The South African Fattail Scorpion Revisited
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Channel Toxin from Parabuthus Transvaalicus
Eur. J. Biochem. 269, 5369–5376 (2002) Ó FEBS 2002 doi:10.1046/j.1432-1033.2002.03171.x A single charged surface residue modifies the activity of ikitoxin, a beta-type Na+ channel toxin from Parabuthus transvaalicus A. Bora Inceoglu1,*, Yuki Hayashida2, Jozsef Lango3, Andrew T. Ishida2 and Bruce D. Hammock1 1Department of Entomology and Cancer Research Center, 2Section of Neurobiology, Physiology and Behavior, and 3Department of Chemistry and Superfund Analytical Laboratory, University of California, Davis, CA, USA We previously purified and characterized a peptide toxin, from birtoxin by a single residue change from glycine to birtoxin, from the South African scorpion Parabuthus glutamic acid at position 23, consistent with the apparent transvaalicus. Birtoxin is a 58-residue, long chain neurotoxin mass difference of 72 Da. This single-residue difference that has a unique three disulfide-bridged structure. Here we renders ikitoxin much less effective in producing the same report the isolation and characterization of ikitoxin, a pep- behavioral effect as low concentrations of birtoxin. Elec- tide toxin with a single residue difference, and a markedly trophysiological measurements showed that birtoxin and reduced biological activity, from birtoxin. Bioassays on mice ikitoxin can be classified as beta group toxins for voltage- showed that high doses of ikitoxin induce unprovoked gated Na+ channels of central neurons. It is our conclusion jumps, whereas birtoxin induces jumps at a 1000-fold lower that the N-terminal loop preceding the a-helix in scorpion concentration. Both toxins are active against mice when toxins is one of the determinative domains in the interaction administered intracerebroventricularly. -

Scorpion Stings and Venoms
Scorpion stings and venoms The term scorpionism is the medical term used to describe the syndrome of scorpion stings. We focus here on the thick-tailed scorpions in the family Buthidae, which are the most dangerous scorpions in South Africa (See Dangerous scorpions: how to identify them). Find out here about how to prevent being stung, the signs and symptoms of scorpionism, and scorpionism management. Introduction In South Africa we are fortunate to have a fascinating and diverse scorpion fauna and yet a low incidence of scorpionism, unlike areas in the south-western U.S.A., Mexico, east-central South America, north Africa, the Middle East and India where the incidence of serious scorpion envenomation is high. Worldwide, there are about 100,000 cases of scorpion envenomation resulting in approximately 800 deaths per year. Locally more than 95% of cases of scorpionism results in no more than local pain lasting from several minutes to about 4 hours with most of the Ischnurid stings resulting in no more than a pin prick. In South Africa there are only 1 to 4 deaths a year resulting from Parabuthus envenomation (nothing in comparison to car, crime, sport or health related deaths). Parabuthus capensis. [image N. Larsen ©] Parabuthus transvaalicus. [image L. Prendini ©] A case study of 42 serious scorpion envenomations, occurring in western Cape over 5 summers (1986/7 to 1991/2), recorded 4 fatalities of children. Parabuthus granulatus was found to be the main culprit, responsible for 3 deaths. Parabuthus capensis was the alleged culprit of the fourth death but as the specimen was lost it cannot be verified. -

The Spider Club News
