Recurrent Targetoid Hemosiderotic Hemangioma in a 26-Year-Old Man
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tumors and Tumor-Like Lesions of Blood Vessels 16 F.Ramon
16_DeSchepper_Tumors_and 15.09.2005 13:27 Uhr Seite 263 Chapter Tumors and Tumor-like Lesions of Blood Vessels 16 F.Ramon Contents 42]. There are two major classification schemes for vas- cular tumors. That of Enzinger et al. [12] relies on 16.1 Introduction . 263 pathological criteria and includes clinical and radiolog- 16.2 Definition and Classification . 264 ical features when appropriate. On the other hand, the 16.2.1 Benign Vascular Tumors . 264 classification of Mulliken and Glowacki [42] is based on 16.2.1.1 Classification of Mulliken . 264 endothelial growth characteristics and distinguishes 16.2.1.2 Classification of Enzinger . 264 16.2.1.3 WHO Classification . 265 hemangiomas from vascular malformations. The latter 16.2.2 Vascular Tumors of Borderline classification shows good correlation with the clinical or Intermediate Malignancy . 265 picture and imaging findings. 16.2.3 Malignant Vascular Tumors . 265 Hemangiomas are characterized by a phase of prolif- 16.2.4 Glomus Tumor . 266 eration and a stationary period, followed by involution. 16.2.5 Hemangiopericytoma . 266 Vascular malformations are no real tumors and can be 16.3 Incidence and Clinical Behavior . 266 divided into low- or high-flow lesions [65]. 16.3.1 Benign Vascular Tumors . 266 Cutaneous and subcutaneous lesions are usually 16.3.2 Angiomatous Syndromes . 267 easily diagnosed and present no significant diagnostic 16.3.3 Hemangioendothelioma . 267 problems. On the other hand, hemangiomas or vascular 16.3.4 Angiosarcomas . 268 16.3.5 Glomus Tumor . 268 malformations that arise in deep soft tissue must be dif- 16.3.6 Hemangiopericytoma . -

Vascular Tumors and Malformations of the Orbit
14 Vascular Tumors Kaan Gündüz and Zeynel A. Karcioglu ascular tumors and malformations of the orbit VIII related antigen (v,w,f), CV141 (endothelium, comprise an important group of orbital space- mesothelium, and squamous cells), and VEGFR-3 Voccupying lesions. Reviews indicate that vas- (channels, neovascular endothelium). None of the cell cular lesions account for 6.2 to 12.0% of all histopatho- markers is absolutely specific in its application; a com- logically documented orbital space-occupying lesions bination is recommended in difficult cases. CD31 is (Table 14.1).1–5 There is ultrastructural and immuno- the most often used endothelial cell marker, with pos- histochemical evidence that capillary and cavernous itive membrane staining pattern in over 90% of cap- hemangiomas, lymphangioma, and other vascular le- illary hemangiomas, cavernous hemangiomas, and an- sions are of different nosologic origins, yet in many giosarcomas; CD34 is expressed only in about 50% of patients these entities coexist. Hence, some prefer to endothelial cell tumors. Lymphangioma pattern, on use a single umbrella term, “vascular hamartomatous the other hand, is negative with CD31 and CD34, lesions” to identify these masses, with the qualifica- but, it is positive with VEGFR-3. VEGFR-3 expression tion that, in a given case, one tissue element may pre- is also seen in Kaposi sarcoma and in neovascular dominate.6 For example, an “infantile hemangioma” endothelium. In hemangiopericytomas, the tumor may contain a few caverns or intertwined abnormal cells are typically positive for vimentin and CD34 and blood vessels, but its predominating component is negative for markers of endothelia (factor VIII, CD31, usually capillary hemangioma. -

Benign Hemangiomas
TUMORS OF BLOOD VESSELS CHARLES F. GESCHICKTER, M.D. (From tke Surgical Palkological Laboratory, Department of Surgery, Johns Hopkins Hospital and University) AND LOUISA E. KEASBEY, M.D. (Lancaster Gcaeral Hospital, Lancuster, Pennsylvania) Tumors of the blood vessels are perhaps as common as any form of neoplasm occurring in the human body. The greatest number of these lesions are benign angiomas of the body surfaces, small elevated red areas which remain without symptoms throughout life and are not subjected to treatment. Larger tumors of this type which undergb active growth after birth or which are situated about the face or oral cavity, where they constitute cosmetic defects, are more often the object of surgical removal. The majority of the vascular tumors clinically or pathologically studied fall into this latter group. Benign angiomas of similar pathologic nature occur in all of the internal viscera but are most common in the liver, where they are disclosed usually at autopsy. Angiomas of the bone, muscle, and the central nervous system are of less common occurrence, but, because of the symptoms produced, a higher percentage are available for study. Malignant lesions of the blood vessels are far more rare than was formerly supposed. An occasional angioma may metastasize following trauma or after repeated recurrences, but less than 1per cent of benign angiomas subjected to treatment fall into this group. I Primarily ma- lignant tumors of the vascular system-angiosarcomas-are equally rare. The pathological criteria for these growths have never been ade- quately established, and there is no general agreement as to this par- ticular form of tumor. -

