Emcyt® Estramustine Phosphate Sodium Capsules DESCRIPTION
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Guide to Feminizing Hormones – Estrogen
1 | Feminizing Hormones A Guide to Feminizing Hormones Hormone therapy is an option that can help transgender and gender-diverse people feel more comfortable in their bodies. Like other medical treatments, there are benefits and risks. Knowing what to expect will help us work together to maximize the benefits and minimize the risks. What are hormones? Hormones are chemical messengers that tell the body’s cells how to function, when to grow, when to divide, and when to die. They regulate many functions, including growth, sex drive, hunger, thirst, digestion, metabolism, fat burning & storage, blood sugar, cholesterol levels, and reproduction. What are sex hormones? Sex hormones regulate the development of sex characteristics, including the sex organs such as genitals and ovaries/testicles. Sex hormones also affect the secondary sex characteristics that typically develop at puberty, like facial and body hair, bone growth, breast growth, and voice changes. There are three categories of sex hormones in the body: • Androgens: testosterone, dehydroepiandrosterone (DHEA), dihydrotestosterone (DHT) • Estrogens: estradiol, estriol, estrone • Progestin: progesterone Generally, “males” tend to have higher androgen levels, and “females” tend to have higher levels of estrogens and progestogens. What is hormone therapy? Hormone therapy is taking medicine to change the levels of sex hormones in your body. Changing these levels will affect your hair growth, voice pitch, fat distribution, muscle mass, and other features associated with sex and gender. Feminizing hormone therapy can help make the body look and feel less “masculine” and more “feminine" — making your body more closely match your identity. What medicines are involved? There are different kinds of medicines used to change the levels of sex hormones in your body. -

Structure and Origin of Uterine and Extragenital L=Ibroids Induced
Structure and Origin of Uterine and Extragenital l=ibroids Induced Experimentally in the Guinea Pig by Prolonged Administration of Estrogens* Alexander Lipschotz, M.D., and Louis Vargas, Jr., M.D. (From Department o/ Experimental Medicine, National Health Service o/the Republic o/Chile, Santiago, Chile) (Received for publication December 13, x94o) The purpose of this communication is to present the These experimentally induced abdominal tumors findings of a detailed microscopical study of the sites present a smooth surface formed of a capsule com- of origin and stages of development of the subserous posed of flattened superficial cells (Plate 2, Figs. 2-A fibroid tumors induced in guinea pigs by prolonged and 2-B). The cells beneath the capsule resemble administration of estrogens. Details of treatment of fibroblasts. These cells have definite boundaries or the animals are given in the explanations of Plates I- 5. they are separated from each other by collagenous Subserous uterine tumors which can be induced in fibers (Plate 4, Fig. ix-C). guinea pigs by prolonged administration of estrogens, The masses of fibroid tumors arising from the apex as described by Nelson (26, 27), were found to be of the uterine horn may enclose the tubes or large fibroids. Lipschiitz, Iglesias, and Vargas (i3, 18, 22) tubal cysts. The demarcation between the muscular have shown that extragenital tumors in the abdominal coat of the tube and the tumor is not always sharp. cavity, induced by estrogens, also were fibroids. The In some instances, especially when the apical fibroid localization of these tumo~:s at various sites on the is small, the tumor is in close contact with an abun- uterus, pancreas, kidney, spleen, etc., have been de- dance of smooth muscle and adipose tissue (Plate 2, scribed by Iglesias (5), Vargas and Lipschiitz (32), Fig. -
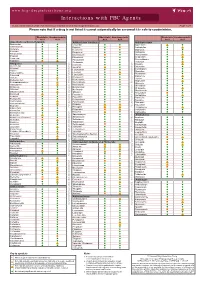
Interactions with PBC Agents
www.hep-druginteractions.org Interactions with PBC Agents Charts created March 2020. Full information available at www.hep-druginteractions.org Page 1 of 4 Please note that if a drug is not listed it cannot automatically be assumed it is safe to coadminister. Obeticholic Ursodeoxycholic Obeticholic Ursodeoxycholic Obeticholic Ursodeoxycholic Acid Acid Acid Acid Acid Acid Anaesthetics & Muscle Relaxants Antibacterials (continued) Antidepressants Bupivacaine Cloxacillin Agomelatine Cisatracurium Dapsone Amitriptyline Isoflurane Delamanid Bupropion Ketamine Ertapenem Citalopram Nitrous oxide Erythromycin Clomipramine Propofol Ethambutol Desipramine Thiopental Flucloxacillin Desvenlafaxine Tizanidine Gentamicin Dosulepin Analgesics Imipenem Doxepin Aceclofenac Isoniazid Duloxetine Alfentanil Escitalopram Aspirin Levofloxacin Linezolid Fluoxetine Buprenorphine Fluvoxamine Lymecycline distribution. Celecoxib Imipramine Meropenem Codeine Lithium Methenamine Dexketoprofen Maprotiline Metronidazole Dextropropoxyphene Mianserin Moxifloxacin Diamorphine Milnacipran Diclofenac Nitrofurantoin only. Not for distribution. for only. Not Mirtazapine Diflunisal Norfloxacin Moclobemide Dihydrocodeine Ofloxacin Nefazodone Etoricoxib Penicillin V Nortriptyline Fentanyl Piperacillin Paroxetine Flurbiprofen Pivmecillinam Sertraline Hydrocodone use ersonal Pyrazinamide Tianeptine Hydromorphone Rifabutin Trazodone Ibuprofen Rifampicin -