The Spider Club News Editor: Joan Faiola JUNE 2011 - Vol.27 #2 Natural History – A Love Poem by E.B. White (1899-1985) (Author of Charlotte’s Web) The spider, dropping down from twig, Unfolds a plan of her devising, A thin premeditated rig To use in rising. And all that journey down through space, In cool descent and loyal hearted, She spins a ladder to the place From where she started. COPYRIGHT: E.B. WHITE AND GARTH WILLIAMS Thus I, gone forth as spiders do (Respectively Author and Illustrator of Charlotte’s In spider's web a truth discerning, Web) Attach one silken thread to you For my returning. Spider Club News June 2011 P a g e 1 Contents Page No. Who are we? 3 Mission Statement 3 Contact Details 3 From the Hub Chairman’s letter 4 From the Editor 4 Books Books for sale; WS Bristowe 5 Snippets from the Times - Alien Scorpion in Britain 6 Webs of Spiders on drugs 7 Corregium – Gea infuscata 8 Arachno Mugs for sale 8 Events Reports De Beers, Benfontein, Kimberley 9 Moreson, Limpopo 10 Spider Sorting at ARC 12 Interesting sightings - Waferlid Trapdoor Spider in Limpopo 13 Thomisid and two males 13 South African Nephilids catch birds 14 Scientific news & comment Spidernauts in space 15 New Pterinochilus species for S Africa 16 New Caerostris sp. for Madagascar 17 ARC and SANSA 18 NEWS Photo Gallery Jack Hochfeld 19 Spider Club diary 21 2011/2012 DISCLAIMER THE VIEWS OF THE CONTRIBUTORS TO THIS PUBLICATION DO NOT NECESSARILY COINCIDE WITH THOSE OF THE SPIDER CLUB OF SOUTHERN AFRICA. -

Defensive Behavior Is Associated with Morphology and Performance in Scorpions
Choose Your Weapon: Defensive Behavior Is Associated with Morphology and Performance in Scorpions Arie van der Meijden1*, Pedro Lobo Coelho1, Pedro Sousa1, Anthony Herrel2 1 CIBIO, Centro de Investigac¸a˜o em Biodiversidade e Recursos Gene´ticos, Campus Agra´rio de Vaira˜o, Vaira˜o, Portugal, 2 UMR 7179, Muse´um National d9Histoire Naturelle, De´partement d9Ecologie et de Gestion de la Biodiversite´, Paris, France Abstract Morphology can be adaptive through its effect on performance of an organism. The effect of performance may, however, be modulated by behavior; an organism may choose a behavioral option that does not fully utilize its maximum performance. Behavior may therefore be decoupled from morphology and performance. To gain insight into the relationships between these levels of organization, we combined morphological data on defensive structures with measures of defensive performance, and their utilization in defensive behavior. Scorpion species show significant variation in the morphology and performance of their main defensive structures; their chelae (pincers) and the metasoma (‘‘tail’’) carrying the stinger. Our data show that size-corrected pinch force varies to almost two orders of magnitude among species, and is correlated with chela morphology. Chela and metasoma morphology are also correlated to the LD50 of the venom, corroborating the anecdotal rule that dangerously venomous scorpions can be recognized by their chelae and metasoma. Analyses of phylogenetic independent contrasts show that correlations between several aspects of chela and metasoma morphology, performance and behavior are present. These correlations suggest co-evolution of behavior with morphology and performance. Path analysis found a performance variable (pinch force) to partially mediate the relationship between morphology (chela aspect ratio) and behavior (defensive stinger usage). -

Phylogeny of Parabuthus (Scorpiones, Buthidae)
ZSC056.fm Page 13 Thursday, March 15, 2001 2:26 PM PhylogenyBlackwell Science, Ltd of Parabuthus (Scorpiones, Buthidae) LORENZO PRENDINI Accepted: 2 October 2000 Prendini, L. (2001). Phylogeny of Parabuthus (Scorpiones, Buthidae). — Zoologica Scripta, 30, 13–35. A cladistic analysis of the 20 southern African species of Parabuthus Pocock, 1890 (Scorpiones, Buthidae) and five of the eight north-eastern African and Arabian species is presented, based on 53 characters, mostly of the adult morphology. The resultant topology is largely congruent with Lamoral’s (1978) unpublished topology for 14 Namibian species. Monophyly of the genus Parabuthus is supported, but monophyly of the disjunct southern African vs. north- eastern African and Arabian species is unsupported. The implications of the cladogram for understanding ecological specialization in Parabuthus, Afrotropical arid biogeography and Parabuthus envenomation are discussed. Lorenzo Prendini, Percy FitzPatrick Institute, University of Cape Town, Rondebosch, 7701, South Africa. E-mail: [email protected] Introduction the southern African species of Parabuthus are today restricted