Essential Genetics 5
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A 10-Year-Old Girl with Foot Pain After Falling from a Tree
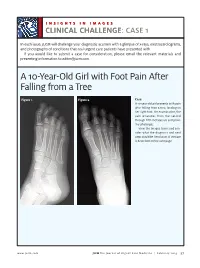
INSIGHTS IN IMAGES CLINICAL CHALLENGECHALLENGE: CASE 1 In each issue, JUCM will challenge your diagnostic acumen with a glimpse of x-rays, electrocardiograms, and photographs of conditions that real urgent care patients have presented with. If you would like to submit a case for consideration, please email the relevant materials and presenting information to [email protected]. A 10-Year-Old Girl with Foot Pain After Falling from a Tree Figure 1. Figure 2. Case A 10-year-old girl presents with pain after falling from a tree, landing on her right foot. On examination, the pain emanates from the second through fifth metatarsals and proxi- mal phalanges. View the images taken and con- sider what the diagnosis and next steps would be. Resolution of the case is described on the next page. www.jucm.com JUCM The Journal of Urgent Care Medicine | February 2019 37 INSIGHTS IN IMAGES: CLINICAL CHALLENGE THE RESOLUTION Figure 1. Mediastinal air Figure 1. Differential Diagnosis Pearls for Urgent Care Management and Ⅲ Fracture of the distal fourth metatarsal Considerations for Transfer Ⅲ Plantar plate disruption Ⅲ Emergent transfer should be considered with associated neu- Ⅲ Sesamoiditis rologic deficit, compartment syndrome, open fracture, or vas- Ⅲ Turf toe cular compromise Ⅲ Referral to an orthopedist is warranted in the case of an in- Diagnosis tra-articular fracture, or with Lisfranc ligament injury or ten- Angulation of the distal fourth metatarsal metaphyseal cortex derness over the Lisfranc ligament and hairline lucency consistent with fracture. Acknowledgment: Images courtesy of Teleradiology Associates. Learnings/What to Look for Ⅲ Proximal metatarsal fractures are most often caused by crush- ing or direct blows Ⅲ In athletes, an axial load placed on a plantar-flexed foot should raise suspicion of a Lisfranc injury 38 JUCM The Journal of Urgent Care Medicine | February 2019 www.jucm.com INSIGHTS IN IMAGES CLINICAL CHALLENGE: CASE 2 A 55-Year-Old Man with 3 Hours of Epigastric Pain 55 years PR 249 QRSD 90 QT 471 QTc 425 AXES P 64 QRS -35 T 30 Figure 1. -

Next Generation Sequencing Panels for Disorders of Sex Development
Next Generation Sequencing Panels for Disorders of Sex Development Disorders of Sex Development – Overview Disorders of sex development (DSDs) occur when sex development does not follow the course of typical male or female patterning. Types of DSDs include congenital development of ambiguous genitalia, disjunction between the internal and external sex anatomy, incomplete development of the sex anatomy, and abnormalities of the development of gonads (such as ovotestes or streak ovaries) (1). Sex chromosome anomalies including Turner syndrome and Klinefelter syndrome as well as sex chromosome mosaicism are also considered to be DSDs. DSDs can be caused by a wide range of genetic abnormalities (2). Determining the etiology of a patient’s DSD can assist in deciding gender assignment, provide recurrence risk information for future pregnancies, and can identify potential health problems such as adrenal crisis or gonadoblastoma (1, 3). Sex chromosome aneuploidy and copy number variation are common genetic causes of DSDs. For this reason, chromosome analysis and/or microarray analysis typically should be the first genetic analysis in the case of a patient with ambiguous genitalia or other suspected disorder of sex development. Identifying whether a patient has a 46,XY or 46,XX karyotype can also be helpful in determining appropriate additional genetic testing. Abnormal/Ambiguous Genitalia Panel Our Abnormal/Ambiguous Genitalia Panel includes mutation analysis of 72 genes associated with both syndromic and non-syndromic DSDs. This comprehensive panel evaluates a broad range of genetic causes of ambiguous or abnormal genitalia, including conditions in which abnormal genitalia are the primary physical finding as well as syndromic conditions that involve abnormal genitalia in addition to other congenital anomalies. -
Understanding Fraser Syndrome
SPECIAL NEEDS // Features Synonyms of Fraser Syndrome • Cryptophthalmos- Syndactyly Syndrome • Cryptophthalmos Syndrome • Cyclopism • Fraser-Francois Syndrome • Meyer-Schwickerath’s Syndrome • Ulrich-Feichtiger Syndrome Understanding Fraser Syndrome A look at how Fraser Syndrome – a rare, non- development of the kidney), skeletal larynx. Lack of kidney function or blockage treatment are often required for those # Ophanet, a consortium of European sex linked genetic disorder – causes anomalies and mental delay. of the larynx is usually the cause of death for surviving Fraser Syndrome-affected children. partners, currently defines a condition rare a wide range of abnormalities, those who are stillborn or die within the first Thanks to advances in genetic counselling when it affects one person per 2,000. particularly vision loss. Associated Symptoms year of infancy. technologies, medical professionals Due to multiple malformations of different 25% of affected infants are stillborn, nowadays find it more effective in carrying * A pattern of inheritance in which both body organs, a child with Fraser Syndrome while 20% die before the age of one out the diagnosis, prenatal treatment and copies of an autosomal gene must be Compilation: Leonard Lau and Yvonne Tan; Photo: stock.xchange is likely to suffer from at least partial visual, year from renal or laryngeal defects. If management of Fraser Syndrome. abnormal for a genetic condition or disease hearing or speech impairment, among other these anomalies are not present, the life Ultrasonographic diagnosis of the to occur. An autosomal gene is a gene A very rare# genetic disorder occurring in Syndrome (the syndrome has a recurrence symptoms. expectancy is almost normal. -

