living allowance, rental allowance called Rent Assist, as well as disability benefit for those that qualify. All EIA recipients all qualify for health care coverage and benefits. This chart is a summary of those health benefits as well as commentary on the gaps between these benefits and the true costs for health care. This chart was created recognizing poverty as a determinant of health with the knowledge that the EIA program incomes are far below all poverty measures of income to meet basic needs. The poverty and limited health coverage for people relying on EIA contributes to health in equities and adds costs to government in other areas. “Injustice will not be destroyed until those who are not affected by it are as outraged as though who are” – Unknown “While explaining our project, the recipient started to laugh. In response to the project description he said, “I apologize, I am just jaded to being optimistic for positive change in this system”. The reason being, people just do not care about poor people - not politicians, not middle class” – EIA Recipient Benefit Coverage Comment Recommendations Personal Experience Health Services Yes 3 month waiting period for Disabled & Single Parents A health manager recommends that EIA policy “I do not think it is appropriate to make people wait so long for their Program: 6 months for General Assistance (GA) for Dental and should allow third party referrals for people who needs” - EIA Recipient Waiting periods Optical coverage cannot apply on their own. -

Directory – Indigenous Organizations in Manitoba
Indigenous Organizations in Manitoba A directory of groups and programs organized by or for First Nations, Inuit and Metis people Community Development Corporation Manual I 1 INDIGENOUS ORGANIZATIONS IN MANITOBA A Directory of Groups and Programs Organized by or for First Nations, Inuit and Metis People Compiled, edited and printed by Indigenous Inclusion Directorate Manitoba Education and Training and Indigenous Relations Manitoba Indigenous and Municipal Relations ________________________________________________________________ INTRODUCTION The directory of Indigenous organizations is designed as a useful reference and resource book to help people locate appropriate organizations and services. The directory also serves as a means of improving communications among people. The idea for the directory arose from the desire to make information about Indigenous organizations more available to the public. This directory was first published in 1975 and has grown from 16 pages in the first edition to more than 100 pages in the current edition. The directory reflects the vitality and diversity of Indigenous cultural traditions, organizations, and enterprises. The editorial committee has made every effort to present accurate and up-to-date listings, with fax numbers, email addresses and websites included whenever possible. If you see any errors or omissions, or if you have updated information on any of the programs and services included in this directory, please call, fax or write to the Indigenous Relations, using the contact information on the -
Wave Magazine
WINNIPEG’S HEALTH & WELLNESS MAGAZINE SEPT/OcT 2010 BAcK TO ScHOOL 5 nutritious ideas for your child’s lunch bag BREATHING EASY One 10-year-old boy’s struggle against asthma DON’T GO VIRAL Get the shot, not the flu 60 MINUTES That’s all it takes to gain a lifetime of good health PLUS PRIME TIME Full-service care for seniors Supportive housing offers seniors independence within a safe, secure environment Pour une version française téléphonez au 926.7000 Rendez vous à notre site Web : www.wrha.mb.ca/lecourant Lee Denture Clinic Denturists: Bill and Tom Lee Don’t under estimate the importance of Denture After Care! Make sure to schedule your annual free check up. At Lee Denture Clinic we create that special or natural smile just for you. For Cosmetic Full or Partial Dentures, Magnetic Repel Dentures or Dentures Over Implants meet with Bill or Tom of Lee Denture Clinic to discuss all of your denture needs. With proper fi tting dentures you will Feel good and Look great! Creating Beautiful Smiles Since 1955 274 Smith Street, Winnipeg, Manitoba R3C 1K1 943-4048 1-866-943-4048 Visit us online at: www.leedentureclinic.com The only Downtown Main Floor Denture Clinic in Winnipeg between Portage and Grahamm AAvenuevenue (Free parking at the rear of the building) Main Floor Wheelchair Access This issue of is brought to you by the following sponsors: Lee Denture Clinic Denturists: Bill and Tom Lee Don’t under estimate the importance of Denture After Care! Make sure to schedule your annual free check up. -
Manitoba Response Monitor
North American COVID-19 Policy Response Monitor: Manitoba July 3, 2020 What is the North American COVID-19 Policy Response Monitor? The North American COVID-19 policy monitor has been designed to collect and organize up-to-date information on how jurisdictions are responding to the crisis. It summarizes responses of health systems as well as wider public health initiatives. The North American policy monitor is an offshoot of the international COVID-19 Health System Response Monitor (HSRM), a joint undertaking of the WHO Regional Office for Europe, the European Commission and the European Observatory on Health Systems and Policies. Canadian content to HSRM is contributed by the North American Observatory on Health Systems and Policies (NAO). Contents 1. Preventing transmission ........................................................................................................................... 2 2. Ensuring sufficient physical infrastructure and workforce capacity ....................................................... 13 3. Providing health services effectively....................................................................................................... 15 4. Paying for services .................................................................................................................................. 19 5. Governance ............................................................................................................................................. 20 6. Measures in other sectors ..................................................................................................................... -

