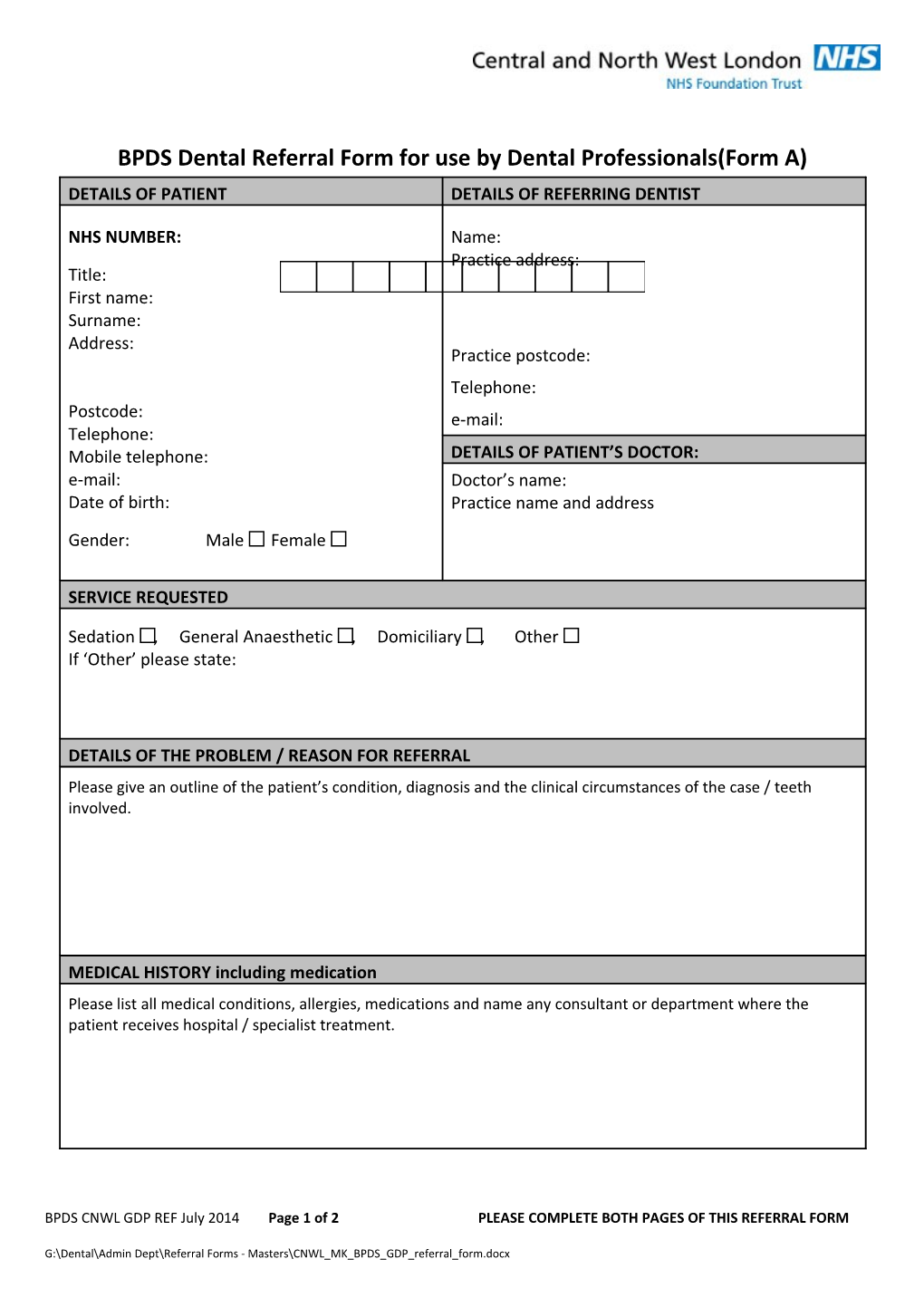
BPDS Dental Referral Form for use by Dental Professionals(Form A) DETAILS OF PATIENT DETAILS OF REFERRING DENTIST
NHS NUMBER: Name: Practice address: Title: First name: Surname: Address: Practice postcode: Telephone: Postcode: e-mail: Telephone: Mobile telephone: DETAILS OF PATIENT’S DOCTOR: e-mail: Doctor’s name: Date of birth: Practice name and address
Gender: Male Female
SERVICE REQUESTED
Sedation , General Anaesthetic , Domiciliary , Other If ‘Other’ please state:
DETAILS OF THE PROBLEM / REASON FOR REFERRAL Please give an outline of the patient’s condition, diagnosis and the clinical circumstances of the case / teeth involved.
MEDICAL HISTORY including medication Please list all medical conditions, allergies, medications and name any consultant or department where the patient receives hospital / specialist treatment.
BPDS CNWL GDP REF July 2014 Page 1 of 2 PLEASE COMPLETE BOTH PAGES OF THIS REFERRAL FORM
G:\Dental\Admin Dept\Referral Forms - Masters\CNWL_MK_BPDS_GDP_referral_form.docx DENTAL HISTORY Please include treatment undertaken or attempted to date and if any preventative advice given.
Radiographs attached: Yes No Relevant radiographs would be expected to be sent so If there are no attached radiographs, please explain why.
Digital radiographs can be emailed as a JPEG file to [email protected]: Tick if emailed Emailed radiographs should be patient non identifiable if not being sent from an NHS.NET email account. Please reference your emailed radiographs. REF No………………………………………………………………… Return items to the practice: No Yes SPECIAL REQUIREMENTS Interpreter needed: No Yes If ‘Yes’ please state language or if required for hearing impairment.
Hoist required: No Yes Any other special requirements:
Copy of referral given to patient: Yes No Signature: FP17RN attached Yes No (Mandatory for all NHS practices): Print Name Date: This form must be completed as fully as possible. Incomplete forms will be returned and may lead to delays.
For Office Use Only Date Received Processed by / Date
All referrals should be sent to: Postal and fax referrals to: Buckinghamshire Priority Dental Service, Brookside Centre, Station Way East, Aylesbury.HP20 2SR. 0844 2252411. Fax - 01296 566421 Email (from NHS.net address only): [email protected]
BPDS CNWL GDP REF July 2014 Page 2 of 2 PLEASE COMPLETE BOTH PAGES OF THIS REFERRAL FORM
G:\Dental\Admin Dept\Referral Forms - Masters\CNWL_MK_BPDS_GDP_referral_form.docx