[Insert Contractor Letterhead Here]
SAFETY PLAN SERVICES (SPS) 15-DAY SUMMARY REPORT
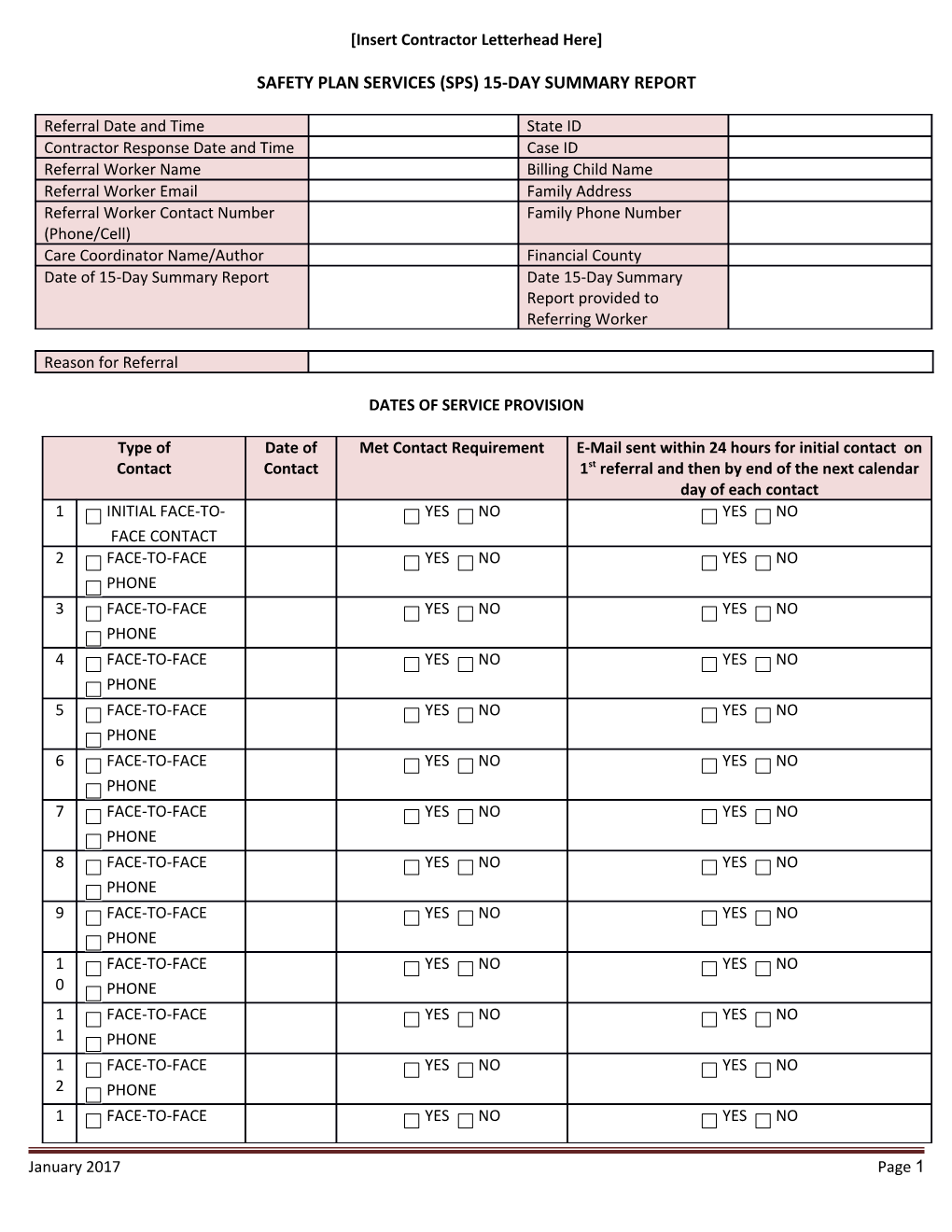
Referral Date and Time State ID Contractor Response Date and Time Case ID Referral Worker Name Billing Child Name Referral Worker Email Family Address Referral Worker Contact Number Family Phone Number (Phone/Cell) Care Coordinator Name/Author Financial County Date of 15-Day Summary Report Date 15-Day Summary Report provided to Referring Worker
Reason for Referral
DATES OF SERVICE PROVISION
Type of Date of Met Contact Requirement E-Mail sent within 24 hours for initial contact on Contact Contact 1st referral and then by end of the next calendar day of each contact 1 INITIAL FACE-TO- YES NO YES NO FACE CONTACT 2 FACE-TO-FACE YES NO YES NO PHONE 3 FACE-TO-FACE YES NO YES NO PHONE 4 FACE-TO-FACE YES NO YES NO PHONE 5 FACE-TO-FACE YES NO YES NO PHONE 6 FACE-TO-FACE YES NO YES NO PHONE 7 FACE-TO-FACE YES NO YES NO PHONE 8 FACE-TO-FACE YES NO YES NO PHONE 9 FACE-TO-FACE YES NO YES NO PHONE 1 FACE-TO-FACE YES NO YES NO 0 PHONE 1 FACE-TO-FACE YES NO YES NO 1 PHONE 1 FACE-TO-FACE YES NO YES NO 2 PHONE 1 FACE-TO-FACE YES NO YES NO
January 2017 Page 1 3 PHONE
1 FACE-TO-FACE YES NO YES NO 4 PHONE 1 FACE-TO-FACE YES NO YES NO 5 PHONE
Summary of Involvement
How were services culturally competent/responsive?
FTDM/YTDM Meeting Attendance YES NO N/A Date Court Hearing Attendance YES NO N/A Date Removal YES NO Date Was there another child abuse YES NO If yes, what NC C F UNK assessment initiated during was the provision of Safety Plan Services? outcome of NC – Not Confirmed the C – Confirmed, Not Placed assessment? F – Confirmed & Placed = Founded UNK – Unknown
Crisis Response YES NO If yes, describe
Flex Funds Expended YES NO If yes, amount and purpose $
Community Resources Engaged YES NO If yes, identify resources
Safety Constructs at Service Termination
Overall assessment of Threats of Maltreatment, Protective Capacities, Child Vulnerability, Underlying Conditions and Contributing Factors
January 2017 Page 2