Genetic Mechanisms of Disease in Children: a New Look
Genetic Mechanisms of Disease in Children: A New Look Laurie Demmer, MD Tufts Medical Center and the Floating Hospital for Children Boston, MA Traditionally genetic disorders have been linked to the ‘one gene-one protein-one disease’ hypothesis. However recent advances in the field of molecular biology and biotechnology have afforded us the opportunity to greatly expand our knowledge of genetics, and we now know that the mechanisms of inherited disorders are often significantly more complex, and consequently, much more intriguing, than originally thought. Classical mendelian disorders with relatively simple genetic mechanisms do exist, but turn out to be far more rare than originally thought. All patients with sickle cell disease for example, carry the same A-to-T point mutation in the sixth codon of the beta globin gene. This results in a glutamate to valine substitution which changes the shape and the function of the globin molecule in a predictable way. Similarly, all patients with achondroplasia have a single base pair substitution at nucleotide #1138 of the FGFR3 gene. On the other hand, another common inherited disorder, cystic fibrosis, is known to result from changes in a specific transmembrane receptor (CFTR), but over 1000 different disease-causing mutations have been reported in this single gene. Since most commercial labs only test for between 23-100 different mutations, interpreting CFTR mutation testing is significantly complicated by the known risk of false negative results. Many examples of complex, or non-Mendelian, inheritance are now known to exist and include disorders of trinucleotide repeats, errors in imprinting, and gene dosage effects. -

MR Imaging of Kallmann Syndrome, a Genetic Disorder of Neuronal Migration Affecting the Olfactory and Genital Systems
MR Imaging of Kallmann Syndrome, a Genetic Disorder of Neuronal Migration Affecting the Olfactory and Genital Systems 1 2 2 3 4 Charles L. Truwit, ' A. James Barkovich, Melvin M. Grumbach, and John J. Martini PURPOSE: We report the MR findings in nine patients with clinical and laboratory evidence of Kallmann syndrome (KS), a genetic disorder of olfactory and gonadal development. In patients with KS, cells that normally express luteinizing hormone-releasing hormone fail to migrate from the medial olfactory placode along the terminalis nerves into the forebrain. In addition, failed neuronal migration from the lateral olfactory placode along the olfactory fila to the forebrain results in aplasia or hypoplasia of the olfactory bulbs and tracts. Patients with KS, therefore, suffer both reproductive and olfactory dysfunction. METHODS: Nine patients with KS underwent direct coronal MR of their olfactory regions in order to assess the olfactory sulci, bulbs, and tracts. A lOth patient had MR findings of KS, although the diagnosis is not yet confirmed by laboratory tests. RESULTS: Abnormalities of the olfactory system were identified in all patients. In particular, the anterior portions of the olfactory sulci were uniformly hypoplastic. The olfactory bulbs and tracts appeared hypoplastic or aplastic in all patients in whom the bulb/ tract region was satisfactorily imaged. In two (possibly three) patients, prominent soft tissue in the region of the bulbs suggests radiographic evidence of neurons that have been arrested before migration. CONCLUSIONS: Previous investigators of patients with KS used axial MR images to demonstrate hypoplasia of the olfactory sulci but offered no assessment of the olfactory bulbs. -

