Ministry of Local Government and Rural Development
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Eindhoven University of Technology MASTER Public Transport in Ghana
Eindhoven University of Technology MASTER Public transport in Ghana : assessment of opportunities to improve the capacity of the Kejetia public transport terminal in Kumasi, Ghana van Hoeven, Nathalie Award date: 1999 Link to publication Disclaimer This document contains a student thesis (bachelor's or master's), as authored by a student at Eindhoven University of Technology. Student theses are made available in the TU/e repository upon obtaining the required degree. The grade received is not published on the document as presented in the repository. The required complexity or quality of research of student theses may vary by program, and the required minimum study period may vary in duration. General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain ASSESSMENT OF OPPORTUNITIES TO IMPROVE THE CAPACITY OF THE KEJETIA PUBLIC TRANSPORT TERMINAL IN KUMASI, GHANA I APPENDICES N. van Hoeven December 1999 Supervisors Eindhoven University of Technology Drs. H. C.J.J. Gaiflard Ir. E.L.C. van Egmond-de Wilde de Ligny Faculty of Technology Management Department of International Technology and Development Studies Ir. A. W.J. Borgers Faculty of Building Engineering Department of Planning In co-operation with Dr. -

Press Release Shooting of the Pilgrims of Mpuasu
PRESS RELEASE SHOOTING OF THE PILGRIMS OF MPUASU-JAPEKROM TRADITIONAL AREA AT NEW DROBO AND THE SECURITY DEVELOPMENT IN THE JAMAN SOUTH MUNICIPALITY – NON-RESIDENTIAL CITIZENS OF MPUASUMAN- JAPEKROM TRADITIONAL AREA Ladies and Gentlemen of the Press, Good morning. We have called the attention of Ghanaians to a very serious security development in the Jaman South Municipal Area, specifically between Japekrom and New Drobo (Drobo). These matters resulted from the shooting of the Youth Chief of Japekrom and two other people, a Senior High School student and a one-year-old baby who were all part of a peaceful procession during the Celebration of the Munufie Festival by the People of the Mpuasu-Japekrom Traditional Area. 2. THE MUNUFIE FESTIVAL The activities marking the Annual Munufie Festival of the people of Mpuasu-Japekrom Traditional Area involved a visit to Mpuasu, the ancestral home of the people to perform a spiritual bath. This year’s activities involved the commemoration of our ancestral journey, a showcase of the coming and settlement of the people of Mpuasu-Japekrom in present day Japekrom. This event, which took place on 17th October, 2018, takes place every 5 decades (50 years) and it involves walking on foot from Krobuo on the main Japekrom-Sampa road to Japekrom. Over 1000 residents and non-residents of the Traditional Area, including men, women, young, old and children participated in the historic walk. Unfortunately, this peaceful walk ended in bloodshed. Unknown assailants fired gunshot from a storey-building at the roadside (eyewitness and police accounts) into the crowd, killing three (3), including a one year old baby. -

Greater Accra Region
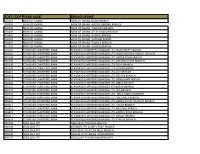