Mesenchymal) Tissues E
Bull. Org. mond. San 11974,) 50, 101-110 Bull. Wid Hith Org.j VIII. Tumours of the soft (mesenchymal) tissues E. WEISS 1 This is a classification oftumours offibrous tissue, fat, muscle, blood and lymph vessels, and mast cells, irrespective of the region of the body in which they arise. Tumours offibrous tissue are divided into fibroma, fibrosarcoma (including " canine haemangiopericytoma "), other sarcomas, equine sarcoid, and various tumour-like lesions. The histological appearance of the tamours is described and illustrated with photographs. For the purpose of this classification " soft tis- autonomic nervous system, the paraganglionic struc- sues" are defined as including all nonepithelial tures, and the mesothelial and synovial tissues. extraskeletal tissues of the body with the exception of This classification was developed together with the haematopoietic and lymphoid tissues, the glia, that of the skin (Part VII, page 79), and in describing the neuroectodermal tissues of the peripheral and some of the tumours reference is made to the skin. HISTOLOGICAL CLASSIFICATION AND NOMENCLATURE OF TUMOURS OF THE SOFT (MESENCHYMAL) TISSUES I. TUMOURS OF FIBROUS TISSUE C. RHABDOMYOMA A. FIBROMA D. RHABDOMYOSARCOMA 1. Fibroma durum IV. TUMOURS OF BLOOD AND 2. Fibroma molle LYMPH VESSELS 3. Myxoma (myxofibroma) A. CAVERNOUS HAEMANGIOMA B. FIBROSARCOMA B. MALIGNANT HAEMANGIOENDOTHELIOMA (ANGIO- 1. Fibrosarcoma SARCOMA) 2. " Canine haemangiopericytoma" C. GLOMUS TUMOUR C. OTHER SARCOMAS D. LYMPHANGIOMA D. EQUINE SARCOID E. LYMPHANGIOSARCOMA (MALIGNANT LYMPH- E. TUMOUR-LIKE LESIONS ANGIOMA) 1. Cutaneous fibrous polyp F. TUMOUR-LIKE LESIONS 2. Keloid and hyperplastic scar V. MESENCHYMAL TUMOURS OF 3. Calcinosis circumscripta PERIPHERAL NERVES II. TUMOURS OF FAT TISSUE VI. -

Head and Neck Kaposi Sarcoma: Clinicopathological Analysis of 11 Cases
Head and Neck Pathology https://doi.org/10.1007/s12105-018-0902-x ORIGINAL PAPER Head and Neck Kaposi Sarcoma: Clinicopathological Analysis of 11 Cases Abbas Agaimy1 · Sarina K. Mueller2 · Thomas Harrer3 · Sebastian Bauer4 · Lester D. R. Thompson5 Received: 24 January 2018 / Accepted: 26 February 2018 © Springer Science+Business Media, LLC, part of Springer Nature 2018 Abstract Kaposi sarcoma (KS) of the head and neck area is uncommon with limited published case series. Our routine and consulta- tion files were reviewed for histologically and immunohistochemically proven KS affecting any cutaneous or mucosal head and neck site. Ten males and one female aged 42–78 years (median, 51 years; mean, 52 years) were retrieved. Eight patients were HIV-positive and three were HIV-negative. The affected sites were skin (n = 5), oral/oropharyngeal mucosa (n = 5), and lymph nodes (n = 3) in variable combination. The ear (pinna and external auditory canal) was affected in two cases; both were HIV-negative. Multifocal non-head and neck KS was reported in 50% of patients. At last follow-up (12–94 months; median, 46 months), most of patients were either KS-free (n = 8) or had ongoing remission under systemic maintenance therapy (n = 2). One patient was alive with KS (poor compliance). Histopathological evaluation showed classical features of KS. One case was predominantly sarcomatoid with prominent inflammation mimicking undifferentiated sarcoma. Immunohisto- chemistry showed consistent expression of CD31, CD34, ERG, D2-40 and HHV8 in all cases. This is one of the few series devoted to head and neck KS showing high prevalence of HIV-positivity, but also unusual presentations in HIV-negative patients with primary origin in the skin of the ear and the auditory canal. -

