THE BAROSSA COUNCIL
INCIDENT REPORT FORM
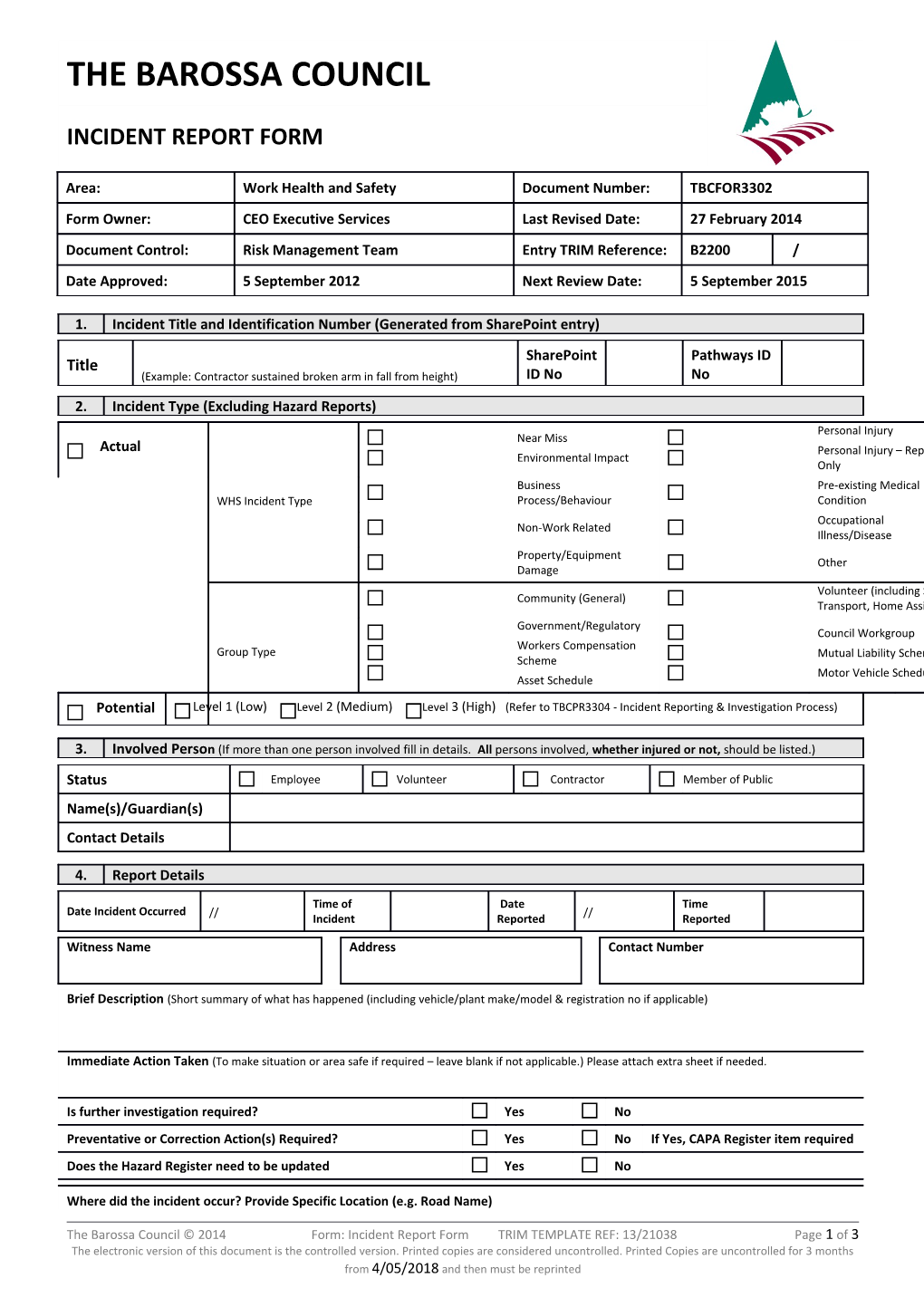
Area: Work Health and Safety Document Number: TBCFOR3302 Form Owner: CEO Executive Services Last Revised Date: 27 February 2014 Document Control: Risk Management Team Entry TRIM Reference: B2200 / Date Approved: 5 September 2012 Next Review Date: 5 September 2015
1. Incident Title and Identification Number (Generated from SharePoint entry) SharePoint Pathways ID Title (Example: Contractor sustained broken arm in fall from height) ID No No
2. Incident Type (Excluding Hazard Reports) Personal Injury Near Miss Actual Personal Injury – Report Environmental Impact Only Business Pre-existing Medical WHS Incident Type Process/Behaviour Condition Occupational Non-Work Related Illness/Disease Property/Equipment Other Damage Volunteer (including S41, Community (General) Transport, Home Assist) Government/Regulatory Council Workgroup Workers Compensation Group Type Mutual Liability Scheme Scheme Motor Vehicle Schedule Asset Schedule Potential Level 1 (Low) Level 2 (Medium) Level 3 (High) (Refer to TBCPR3304 - Incident Reporting & Investigation Process)
3. Involved Person (If more than one person involved fill in details. All persons involved, whether injured or not, should be listed.)