NATIONAL COMMUNICATIONS AUTHORITY LIST OF AUTHORISED VHF-FM RADIO STATIONS IN GHANA AS AT FOURTH QUARTER, 2013 Last updated on the 30th December, 2013 1 NATIONAL COMMUNICATIONS AUTHORITY LIST OF FM STATIONS IN THE COUNTRY AS AT FOURTH QUARTER, 2013 NO. NAME OF TOTAL NO. PUBLIC COMMUN CAMPUS COMMER TOTAL TOTAL REGIONS AUTHORIS ITY CIAL NO. IN NO. NOT ED OPERATI IN ON OPERATI ON 1. Greater Accra 47 5 6 3 33 42 5 2. Ashanti 47 3 4 2 38 41 6 3. Brong Ahafo 45 3 4 0 38 38 7 4. Western 52 6 4 1 39 37 15 5. Central 27 2 7 3 15 22 5 6. Eastern 29 2 5 1 21 26 3 7. Volta 34 3 7 1 23 24 10 8. Northern 30 7 10 0 13 20 10 9. Upper East 13 2 3 1 7 10 3 10. Upper West 15 3 8 1 3 7 8 Total 339 36 58 13 232 267 74 Last updated on the 30th December, 2013 2 GREATER ACCRA REGION S/N Name and Address of Date of Assigned On Air Not Location (Town Type of Station Company Authorisation Frequency on Air /City) 1. MASCOTT MULTI- 13 – 12 – 95 87.9MHz On Air Accra Commercial FM SERVICES LIMITED. (ATLANTIS RADIO) Box PMB CT 106, Accra Tel: 0302 7011212/233308 Fax:0302 230871 Email: 2. NETWORK 7 - 09 – 95 90.5MHz On Air Accra Commercial FM BROADCASTING LIMITED (RADIO GOLD) Box OS 2723,OSU Accra Tel:0302-300281/2 Fax: 0302-300284 Email:[email protected] m 3. -

Yvonne B. Egyin Thesis.Pdf
KWAMME NKRUMAH UNIVERSITY OF SCIENCE AND TECHNOLOGY, KUMASI INSTITUTE OF DISTANCE LEARNING AN ASSESSMENT OF THE SERVICE DELIVERY OF GWCL/AQUA VITANS: A CASE STUDY OF THE SUNYANI MUNICIPALITY YVONNE BATHSHEBA EGYIN B. Sc (Admin) July, 2011 KWAMME NKRUMAH UNIVERSITY OF SCIENCE AND TECHNOLOGY, KUMASI INSTITUTE OF DISTANCE LEARNING AN ASSESSMENT OF THE SERVICE DELIVERY OF GWCL/AQUA VITANS: A CASE STUDY OF THE SUNYANI MUNICIPALITY BY YVONNE BATHSHEBA EGYIN B. Sc (Admin) A DISSERTATION SUBMITTED TO THE INSTITUTE OF DISTANCE LEARNING, KWAME NKRUMAH UNIVERSITY OF SCIENCE AND TECHNOLOGY, KUMASI, IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE DEGREE OF MASTER OF BUSINESS ADMINISTRATION (CEMBA) DEGREE JULY, 2011 DECLARATION I hereby declare that this submission is my own work towards the CEMBA and that, to the best of my knowledge, it contains no material previously published by another person nor material which has been accepted for the award of any other degree of the university, except where due acknowledgement has been made in the text. YVONNE BATHSHEBA EGYIN ________________ _____ (PG 3060309) Signature Date Certified by: Mr. Jones Lewis Arthur _______________ _____ (Principal Supervisor) Signature Date Certified by: ________________ _____ (Head of Department) Signature Date DEDICATION I dedicate this work to God Almighty, my husband, Mr. Kodwo Boakye Egyin, Mr. Jones Lewis Arthur, and my children Kow, Araba and Kurankwesi through whose sacrifice, support and encouragement I have come this far. ABSTRACT The water supply and sanitation sector in Ghana faces severe problems, partly due to a neglect of the sector until the 1990s. Tariffs were kept at a low level which was far from reflecting the real cost of the service. -

2017 Almanac Final Final.Cdr