Dermatologic Aspects of Fabry Disease ª the Author(S) 2016 DOI: 10.1177/2326409816661353 Iem.Sagepub.Com
Original Article Journal of Inborn Errors of Metabolism & Screening 2016, Volume 4: 1–7 Dermatologic Aspects of Fabry Disease ª The Author(s) 2016 DOI: 10.1177/2326409816661353 iem.sagepub.com Paula C. Luna, MD1,2, Paula Boggio, MD2, and Margarita Larralde, MD, PhD1,2 Abstract Isolated angiokeratomas (AKs) are common cutaneous lesions, generally deemed unworthy of further investigation. In contrast, diffuse AKs should alert the physician to a possible diagnosis of Fabry disease (FD). Angiokeratomas often do not appear until adolescence or young adulthood. The number of lesions and the extension over the body increase progressively with time, so that generalization and mucosal involvement are frequent. Although rare, FD remains an important diagnosis to consider in patients with AKs, with or without familial history. Dermatologists must have a high index of suspicion, especially when skin features are associated with other earlier symptoms such as acroparesthesia, hypohidrosis, or heat intolerance. Once the diagnosis is established, prompt screening of family members should be performed. In all cases, a multidisciplinary team is necessary for the long-term follow-up and treatment. Keywords Fabry disease, angiokeratomas, lysosomal storage disorders Introduction Diffuse AKs are characterized by the presence of multiple lesions that affect more than 1 area of the skin. Although any Fabry disease (FD, also known as Anderson-Fabry disease or region of the skin can be affected, lesions usually localize to the angiokeratoma corporis diffusum [ACD]) is a rare X-linked bathing suit area (from the umbilicus to the upper thighs); this disease caused by the partial or complete deficiency of a lyso- phenotype is known as ACD. -

Kaposiform Hemangioendothelioma in Tonsil of a Child
Rekhi et al. World Journal of Surgical Oncology 2011, 9:57 http://www.wjso.com/content/9/1/57 WORLD JOURNAL OF SURGICAL ONCOLOGY CASEREPORT Open Access Kaposiform hemangioendothelioma in tonsil of a child associated with cervical lymphangioma: a rare case report Bharat Rekhi1*, Shweta Sethi1, Suyash S Kulkarni2 and Nirmala A Jambhekar1 Abstract Kaposiform hemangioendothelioma (KHE) is an uncommon vascular tumor of intermediate malignant potential, usually occurs in the extremities and retroperitoneum of infants and is characterized by its association with lymphangiomatosis and Kasabach-Merritt phenomenenon (KMP) in certain cases. It has rarely been observed in the head and neck region and at times, can present without KMP. Herein, we present an extremely uncommon case of KHE occurring in tonsil of a child, associated with a neck swelling, but unassociated with KMP. A 2-year-old male child referred to us with history of sore throat, dyspnoea and right-sided neck swelling off and on, since birth, was clinicoradiologically diagnosed with recurrent tonsillitis, including right sided peritonsillar abscess, for which he underwent right-sided tonsillectomy, elsewhere. Histopathological sections from the excised tonsillar mass were reviewed and showed a tumor composed of irregular, infiltrating lobules of spindle cells arranged in kaposiform architecture with slit-like, crescentic vessels. The cells displayed focal lumen formation containing red blood cells (RBCs), along with platelet thrombi and eosinophilic hyaline bodies. In addition, there were discrete foci of several dilated lymphatic vessels containing lymph and lymphocytes. On immunohistochemistry (IHC), spindle cells were diffusely positive for CD34, focally for CD31 and smooth muscle actin (SMA), the latter marker was mostly expressed around the blood vessels. -