Status Employee Volunteer Contractor Member of Public Name(s)/Guardian(s) Contact Details
4. Report Details
Time of Date Time Date Incident Occurred // // Incident Reported Reported
Witness Name Address Contact Number
Brief Description (Short summary of what has happened (including vehicle/plant make/model & registration no if applicable)
Immediate Action Taken (To make situation or area safe if required – leave blank if not applicable.) Please attach extra sheet if needed.
Is further investigation required? Yes No Preventative or Correction Action(s) Required? Yes No If Yes, CAPA Register item required Does the Hazard Register need to be updated Yes No
Where did the incident occur? Provide Specific Location (e.g. Road Name)
The Barossa Council © 2014 Form: Incident Report Form TRIM TEMPLATE REF: 13/21038 Page 1 of 3 The electronic version of this document is the controlled version. Printed copies are considered uncontrolled. Printed Copies are uncontrolled for 3 months from 4/05/2018 and then must be reprinted Visitor Information Centre Depot Private Residence Library
Barossa Regional Gallery Roadway/Footpaths Refuse Tip Reserve/Park/Oval Council Office In Transit Swimming Pool Recreation Centre
Other
Hazard Type
Slip/Trip/Fall Falling Object Caught In Struck by Manual Handling Environmental conditions Harmful Contact/Exposure Recurrence
Stress/Anxiety Safe Act Observation A B C Other
Injury Type
Property/Environmental Fracture Internal Injury Burns Psychological Damage
Dislocation Open Wound Poisoning Exposure
Aggravation of previous Sprain/Strain Superficial Injury Multiple Injuries condition
Head Injury Eye Injury Rash/Dermatitis Other
Bruising Bite/Sting Currently Unknown NA
Affected Area Head Trunk System Arm Hand Leg Foot Property
Eye Neck Heart Left Left Left Left Council
Ear Hip Lungs Right Right Right Right Public
Nose Chest Circulatory Shoulder Thumb Knee Toe Environmental
Mouth Stomach Respiratory Upper Arm Fingers Lower Leg Foot Vehicle/Plant
Skull Upper back Nervous Forearm Hand Upper Leg Heel Other
Face Lower back Psychological Wrist Other Ankle
Ribs Digestive Elbow
Treatment Associated Services Outcome Associated Issues
No Treatment Police Nil - Report Only Motor Vehicle First Aid (on site) Claims Remainder of day (medical) Injury to other person(s)
Medical treatment Ambulance Unfit for work (LTI) Damage to property Doctor (Outpatient) Fire Unfit for a number of days (LTI) Environmental damage
Admitted to hospital SafeWork SA Modified duties Bullying/Harassment
Date and time if work ceased Name of First Aid Officer:
// @ am/pm
Notification Health & Safety Regional Risk Relevant Supervisor Risk Management Team Representative (HSR) Coordinator (RRC)
5. Notifiable Incident (Refer TBCPR3304 - Incident Reporting and Investigation Process)
Has this risk event resulted in a Notifiable Incident? Yes No
If Yes – the incident must be reported to SafeWork SA by the person in charge of the workplace (or delegate)
Date Reported // Reported By (print name)
6. Sign Offs
//
The Barossa Council © 2014 Form: Incident Report Form TRIM TEMPLATE REF: 13/21038 Page 2 of 3 The electronic version of this document is the controlled version. Printed copies are considered uncontrolled. Printed Copies are uncontrolled for 3 months from 4/05/2018 and then must be reprinted Name of Supervisor/Manager Signature Date
// Name of Person Involved in Incident Signature Date
The Barossa Council © 2014 Form: Incident Report Form TRIM TEMPLATE REF: 13/21038 Page 3 of 3 The electronic version of this document is the controlled version. Printed copies are considered uncontrolled. Printed Copies are uncontrolled for 3 months from 4/05/2018 and then must be reprinted