THE METHODIST CHURCH GHANA CONFERENCE OFFICE, WESLEY HOUSE E252/2, LIBERIA ROAD P. O. BOX GP 403, ACCRA, TEL: 0302 670355 / 679223 WEBSITE: www.methodistchurch_gh.org Email: [email protected] PRESIDING BISHOP: THE MOST REV. TITUS K. AWOTWI PRATT, BA, MA LAY PRESIDENT: MR. KWAME AGYAPONG BOAFO, BA (HONS.), Q.C.L., BL. ADMINISTRATIVE BISHOP: THE RT REV. DR. PAUL KWABENA BOAFO, BA., PhD. DIOCESES BISHOPS LAY CHAIRMEN SYNOD SECRETARIES CAPE COAST The Rt. Rev. Ebenezer K. Abaka-Wilson, BA, MEd Bro. Titus D. Essel Very Rev. Richardson Aboagye Andam, BA MPhil ACCRA The Rt. Rev. Samuel K. Osabutey, BA., MA., PEM (ADR) Bro. Joseph K. Addo, CA, MBA Very Rev. Sampson N. A. M. Laryea Adjei, BTh KUMASI The Rt. Rev. Christopher N. Andam, BA., MSc., MBA Bro. Prof. Seth Opuni Asiama, BSc., PhD Very Rev. Stephen K. Owusu, BD, ThM, MPhil SEKONDI The Rt. Rev. Daniel De-Graft Brace, BA., MA Bro. George Tweneboah-Kodua, BEd, MSc Very Rev. Comfort Quartey-Papafio, MTS., ThM WINNEBA The Rt. Rev. Dr. J. K. Buabeng-Odoom, BEd., MEd., DMin Bro. Nicholas Taylor, BEd, MEd Very Rev. Joseph M. Ossei, BA., MPhil KOFORIDUA The Rt. Rev. Michael Agyakwa Bossman, BA., MPhil Bro. Samuel B. Mensah Jnr., BEd Very Rev. Samual Dua Dodd, BTh., D.Min SUNYANI The Rt. Rev. Kofi Asare Bediako, BA., MSc Sis. Grace Amoako Very Rev. Daniel K. Tannor, BA, MPhil TARKWA The Rt. Rev. Thomas Amponsah-Donkor, BA., LLB, BL Bro. Joseph K. Amponsah, BEd Very Rev. Nicholas Odum Baido, BA., MA NORTHERN GHANA The Rt. Rev. Dr. -

Brong Ahafo Region
CERTIFIED ELECTRICAL WIRING PROFESSIONALS REGISTER- BRONG AHAFO REGION ENERGY COMMISSION THIS DOCUMENT IS VALID TILL JUNE 2017 CERTIFICATION NAME SPECIFIC LOCATION PHONE NUMBER CLASS 1 ABDEEN HASSAN WENCHI +233208435255 DOMESTIC 2 ABDULAI-BABA LOSINA WATARA WENCHI +233208306812 DOMESTIC 3 ABOAGYE ERIC WENCHI +233209097188 DOMESTIC 4 ABOAGYE SOLOMON NTOFROSO-GYEDU, BRONG AHAFO +233245132173 DOMESTIC 5 ABREFAH NOAH TECHIMAN 233246840008 DOMESTIC 6 ABU SADIQUE TECHIMAN +233208430808 DOMESTIC 7 ACHEAMPONG ERNEST KWABENA DUAYAW KKWANTIA BRONG AHAFO +233208589610 DOMESTIC 8 ACHIANGBON KWABLA TECHIMAN +233543577329 DOMESTIC 9 ADAMA ISSAKA BEREKUM +233208392240 DOMESTIC 10 ADDAI KOFI MARTIN TECHIMAN +233246312473 DOMESTIC 11 ADDAI STEPHEN JUSTICE GOASO, BRONG AHAFO +233249886038 DOMESTIC 12 ADDAI THOMAS KWAME SUNYANI +233209255172 DOMESTIC 13 ADDO BISMARK ABESIM +233208409541 DOMESTIC 14 ADDO JOSEPH DROBO +233246988356 DOMESTIC 15 ADDO NANA MIKE WENCHI +233506150373 DOMESTIC 16 ADDO SAMUEL DANSO KENYASI +233541184064 DOMESTIC 17 ADDOM EDWARD KWADWO SUNYANI +233208246058 INDUSTRIAL 18 ADJEI DAVID SUNYANI +233248611681 DOMESTIC 19 ADJEI KWADWO SAMUEL DORMAA WEST +233242863447 COMMERCIAL 20 ADOM KWASI EMMANUEL BEREKUM +233208169881 COMMERCIAL 21 ADOMAH KWADWO ABRAHAM DROBO +233242870092 DOMESTIC 22 ADOMAH SAMUEL SUNYANI +233209059586 DOMESTIC 23 ADU AMANFO EMMANUEL DUAYAW-NKWANTA +233243141355 DOMESTIC 24 ADU EDWARD SARKODIE KENYASI +233243289256 DOMESTIC 25 ADU JOSHUA BRONG AHAFO REGION,TECHIMAN +233245400900 DOMESTIC 26 ADU PAUL GOASO,BRONG AHAFO -

Compilation of Telephone Directory with Addresses