Giant Cavernous Hepatic Hemangioma Diagnosed Incidentally in a Perimenopausal Obese Female with Endometrial Adenocarcinoma: a Case Report
ANTICANCER RESEARCH 36: 769-772 (2016) Giant Cavernous Hepatic Hemangioma Diagnosed Incidentally in a Perimenopausal Obese Female with Endometrial Adenocarcinoma: A Case Report TIVADAR BARA JR.1, SIMONA GURZU2, IOAN JUNG2, MIRCEA MURESAN2, JANOS SZEDERJESI3 and TIVADAR BARA1 Departments of 1Surgery, 2Pathology, and 3Intensive Care, University of Medicine and Pharmacy of Tirgu-Mures, Tirgu-Mures, Romania Abstract. Hemangiomas are the most common benign Macroscopically, LHs are hypervascular poorly tumors of the liver, considered giant when they exceed 50- circumscribed lesions. Microscopically, they consist of large 100 mm in diameter. In the present report, we present a case cavities filled with venous blood coming from the hepatic of a 5.2-kg hemangioma of the right hepatic lobe, with artery, lined by endothelial cells and separated by fibrous septa hemangiomatous foci in the left lobe, which was incidentally (1). Due to unreported malignant transformation of LHs, their diagnosed in a 53-year-old obese female hospitalized for slow growth and low risk for bleeding, simple observation of uterine bleeding. The computed tomographic scan and asymptomatic lesions is usually recommended (1). physical examination revealed a giant abdominal tumor and LHs can be single or multiple and their size can vary from hepatic hemangioma of the right hepatic lobe was suspected. a few millimeters to over 20 cm (5). The term 'giant Right hepatectomy and total hysterectomy with bilateral hemangioma' is commonly used for lesions larger than 4 cm ovariectomy was performed. The histological examination of in diameter (1-5). LHs over 10 cm are considered extremely the surgical specimens confirmed the extremely giant large or massive, and only occasional cases over 30 cm or cavernous hepatic hemangioma, and a synchronous pT1a weighing more than 2 to 3 kg have been reported (3, 4). -

Malignant Vascular Tumors&Mdash
Modern Pathology (2014) 27, S30–S38 S30 & 2014 USCAP, Inc All rights reserved 0893-3952/14 $32.00 Malignant vascular tumors—an update Cristina Antonescu Department of Pathology, Memorial Sloan-Kettering Cancer Center, New York, NY, USA Although benign hemangiomas are among the most common diagnoses amid connective tissue tumors, sarcomas showing endothelial differentiation (ie, angiosarcoma and epithelioid hemangioendothelioma) represent under 1% of all sarcoma diagnoses, and thus it is likely that fewer than 500 people in the United States are affected each year. Differential diagnosis of malignant vascular tumors can be often quite challenging, either at the low end of the spectrum, distinguishing an epithelioid hemangioendothelioma from an epithelioid hemangioma, or at the high-grade end of the spectrum, between an angiosarcoma and a malignant epithelioid hemangioendothelioma. Within this differential diagnosis both clinico-radiological features (ie, size and multifocality) and immunohistochemical markers (ie, expression of endothelial markers) are often similar and cannot distinguish between benign and malignant vascular lesions. Molecular ancillary tests have long been needed for a more objective diagnosis and classification of malignant vascular tumors, particularly within the epithelioid phenotype. As significant advances have been recently made in understanding the genetic signatures of vascular tumors, this review will take the opportunity to provide a detailed update on these findings. Specifically, this article will focus on -
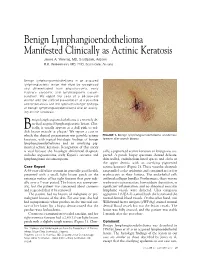
Benign Lymphangioendothelioma Manifested Clinically As Actinic Keratosis James A
Benign Lymphangioendothelioma Manifested Clinically as Actinic Keratosis James A. Yiannias, MD, Scottsdale, Arizona R.K. Winkelmann, MD, PhD, Scottsdale, Arizona Benign lymphangioendothelioma is an acquired lymphangiectatic lesion that must be recognized and differentiated from angiosarcoma, early Kaposi’s sarcoma, and lymphangioma circum- scriptum. We report the case of a 68-year-old woman with the clinical presentation of a possible actinic keratosis and the typical histologic findings of benign lymphangioendothelioma and an overly- ing actinic keratosis. enign lymphangioendothelioma is a recently de- scribed acquired lymphangiectatic lesion. Clin- ically, it usually appears as a dull pink to red- B 1 dish brown macule or plaque. We report a case in which the clinical presentation was possible actinic FIGURE 1. Benign lymphangioendothelioma at extensor keratosis, with typical histologic findings of benign forearm after punch biopsy. lymphangioendothelioma and an overlying pig- mented actinic keratosis. Recognition of this entity is vital because the histologic differential diagnosis cally, a pigmented actinic keratosis or lentigo was sus- includes angiosarcoma, early Kaposi’s sarcoma, and pected. A punch biopsy specimen showed delicate, lymphangioma circumscriptum. thin-walled, endothelium-lined spaces and clefts in the upper dermis, with an overlying pigmented Case Report actinic keratosis (Figure 2). These vascular channels A 68-year-old white woman in generally good health ran parallel to the epidermis and contained no or few presented with a small, light brown patch on the erythrocytes in their lumina. The endothelial cells extensor surface of her right forearm that grew radi- outlined collagen bundles. Furthermore, there was no ally over a 2-year period. The lesion was asymptom- erythrocyte extravasation, hemosiderin deposition, or atic, but the patient was concerned about cosmesis significant inflammation, and no abnormal muscular and requested that it be removed. -