Parabuthus Pocock, 1890 is the fifth largest genus in the diverse, to areas receiving less than 600 mm of rainfall per annum cosmopolitan scorpion family Buthidae (Fet & Lowe 2000). (Newlands 1978a,b). The genus includes the world’s largest buthid scorpions, e.g. In addition to their dependence on aridity, many Parabuthus villosus ( Peters, 1862), Parabuthus transvaalicus Purcell, Parabuthus species are also specialized for life on particular 1899 and Parabuthus schlechteri Purcell, 1899, which can reach a substrata. Several species (e.g. Parabuthus distridor Lamoral, length of 140 mm and a mass of 14 g (Newlands 1974a, 1978a). -
Arthropod Assassins: Crawling Biochemists with Diverse Toxin Pharmacopeias
Accepted Manuscript Arthropod assassins: crawling biochemists with diverse toxin pharmacopeias Volker Herzig PII: S0041-0101(18)31041-9 DOI: https://doi.org/10.1016/j.toxicon.2018.11.312 Reference: TOXCON 6038 To appear in: Toxicon Please cite this article as: Herzig, V., Arthropod assassins: crawling biochemists with diverse toxin pharmacopeias, Toxicon, https://doi.org/10.1016/j.toxicon.2018.11.312. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. ACCEPTED MANUSCRIPT 1 Editorial 2 Arthropod assassins: crawling biochemists with diverse toxin pharmacopeias 3 Volker Herzig 1 4 5 6 1 Institute for Molecular Bioscience, The University of Queensland, St. Lucia QLD 4072, 7 Australia 8 9 10 11 *Address correspondence to: Volker Herzig, Institute for Molecular Bioscience, The University 12 of Queensland, St. Lucia QLD 4072, Australia; Phone: +61 7 3346 2018, Fax: +61 7 3346 2101, 13 Email: [email protected] 14 15 16 17 MANUSCRIPT 18 19 20 21 22 23 24 25 26 ACCEPTED 1 ACCEPTED MANUSCRIPT 27 Abstract 28 The millions of extant arthropod species are testament to their evolutionary success that can at 29 least partially be attributed to venom usage, which evolved independently in at least 19 arthropod 30 lineages. -

Animal Venoms—Curse Or Cure?
biomedicines Editorial Animal Venoms—Curse or Cure? Volker Herzig 1,2 1 GeneCology Research Centre, University of the Sunshine Coast, Sippy Downs, QLD 4556, Australia; [email protected]; Tel.: +61-7-5456-5382 2 School of Science, Technology and Engineering, University of the Sunshine Coast, Sippy Downs, QLD 4556, Australia Abstract: An estimated 15% of animals are venomous, with representatives spread across the majority of animal lineages. Animals use venoms for various purposes, such as prey capture and predator deterrence. Humans have always been fascinated by venomous animals in a Janus-faced way. On the one hand, humans have a deeply rooted fear of venomous animals. This is boosted by their largely negative image in public media and the fact that snakes alone cause an annual global death toll in the hundreds of thousands, with even more people being left disabled or disfigured. Consequently, snake envenomation has recently been reclassified by the World Health Organization as a neglected tropical disease. On the other hand, there has been a growth in recent decades in the global scene of enthusiasts keeping venomous snakes, spiders, scorpions, and centipedes in captivity as pets. Recent scientific research has focussed on utilising animal venoms and toxins for the benefit of humanity in the form of molecular research tools, novel diagnostics and therapeutics, biopesticides, or anti-parasitic treatments. Continued research into developing efficient and safe antivenoms and promising discoveries of beneficial effects of animal toxins is further tipping the scales in favour of the “cure” rather than the “curse” prospect of venoms. Keywords: venom; toxin; toxicity; lethality; envenomation; antivenom; venoms to drugs; therapeu- tics; biopesticide; anti-parasitic Citation: Herzig, V. -
Common Scorpions
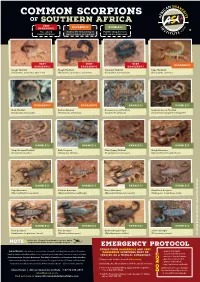