TABLE OF CONTENTS PAGE 1.0 Address and Telephone No.s for ARB Apex Bank Ltd. 2 2.0 Address and Telephone No.s Association of Rural Banks 3 3.0 Addresses and Telephone No.s of RCBs 5 - 4.0 Other useful information 5.0 Index 1 | P a g e ARB APEX BANK LIMITED 1. ARB APEX BANK LTD +233(0)302 – 771738 HEAD OFFICE 772129 P. O. Box GP 20321 772034 Accra FAX: Location: No. 5, 9 th Gamel Abdul Naser Avenue, +233(0)302 – 772260 South Ridge Accra Email: [email protected] 2. ACCRA BRANCH 0302 - 770811 Location: No. 5, 9 th Gamel Abdul Naser Avenue, South Ridge Accra 3. COCOA HOUSE 030 -2677993 Location: Ground Floor, Cocoa House, Accra 030-2678000 030-2677998 4. BOLGATANGA BRANCH 038-2024483 Location: Alhaji Danladi Palace No. 2, 038-2024027 Address: P. O. Box 619 Bolgatanga 038-2023309 (Fax) 5. KOFORIDUA CLEARING CENTRE 0342 – 022913 Location: 1 ST Floor, South Akim RBL Koforidua 0342 – 020003 Agency Telefax: Address: Private Mail Bag Koforidua 0342 – 020004 6. KUMASI BRANCH 03220 – 40990 Location: Near Ahodwo Roundabout 40992 Address: P. O. Box 14745 Kumasi 40993 7. SUNYANI CLEARING CEN TRE 03520 – 24461 Location: Opposite Sunyani Polytechnic 28930 Address: P. O. Box 1987, Sunyani 28931 Fax: (0)3520 – 28932 8. TAKORADI BRANCH (0)3120 – 92011/4 Location: SSNIT Office Complex Building near Bank 92012/3 of Ghana Offices, Takoradi Address: P. O. Box AX 573 Takoradi 9. TAMALE BRANCH 03720 – 23119 Location: Opposite Ola Cathedral Off Teaching Hospital Address: P. O. Box TL 997 Tamale 10. -

GES-SHS-Selection-REGISTER-2019
CATEGORY A PROGRAMMES NO. SCHOOL AGRI HOM. VIS. GEN. GEN. OF S/N REGION DISTRICT SCHOOL NAME LOCATION GENDER BUS TECH STATUS CODE C ECONS ARTS ARTS SCI PROG S 101 201 301 401 402 501 502 1 AHAFO Asutifi North 0061201 OLA Girls Senior High, Kenyasi Kenyasi Girls X X X X 4 Day/Boarding 2 AHAFO Tano North 0060203 Serwaa Kesse Girls Senior High Duayaw Nkwanta Girls X X X X X X 6 Day/Boarding 3 ASHANTI Kumasi Metro 0050102 St. Louis Senior High, Kumasi Oduom-Kumasi Girls X X X X X 5 Day/Boarding 4 ASHANTI Kumasi Metro 0050111 Kumasi Senior High Gyinyase-Kumasi Boys X X X X X 5 Day/Boarding 5 ASHANTI Kumasi Metro 0050110 Opoku Ware Senior High Santasi-Kumasi Boys X X X X 4 Day/Boarding 6 ASHANTI Kumasi Metro 0050108 Prempeh College Sofoline-Kumasi Boys X X X X 4 Day/Boarding 7 ASHANTI Kumasi Metro 0050104 T. I. Ahmadiyya Senior High , Kumasi Kumasi - Stadium Mixed X X X X X X 6 Day/Boarding 8 ASHANTI Kumasi Metro 0050201 Yaa Asantewaa Girls Senior High . Tanoso-Kumasi Girls X X X X X X 6 Day/Boarding 9 B. AHAFO Berekum-Municipal 0060303 Berekum Presby Senior High Berekum Mixed X X X X X X 6 Day/Boarding 10 B. AHAFO Jaman North 0060513 St. Ann's Girls Senior High, Sampa Sampa Girls X X 2 Day 11 B. AHAFO Jaman South 0060505 Our Lady of Providence Senior High Kwasi Buokrom Girls X X X X 4 Day/Boarding 12 B. -
Sort Code Bank Name Branch Name