Hepatic Angiosarcoma Masquerading As Hemangioma
Hepatic Angiosarcoma Masquerading as Hemangioma: A CASO CLÍNICO Challenging Differential Diagnosis Angiosarcoma Hepático e Hemangioma: Um Diagnóstico Diferencial Desafiante Ana Rita GARCIA1, João RIBEIRO1, Helena GERVÁSIO1, Francisco Castro e SOUSA2,3 Acta Med Port 2017 Oct;30(10):750-753 ▪ https://doi.org/10.20344/amp.8593 ABSTRACT Hemangiomas are usually diagnosed based on ultrasound findings. The presence of symptoms, rapid growth or atipical imagiological findings should make us consider other diagnoses, including malignant tumors such as angiosarcomas. We describe the case of a previously healthy 46-year-old female without a history of exposure to carcinogens who presented with abdominal pain for two months. Diagnostic work-up revealed elevated gamma-glutamyl transferase and lactate dehydrogenase levels. Abdominal ultrasound described a large nodular lesion in the right lobe of the liver described as a hemangioma. One month later, a computed tomography-scan was made and revealed the same lesion, which had grown from 13.5 to 20 cm, maintaining typical imaging characteristics of a hemangioma. A right hepatectomy was performed and pathology revealed an angiosarcoma. After surgery, a positron emission tomography-com- puted tomography scan showed hepatic and bone metastasis. The patient started taxane-based chemotherapy and lumbar palliative radiotherapy, but died 10 months after surgery. This case shows how difficult it is to diagnose hepatic angiosarcoma relying only on imaging findings. Two abdominal computed tomography -scans were performed and none suggested this diagnosis. Angiosarcoma is a very aggressive tumour with an adverse prognosis. Surgery is the only curative treatment available. However, it is rarely feasible due to unresectable disease or distant metastasis. -

Cervical Lymphangioma in Adult Cervical Lymphangioma in Adult
AIJOC 10.5005/jp-journals-10003-1101 CASE REPORT Cervical Lymphangioma in Adult Cervical Lymphangioma in Adult Vinod Tukaram Kandakure, Girish Vitthalrao Thakur, Amit Ramesh Thote, Ayesha Junaid Kausar ABSTRACT There was no enhancing portion, and the lesion measured Lymphangiomas are uncommon congenital lesions of the approximately 6 × 4 × 3 cm. It was profoundly hyperintense lymphatic system which are usually present in childhood. We on T2W1 images (Fig. 2). It showed multiple incomplete report a case of adult lymphangioma, localized in the neck, and thin septi with communicating loculi. discuss the presentation, diagnosis and management of this tumor. Surgery Keywords: Head and neck, Lymphangioma, Children, Diagnosis, Treatment. The mass was reached through a 7 cm transverse skin incision in the submandibular region. Cystic mass was seen in How to cite this article: Kandakure VT, Thakur GV, Thote AR, Kausar AJ. Cervical Lymphangioma in Adult. Int J subcutaneous plane. Mass was dissected from tail of parotid Otorhinolaryngol Clin 2012;4(3):147-150. laterally then from behind posterior belly of digastric muscle till submandibular gland medially to vallecula in Source of support: Nil superomedial plane. It was touching internal jugular vein Conflict of interest: None declared (IJV) and common carotid artery posteriorly. Cystic mass was draining into the IJV via small vessel (Fig. 3). That vessel INTRODUCTION was ligated near the IJV. Although the lesion was in close Lymphangioma is an uncommon benign pathology, usually proximity to nerves, vessels and muscles, there was no reported in children and rarely in adults. Cervical lymphangioma involves congenital and cystic abnormalities derived from lymphatic vessels with a progressive and painless growth.