The Counsyl Foresight™ Carrier Screen
The Counsyl Foresight™ Carrier Screen 180 Kimball Way | South San Francisco, CA 94080 www.counsyl.com | [email protected] | (888) COUNSYL The Counsyl Foresight Carrier Screen - Disease Reference Book 11-beta-hydroxylase-deficient Congenital Adrenal Hyperplasia .................................................................................................................................................................................... 8 21-hydroxylase-deficient Congenital Adrenal Hyperplasia ...........................................................................................................................................................................................10 6-pyruvoyl-tetrahydropterin Synthase Deficiency ..........................................................................................................................................................................................................12 ABCC8-related Hyperinsulinism........................................................................................................................................................................................................................................ 14 Adenosine Deaminase Deficiency .................................................................................................................................................................................................................................... 16 Alpha Thalassemia............................................................................................................................................................................................................................................................. -

Journal of Medical Genetics April 1992 Vol 29 No4 Contents Original Articles
Journal of Medical Genetics April 1992 Vol 29 No4 Contents Original articles Beckwith-Wiedemann syndrome: a demonstration of the mechanisms responsible for the excess J Med Genet: first published as on 1 April 1992. Downloaded from of transmitting females C Moutou, C Junien, / Henry, C Bonai-Pellig 217 Evidence for paternal imprinting in familial Beckwith-Wiedemann syndrome D Viljoen, R Ramesar 221 Sex reversal in a child with a 46,X,Yp+ karyotype: support for the existence of a gene(s), located in distal Xp, involved in testis formation T Ogata, J R Hawkins, A Taylor, N Matsuo, J-1 Hata, P N Goodfellow 226 Highly polymorphic Xbol RFLPs of the human 21 -hydroxylase genes among Chinese L Chen, X Pan, Y Shen, Z Chen, Y Zhang, R Chen 231 Screening of microdeletions of chromosome 20 in patients with Alagille syndrome C Desmaze, J F Deleuze, A M Dutrillaux, G Thomas, M Hadchouel, A Aurias 233 Confirmation of genetic linkage between atopic IgE responses and chromosome 1 1 ql 3 R P Young, P A Sharp, J R Lynch, J A Faux, G M Lathrop, W 0 C M Cookson, J M Hopkini 236 Age at onset and life table risks in genetic counselling for Huntington's disease P S Harper, R G Newcombe 239 Genetic and clinical studies in autosomal dominant polycystic kidney disease type 1 (ADPKD1) E Coto, S Aguado, J Alvarez, M J Menendez-DIas, C Lopez-Larrea 243 Short communication Evidence for linkage disequilibrium between D16S94 and the adult onset polycystic kidney disease (PKD1) gene S E Pound, A D Carothers, P M Pignatelli, A M Macnicol, M L Watson, A F Wright 247 Technical note A strategy for the rapid isolation of new PCR based DNA polymorphisms P R Hoban, M F Santibanez-Koref, J Heighway 249 http://jmg.bmj.com/ Case reports Campomelic dysplasia associated with a de novo 2q;1 7q reciprocal translocation I D Young, J M Zuccollo, E L Maltby, N J Broderick 251 A complex chromosome rearrangement with 10 breakpoints: tentative assignment of the locus for Williams syndrome to 4q33-q35.1 R Tupler, P Maraschio, A Gerardo, R Mainieri G Lanzi L Tiepolo 253 on September 26, 2021 by guest. -

Cryptophthalmos Syndrome: a Case Report
Case Report Cryptophthalmos Syndrome: A Case Report Jawad Bin Yamin Butt, Tariq Mehmood Qureshi, Muhammad Tariq Khan, Anwar-ul-Haq Ahmad Pak J Ophthalmol 2014, Vol. 30 No.3 . .. .. See end of article for A 20 days female baby presented to us in OPD. She was the 4th child of normal authors affiliations parents with 3 normal siblings. She exhibited few features of cryptophthalmos which fit the criteria of Fraser syndrome. …..……………………….. Key words: Cryptophthalmos, Fraser syndrome, Eye lid defect. Correspondence to: Jawad Bin Yamin Butt Layton Benevolent Trust Hospital (LRBT), 436 A/I Township, Lahore …..……………………….. ryptophthalmos (CO) is defined as a set of rare CASE REPORT congenital eyelid defects in which the lid folds The patient is a 20 days old female. She is the 4th child C are unable to divide in the embryo and the of healthy parents. Her three older siblings are normal skin extends continuously from the forehead with no congenital malformation. The infant is full 1-3 onto the cheeks covering the eyes. CO maybe term and delivered by spontaneous vaginal delivery bilateral or unilateral and fluctuates in severity from which was eventless. The baby weighed 2900 grams at the presence of rudimentary, distorted eyelids to birth and exhibits normal feeding manner. complete absence of eyelids2. Autosomal recessive and autosomal dominant inheritance have been reported, Clinical evaluation exhibits complete absence of but most cases are autosomal recessive.4-8 right side eyelid formation with absent eyelashes. The skin is continuous from the forehead to the cheek, CO is of three clinical types: covering the entire globe. -

