30 Sep – External Eye
Periorbital Cellulitis – most common from bacterial infection Check vision and EOM (if EOM effected the has moved to the muscles) Tx – Antibiotic – IV & Oral
Chalazion – Hordeolum Hot compress
Malignancy Long history of non-healing ulceration or lesion
Blepharitis Scurf on eyelids with associated inflammation Itching, redness (3-6 months) Exam – “dandruff” on eyelashes Tx – Lid hygiene (warm cloth & baby shampoo)
Meibomian Gland Dysfunction Lipid tear film deficiency Risk factors – Rosacea Acutance therapy (White mark on the eye lid – on the glands) Tx – Lid Hygiene – warm compress
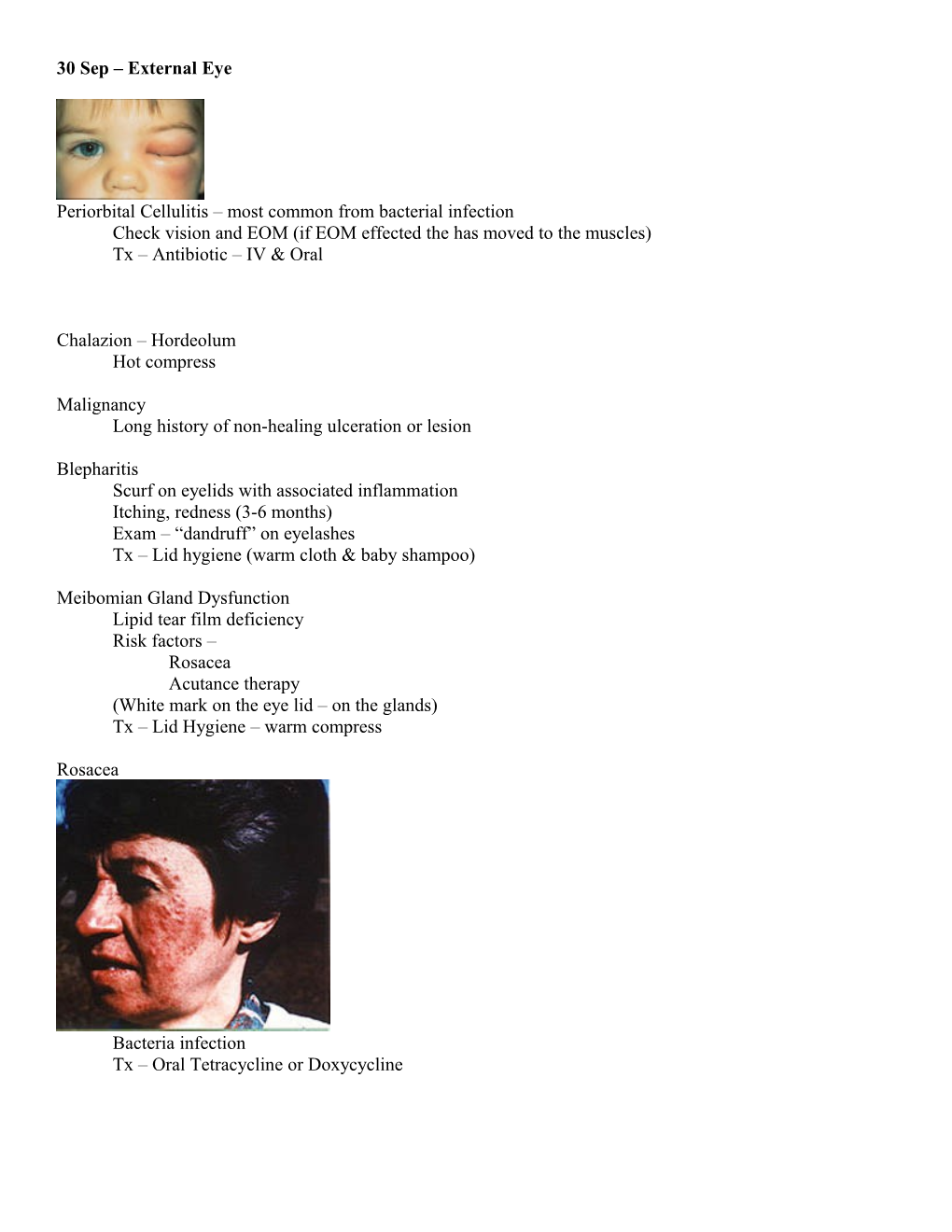
Rosacea
Bacteria infection Tx – Oral Tetracycline or Doxycycline Dry Eye Syndrome
Tear Film Aqueous Lipid - Symptoms - Dryness, irritation or dry eye sensation Meibomian gland dysfunction or tear deficiency
Tx- minimize topical medication Use artificial tears Topical Cyclosporine Meds can dry eye (BP meds, Psych, Decongestants & Antihistamine) Humidifier / Where glasses / avoid heating or AC
Conjunctivitis
Viral infection (most) – Bacterial (minimal) – Bacterial will have Purulent discharge / Viral will have clear discharge (can cause opacity in cornea)
Tx – Nothing / Bacterial can treat with Antibiotics Stay home 7-10 days (contagious) Giant Papillary Conjunctivitis
Immune response to contact lens
Tx – stop wearing contacts
Look under lids – Bumps
Corneal Ulcer
Pseudomonas
Infectious Keratitis Redness, pain, decrease vision, Common from Bacteria Herpes of the Cornea
- Anti Viral treatment
Corneal Abrasion Tx – Topical ointment (Antibiotic) (3-4 times a day for 3-4 days) Can patch if desired