COMMON SCORPIONS OF SOUTHERN AFRICA VERY DANGEROUS DANGEROUS HARMLESS Has caused May be life threatening in Painful sting, but does human fatalities small children and animals not require antivenom VERY VERY VERY DANGEROUS DANGEROUS DANGEROUS DANGEROUS Rough Thicktail Rough Thicktail Transvaal Thicktail Cape Thicktail (Parabuthus granulatus, light form) (Parabuthus granulatus, dark form) (Parabuthus transvaalicus) (Parabuthus capensis) DANGEROUS DANGEROUS HARMLESS HARMLESS Drab Thicktail Eastern Nomad Common Lesser-Thicktail Highveld Lesser-Thicktail (Parabuthus planicauda) (Hottentotta trilineatus) (Uroplectes carinatus) (Uroplectes triangulifer triangulifer) HARMLESS HARMLESS HARMLESS HARMLESS Striped Lesser-Thicktail Bark Scorpion Plain Pygmy-Thicktail Rough Burrower (Uroplectes lineatus) (Uroplectes vittatus) (Pseudolychas ochraceus) (Opistophthalmus glabrifrons) HARMLESS HARMLESS HARMLESS HARMLESS Cape Burrower Kalahari Burrower Karoo Burrower Giant Rock Scorpion (Opistophthalmus capensis) (Opistophthalmus wahlbergii) (Opistophthalmus karrooensis) (Hadogenes troglodytes, male) HARMLESS HARMLESS HARMLESS HARMLESS Rock Scorpion Tree Creeper Drakensberg Creeper Jones’s Creeper (Hadogenes longimanus, female) (Opisthacanthus asper) (Opisthacanthus validus) (Cheloctonus jonesii) © Johan Marais African Snakebite Institute In the case of stings from harmless species, apply NOTE a topical anaesthetic cream to manage the pain. EMERGENCY PROTOCOL Stings from dangerous and very Johan Marais is the author of various books on reptiles, including -

The Isolation, Structure, and Membrane Interactions Of
The isolation, structure, and membrane interactions of biologically active peptides A thesis submitted for the degree of doctor of philosophy By Patrick James Sherman B. Sc. (Hons.) from the Department of Chemistry The University of Adelaide June, 2012 Contents Acknowledgements viii Statement of originality x Abstract xi Abbreviations xiii Chapter 1 Biologically active peptides 1 1.1 Synopsis 1 1.2 Peptide Biosynthesis 2 1.3 Anuran secretions 4 1.3.1 Collection of anuran secretion 5 1.3.2 Australian anuran peptides 7 1.4 Scorpion venoms 13 1.4.1 Collection of scorpion venom 14 1.4.2 Scorpion peptides 15 Chapter 2 Methodology I – Mass Spectrometry 20 2.1 Mass Spectrometry 20 2.2 The Q-TOF2 Mass Spectrometer 21 2.2.1 The Quadrupole analyser 22 2.2.2 The Hexapole Collision Cell 23 2.2.3 The Time of Flight Sector 24 2.3 Electrospray ionisation 25 2.4 Peptide sequence determination 26 2.4.1 High Performance Liquid Chromatography 27 2.4.2 Positive ion fragmentation 27 2.4.3 Negative ion fragmentation 28 2.4.4 Edman Sequencing 31 - ii - Chapter 3 Methodology II – Nuclear Magnetic Resonance Spectroscopy 33 3.1 Nuclear magnetic resonance spectroscopy of peptides in solution 33 3.1.1 Principles of nuclear magnetic resonance spectroscopy 34 3.1.2 One-dimensional NMR spectroscopy 36 3.1.3 Two-dimensional NMR spectroscopy 40 3.1.3.1 Correlation NMR spectroscopy 41 3.1.3.2 Total correlation NMR spectroscopy 44 3.1.3.3 Nuclear Overhauser effect NMR spectroscopy 45 3.1.4 Chemical shift Assignment 46 3.1.5 NOE Connectivities 48 3.1.6 Secondary shifts -
Sites and Species of Conservation Interest for the CESVI Project Area
SPECIES and SITES of CONSERVATION INTEREST for the CESVI PROJECT AREA, SOUTHERN ZIMBABWE edited by Rob Cunliffe October 2000 Occasional Publications in Biodiversity No. 7 SPECIES AND SITES OF CONSERVATION INTEREST FOR THE CESVI PROJECT AREA, SOUTHERN ZIMBABWE R. N. Cunliffe October 2000 Occasional Publications in Biodiversity No. 7 Biodiversity Foundation for Africa P.O. Box FM730, Famona, Bulawayo, Zimbabwe Species and Sites for Conservation in the Southern Lowveld i TABLE OF CONTENTS 1. INTRODUCTION .......................................................1 2. APPROACH ...........................................................1 3. SPECIES LISTS ........................................................2 3.1 Patterns of Diversity ...............................................2 4. SPECIES OF INTEREST .................................................3 5. SITES OF INTEREST....................................................3 6. FURTHER WORK REQUIRED............................................4 7. DISCUSSION ..........................................................4 7.1 Sites of Conservation Interest ........................................4 7.2 The Need for a Broader Overview.....................................5 8. ACKNOWLEDGEMENTS ................................................5 9. REFERENCES .........................................................5 10. TABLES ..............................................................7 Table 1. Numbers of species of various taxa listed..............................7 Table 2. Numbers of species of -