The Genetic Basis for Skeletal Diseases
insight review articles The genetic basis for skeletal diseases Elazar Zelzer & Bjorn R. Olsen Harvard Medical School, Department of Cell Biology, 240 Longwood Avenue, Boston, Massachusetts 02115, USA (e-mail: [email protected]) We walk, run, work and play, paying little attention to our bones, their joints and their muscle connections, because the system works. Evolution has refined robust genetic mechanisms for skeletal development and growth that are able to direct the formation of a complex, yet wonderfully adaptable organ system. How is it done? Recent studies of rare genetic diseases have identified many of the critical transcription factors and signalling pathways specifying the normal development of bones, confirming the wisdom of William Harvey when he said: “nature is nowhere accustomed more openly to display her secret mysteries than in cases where she shows traces of her workings apart from the beaten path”. enetic studies of diseases that affect skeletal differentiation to cartilage cells (chondrocytes) or bone cells development and growth are providing (osteoblasts) within the condensations. Subsequent growth invaluable insights into the roles not only of during the organogenesis phase generates cartilage models individual genes, but also of entire (anlagen) of future bones (as in limb bones) or membranous developmental pathways. Different mutations bones (as in the cranial vault) (Fig. 1). The cartilage anlagen Gin the same gene may result in a range of abnormalities, are replaced by bone and marrow in a process called endo- and disease ‘families’ are frequently caused by mutations in chondral ossification. Finally, a process of growth and components of the same pathway. -

Advances in Understanding the Genetics of Syndromes Involving Congenital Upper Limb Anomalies
Review Article Page 1 of 10 Advances in understanding the genetics of syndromes involving congenital upper limb anomalies Liying Sun1#, Yingzhao Huang2,3,4#, Sen Zhao2,3,4, Wenyao Zhong1, Mao Lin2,3,4, Yang Guo1, Yuehan Yin1, Nan Wu2,3,4, Zhihong Wu2,3,5, Wen Tian1 1Hand Surgery Department, Beijing Jishuitan Hospital, Beijing 100035, China; 2Beijing Key Laboratory for Genetic Research of Skeletal Deformity, Beijing 100730, China; 3Medical Research Center of Orthopedics, Chinese Academy of Medical Sciences, Beijing 100730, China; 4Department of Orthopedic Surgery, 5Department of Central Laboratory, Peking Union Medical College Hospital, Peking Union Medical College and Chinese Academy of Medical Sciences, Beijing 100730, China Contributions: (I) Conception and design: W Tian, N Wu, Z Wu, S Zhong; (II) Administrative support: All authors; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: Y Huang; (V) Data analysis and interpretation: L Sun; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Wen Tian. Hand Surgery Department, Beijing Jishuitan Hospital, Beijing 100035, China. Email: [email protected]. Abstract: Congenital upper limb anomalies (CULA) are a common birth defect and a significant portion of complicated syndromic anomalies have upper limb involvement. Mostly the mortality of babies with CULA can be attributed to associated anomalies. The cause of the majority of syndromic CULA was unknown until recently. Advances in genetic and genomic technologies have unraveled the genetic basis of many syndromes- associated CULA, while at the same time highlighting the extreme heterogeneity in CULA genetics. Discoveries regarding biological pathways and syndromic CULA provide insights into the limb development and bring a better understanding of the pathogenesis of CULA. -