Mbtelehealth: Report to Our Partners
University of Calgary PRISM: University of Calgary's Digital Repository Research Centres, Institutes, Projects and Units E-Health Resource Repository 2003 MBTelehealth: Report to Our Partners. MBTelehealth MBTelehealth MBTelehealth. 2003. MBTelehealth: Report to Our Partners. MBTelehealth: Winnipeg, MB. 1-47. http://hdl.handle.net/1880/43075 unknown Downloaded from PRISM: https://prism.ucalgary.ca MBTelehealth Network Sites Marquette and South Westrnan were amalgamated into ~ssiniboineRHA in Spring, 2002 By Wayne Bo-ye,MBTelehealth Director, WRHA sector suppliers of equipment and services, sent home to be official representatives of the hospital information technology (I.T.) new network. Dear Reader; departments and health administrators from all regions of the province. In less than a year, the network was ready to As you thumb through the pictures, charts and go. Manitoba Health Minister David Chomiak articles that follow, you will be struck, as I was, At the beginning of the MBTelehealth project, officiated at the network launch in February by the diversity of people, places and activities in early March 2001, the late Dr. Ron Duhamel, 2002 with a connection to Flin Flon. By April that have been a part of the growth of telehealth senior federal cabinet minister for Manitoba, all sites with the exception of Norway House in Manitoba. accompanied by Cabinet colleague Dr. Rey were functioning. It came on board in June. These past two years have been demanding, to Pagtakhan, offered support for the project while pledging $3 million for development over the At almost every site patients started coming be sure. They have involved the mastery of new immediately. -

Vendor Payments Over $50,000 20
FOR THE YEAR ENDED MARCH 31, 2020 Vendor Payments Over $50,000 20 VENDOR STATEMENT OF CONSOLIDATED FUND PAYMENTS IN EXCESS OF $50,000 TO CORPORATIONS, FIRMS, INDIVIDUALS, OTHER GOVERNMENTS AND GOVERNMENT AGENCIES For the fiscal year ended March 31, 2020 (UNAUDITED) ………………………………………………… INFORMATION 1. This statement lists, in alphabetical order within Department or Special Operating Agency, each payee whose total payments by that individual department or special operating agency exceeded $50,000 during the fiscal year. Payments are presented on a gross basis to show all amounts which were charged to the 2019-2020 fiscal period for the purchase of goods and services, investment and loan transactions, grant payments and refunds as well as payments from amounts held in trust on behalf of others. 2. Where a Department or Special Operating Agency did not have any payee meeting the threshold of total payments exceeding $50,000, it is noted that there are “NO REPORTING VENDORS”. 3. Where multiple, same name vendors are found within a city/town, they are applicable to different locations. 4. Where the name of a city/town appears twice, in succession, the first is attached to the vendor’s name, the second is applicable to the vendor’s address. 5. This statement also lists, in alphabetical order within department, vendors from whom departmental purchases, using the National Bank of Canada procurement cards, are equal to or exceeding $25,000 during the fiscal year. 6. Payments in other currencies are shown in the Canadian dollar equivalent at the time of payment. 7. The location of the payee is shown except where payment was made to an address in Winnipeg.