Variation of Protein Profile Among Consecutive Stings
VARIATION OF PROTEIN PROFILE AMONG CONSECUTIVE ……. 61 VARIATION OF PROTEIN PROFILE AMONG CONSECUTIVE STINGS OF THE SCORPION PARABUTHUS LEIOSOMA (FAMILY: BUTHIDAE) FROM EGYPT, SUPPORTS THE VENOM-METERING HYPOTHESIS IN SCORPIONS. MOUSTAFA M.H. SARHAN1, MAGED M.A. FOUDA1, ALAA M.H. ELBITAR1, HAMDY A.M. ALY1 and AHMED B. SAYED2 1Zoology Department, Faculty of Science, Al Azhar University, Assiut 2Zoology Department, Faculty of Science, Al Azhar University, Cairo Abstract Scorpions use their venom to immobilize prey items and defend themselves against predators. Scorpion venom is a complex mixture composed of a wide array of substances such as salts, small molecules, peptides, and proteins. During analysis of the prey capture behavior of the scorpion Parabuthus leiosoma, we noticed that the scorpion stings the prey several successive stings in different specific regions. The stings started with ventral surface of the abdomen followed by thorax, shoulders and finally the head. This finding raised the possibility that the scorpion might use the venom with different composition in different contexts. To check this possibility, venom was collected as sequential drops (stings) by electrical stimulation (20 Volt) of the telson of the Parabuthus leiosoma. Protein content was determined by spectrophotometer using total protein KIT. The results showed marked variation of the total protein among the consecutive stings of each of the investigated scorpions. To go further, the protein profiles for all the collected stings were analyzed separately using 10% SDS-polyacrylamide electrophoresis (SDS-PAGE). Similarly, differences were observed among the stings, not only in the number of the protein bands, but also in the intensity of the bands. -

One Scorpion, Two Venoms: Prevenom of Parabuthus Transvaalicus Acts As an Alternative Type of Venom with Distinct Mechanism of Action
One scorpion, two venoms: Prevenom of Parabuthus transvaalicus acts as an alternative type of venom with distinct mechanism of action Bora Inceoglu*, Jozsef Lango†, Jie Jing‡, Lili Chen‡, Fuat Doymaz§, Isaac N. Pessah‡, and Bruce D. Hammock*¶ Departments of *Entomology and Cancer Research Center, †Chemistry and Superfund Analytical Laboratory, ‡Molecular Biosciences, School of Veterinary Medicine, and §Chemical Engineering and Materials Science, University of California, Davis, CA 95616 Contributed by Bruce D. Hammock, December 3, 2002 Scorpion venom is a complex mixture of salts, small molecules, the venom are reported to be highly folded, disulfide-bridged peptides, and proteins. Scorpions employ this valuable tool in molecules (13). Low yields of expression of these peptides in several sophisticated ways for subduing prey, deterring predators, recombinant systems also hint at the unique and difficult folding and possibly during mating. Here, a subtle but clever strategy of and storage requirements (14). However, used sparingly, venom venom utilization by scorpions is reported. Scorpions secrete a is an excellent tool for both offense and defense. A study on small quantity of transparent venom when initially stimulated that the sting use of Parabuthus species is a good example of the we propose to name prevenom. If secretion continues, a cloudy regulation of sting use according to prey size, demonstrating the and dense venom that is white in color is subsequently released. conservative use of venom (15). The conservative use of venom The prevenom contains a combination of high K؉ salt and several ؉ by many species of scorpions suggests that venom secretion is peptides including some that block rectifying K channels and elicit also regulated.