SORT CODE BANK NAME BRANCH NAME 010101 BANK OF GHANA BANK OF GHANA ACCRA BRANCH 010303 BANK OF GHANA BANK OF GHANA -AGONA SWEDRU BRANCH 010401 BANK OF GHANA BANK OF GHANA -TAKORADI BRANCH 010402 BANK OF GHANA BANK OF GHANA -SEFWI BOAKO BRANCH 010601 BANK OF GHANA BANK OF GHANA -KUMASI BRANCH 010701 BANK OF GHANA BANK OF GHANA -SUNYANI BRANCH 010801 BANK OF GHANA BANK OF GHANA -TAMALE BRANCH 011101 BANK OF GHANA BANK OF GHANA - HOHOE BRANCH 020101 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-HIGH STREET BRANCH 020102 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD- INDEPENDENCE AVENUE BRANCH 020104 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-LIBERIA ROAD BRANCH 020105 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-OPEIBEA HOUSE BRANCH 020106 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-TEMA BRANCH 020108 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-LEGON BRANCH 020112 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-OSU BRANCH 020118 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-SPINTEX BRANCH 020121 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-DANSOMAN BRANCH 020126 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD-ABEKA BRANCH 020127 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH)-ACHIMOTA BRANCH 020129 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD- NIA BRANCH 020132 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD- TEMA HABOUR BRANCH 020133 STANDARD CHARTERED BANK STANDARD CHARTERED BANK(GH) LTD- WESTHILLS BRANCH 020436 -

Office of Government Machinery
REPUBLIC OF GHANA MEDIUM TERM EXPENDITURE FRAMEWORK (MTEF) FOR 2021-2024 OFFICE OF GOVERNMENT MACHINERY PROGRAMME BASED BUDGET ESTIMATES For 2021 Transforming Ghana Beyond Aid REPUBLIC OF GHANA Finance Drive, Ministries-Accra Digital Address: GA - 144-2024 MB40, Accra - Ghana +233 302-747-197 [email protected] mofep.gov.gh Stay Safe: Protect yourself and others © 2021. All rights reserved. No part of this publication may be stored in a retrieval system or Observe the COVID-19 Health and Safety Protocols transmitted in any or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior written permission of the Ministry of Finance Get Vaccinated OFFICE OF GOVERNMENT MACHINERY The OGM MTEF PBB for 2021 is also available on the internet at: www.mofep.gov.gh ii | 2021 BUDGET ESTIMATES Contents PART A: STRATEGIC OVERVIEW OF THE OFFICE OF GOVERNMENT MACHINERY (OGM) ................................................................................................... 2 1. POLICY OBJECTIVES ..................................................................................... 2 2. GOAL ................................................................................................................ 2 3. CORE FUNCTIONS .......................................................................................... 2 4. POLICY OUTCOME INDICATORS AND TARGETS ....................................... 3 POLICY OUTCOME INDICATORS AND TARGETS (MINISTRY OF SPECIAL INITIATIVE AND DEVELOPMENT) ..................................................................... -

Staff-ID-For-Bono