Circle Applicable Codes
IDENTIFYING INFORMATION (please print legibly) Individual’s Name: DOB: Last 4 Digits of Social Security #: CIRCLE APPLICABLE CODES ICD-10 ICD-10 ICD-9 DIAGNOSTIC ICD-9 DIAGNOSTIC PRIMARY ICD-9 CODES CODE CODE PRIMARY ICD-9 CODES CODE CODE Abetalipoproteinemia 272.5 E78.6 Hallervorden-Spatz Syndrome 333.0 G23.0 Acrocephalosyndactyly (Apert’s Syndrome) 755.55 Q87.0 Head Injury, unspecified – Age of onset: 959.01 S09.90XA Adrenaleukodystrophy 277.86 E71.529 Hemiplegia, unspecified 342.9 G81.90 Arginase Deficiency 270.6 E72.21 Holoprosencephaly 742.2 Q04.2 Agenesis of the Corpus Callosum 742.2 Q04.3 Homocystinuria 270.4 E72.11 Agenesis of Septum Pellucidum 742.2 Q04.3 Huntington’s Chorea 333.4 G10 Argyria/Pachygyria/Microgyria 742.2 Q04.3 Hurler’s Syndrome 277.5 E76.01 or 758.33 Aicardi Syndrome 333 G23.8 Hyperammonemia Syndrome 270.6 E72.4 Alcohol Embryo and Fetopathy 760.71 F84.5 I-Cell Disease 272.2 E77.0 Anencephaly 655.0 Q00.0 Idiopathic Torsion Dystonia 333.6 G24.1 Angelman Syndrome 759.89 Q93.5 Incontinentia Pigmenti 757.33 Q82.3 Asperger Syndrome 299.8 F84.5 Infantile Cerebral Palsy, unspecified 343.9 G80.9 Ataxia-Telangiectasia 334.8 G11.3 Intractable Seizure Disorder 345.1 G40.309 Autistic Disorder (Childhood Autism, Infantile 299.0 F84.0 Klinefelter’s Syndrome 758.7 Q98.4 Psychosis, Kanner’s Syndrome) Biotinidase Deficiency 277.6 D84.1 Krabbe Disease 333.0 E75.23 Canavan Disease 330.0 E75.29 Kugelberg-Welander Disease 335.11 G12.1 Carpenter Syndrome 759.89 Q87.0 Larsen’s Syndrome 755.8 Q74.8 Cerebral Palsy, unspecified 343.69 G80.9 -

2018 Etiologies by Frequencies
2018 Etiologies in Order of Frequency by Category Hereditary Syndromes and Disorders Count CHARGE Syndrome 958 Down syndrome (Trisomy 21 syndrome) 308 Usher I syndrome 252 Stickler syndrome 130 Dandy Walker syndrome 119 Cornelia de Lange 102 Goldenhar syndrome 98 Usher II syndrome 83 Wolf-Hirschhorn syndrome (Trisomy 4p) 68 Trisomy 13 (Trisomy 13-15, Patau syndrome) 60 Pierre-Robin syndrome 57 Moebius syndrome 55 Trisomy 18 (Edwards syndrome) 52 Norrie disease 38 Leber congenital amaurosis 35 Chromosome 18, Ring 18 31 Aicardi syndrome 29 Alstrom syndrome 27 Pfieffer syndrome 27 Treacher Collins syndrome 27 Waardenburg syndrome 27 Marshall syndrome 25 Refsum syndrome 21 Cri du chat syndrome (Chromosome 5p- synd) 16 Bardet-Biedl syndrome (Laurence Moon-Biedl) 15 Hurler syndrome (MPS I-H) 15 Crouzon syndrome (Craniofacial Dysotosis) 13 NF1 - Neurofibromatosis (von Recklinghausen dis) 13 Kniest Dysplasia 12 Turner syndrome 11 Usher III syndrome 10 Cockayne syndrome 9 Apert syndrome/Acrocephalosyndactyly, Type 1 8 Leigh Disease 8 Alport syndrome 6 Monosomy 10p 6 NF2 - Bilateral Acoustic Neurofibromatosis 6 Batten disease 5 Kearns-Sayre syndrome 5 Klippel-Feil sequence 5 Hereditary Syndromes and Disorders Count Prader-Willi 5 Sturge-Weber syndrome 5 Marfan syndrome 3 Hand-Schuller-Christian (Histiocytosis X) 2 Hunter Syndrome (MPS II) 2 Maroteaux-Lamy syndrome (MPS VI) 2 Morquio syndrome (MPS IV-B) 2 Optico-Cochleo-Dentate Degeneration 2 Smith-Lemli-Opitz (SLO) syndrome 2 Wildervanck syndrome 2 Herpes-Zoster (or Hunt) 1 Vogt-Koyanagi-Harada