BRONG AHAFO-1607 S/N STAFF ID FULL_NAME MANAGEMENT_UNIT DISTRICT 1 1417193 FOSUAA, Mrs. JEMIMA 0725 Bongase DA KG & Prim Banda 2 1417184 TETTEH, Mr. ISAAC KWESI 0725 Bongase DA KG & Prim Banda 3 1417178 ANDAMAH, Mr. MUSAH 0725 Dorbor DA Prim Banda 4 1417183 ABIIKARO, Mrs. BARBARA 0725 Banda-AhenkroGbao DA Prim Dist Educ Banda 5 1417189 AFRIYIE, Miss MAVIS 0725Office Banda-Ahenkro Dist Educ Banda 6 1417199 KYERAA, Mrs. RITA 0725Office Banda-Ahenkro Dist Educ Banda 7 1417174 ASIEDU, Mr. PRINCE Office Banda 0725 Bandaman Senior High Tech 8 1416532 NSIAH ABABIO, Mrs. GLORIA 0725Sch Bandaman Senior High Tech Banda 9 1416539 BOAKYE, Mr. ERIC 0725Sch Bandaman Senior High Tech Banda 10 1416544 BEKOE, Mr. RICHARD 0725Sch Bandaman Senior High Tech Banda 11 1416521 BOATENG, Mr. SAMUEL 0725Sch Bandaman Senior High Tech Banda 12 1416550 MOSES, Mr. SIE KWAKU Sch Banda BOAMPONG, Mr. RICHARD 0725 Bandaman Senior High Tech 13 1416534 ANOMAH Sch Banda 0725 Bandaman Senior High Tech 14 1416527 GYAMFI, Mr. MICHAEL KWASI 0725Sch Bandaman Senior High Tech Banda 15 1416524 ASIEDU, Mr. MICHAEL Sch Banda 16 1417169 OBENG, Mr. ISAAC BOATENG 0725 Sanwa Makala DA Prim Banda 17 1417225 KYEREH, Mr. STEPHEN 0725 Sanwa Makala DA Prim Banda 18 1417216 FUSENI, Miss MUNIRATU 0725 Banda Ahenkro Meth Prim Banda 19 1417214 TIEREOFAA, Mr. MWINKUM 0725 Banda Ahenkro Meth Prim Banda 20 1417220 BOSEAH, Mr. MOSES 0725 Banda Ahenkro Presby Prim Banda 21 1417208 ASANTE, Mr. MICHAEL 0725 Banda Ahenkro Presby Prim Banda OSEI, Mr. ORPHEAUS 22 1417204 SARPONG 0725 Kojee Presby Prim Banda Berekum Municipal 23 1418346 WEJENAKA, Miss RITA 0705 Amomaso MA Prim (GOV) Assembly Berekum NINFAM, Mr. -
National Communications Authority List Of
NATIONAL COMMUNICATIONS AUTHORITY LIST OF AUTHORISED VHF-FM RADIO STATIONS IN GHANA AS AT SECOND QUARTER, 2017 Page 1 of 82 OVERVIEW OF FM RADIO BROADCASTING STATIONS IN GHANA Section 2 of the Electronic Communications Act, 2008, Act 775 mandates that the National Communications Authority “shall regulate the radio spectrum designated or allocated for use by broadcasting organisations and providers of broadcasting services”; “… determine technical and other standards and issue guidelines for the operation of broadcasting organisations …” “… may adopt policies to cater for rural communities and for this purpose may waive fees wholly or in part for the grant of a frequency authorisation”. The Broadcasting service is a communication service in which the transmissions are intended for direct reception by the general public. The sound broadcasting service involves the broadcasting of sound which may be accompanied by associated text/data. Sound broadcasting is currently deployed in Ghana using analogue transmission techniques: Amplitude Modulation (AM) and Frequency Modulation (FM). Over the last two decades, AM sound broadcasting has faded, leaving FM radio as the only form of sound broadcasting in Ghana. FM radio broadcasting stations are classified for the purpose of regulatory administration of the service towards the attainment of efficient use of frequency. The following is the classification of FM radio broadcasting stations in Ghana. (1) Classification by Purpose: a) Public – all stations owned and operated by the Ghana Broadcasting Corporation (GBC) and/or any other station established by the Government of Ghana by a statutory enactment. b) Public Foreign – stations established by Foreign Governments through diplomatic arrangements to rebroadcast/relay content from foreign countries e.g.