Gender-Affirming Hormone Therapy
GENDER-AFFIRMING HORMONE THERAPY Julie Thompson, PA-C Medical Director of Trans Health, Fenway Health March 2020 fenwayhealth.org GOALS AND OBJECTIVES 1. Review process of initiating hormone therapy through the informed consent model 2. Provide an overview of masculinizing and feminizing hormone therapy 3. Review realistic expectations and benefits of hormone therapy vs their associated risks 4. Discuss recommendations for monitoring fenwayhealth.org PROTOCOLS AND STANDARDS OF CARE fenwayhealth.org WPATH STANDARDS OF CARE, 2011 The criteria for hormone therapy are as follows: 1. Well-documented, persistent (at least 6mo) gender dysphoria 2. Capacity to make a fully informed decision and to consent for treatment 3. Age of majority in a given country 4. If significant medical or mental health concerns are present, they must be reasonably well controlled fenwayhealth.org INFORMED CONSENT MODEL ▪ Requires healthcare provider to ▪ Effectively communicate benefits, risks and alternatives of treatment to patient ▪ Assess that the patient is able to understand and consent to the treatment ▪ Informed consent model does not preclude mental health care! ▪ Recognizes that prescribing decision ultimately rests with clinical judgment of provider working together with the patient ▪ Recognizes patient autonomy and empowers self-agency ▪ Decreases barriers to medically necessary care fenwayhealth.org INITIAL VISITS ▪ Review history of gender experience and patient’s goals ▪ Document prior hormone use ▪ Assess appropriateness for gender affirming medical -

(12) United States Patent (10) Patent No.: US 9.498,431 B2 Xu Et Al
USOO9498431B2 (12) United States Patent (10) Patent No.: US 9.498,431 B2 Xu et al. (45) Date of Patent: Nov. 22, 2016 (54) CONTROLLED RELEASING COMPOSITION 7,053,134 B2 * 5/2006 Baldwin et al. .............. 522,154 2004/0058056 A1 3/2004 Osaki et al. ................... 427.2.1 (76) Inventors: Jianjian Xu, Hefei (CN); Shiliang 2005/0037047 A1 2/2005 Song Wang, Hefei (CN); Manzhi Ding 2007/0055364 A1* 3/2007 Hossainy .................. A61F 2/82 s: s s 623, 1.38 Hefei (CN) 2008/0274194 A1* 11/2008 Miller .................... A61K 9.146 424/489 (*) Notice: Subject to any disclaimer, the term of this patent is extended or adjusted under 35 FOREIGN PATENT DOCUMENTS U.S.C. 154(b) by 0 days. CN 1208.610 A 2, 1999 (21) Appl. No.: 13/133,656 EP O251680 A2 1, 1988 JP S63-22516. A 1, 1988 JP H1O-310518 A 11, 1998 (22) PCT Filed: Dec. 10, 2009 WO 96,10395 A1 4f1996 WO WO 2005.000277 A1 * 1, 2005 (86). PCT No.: PCT/CN2009/075468 WO 2007 115045 A2 10, 2007 WO 2008/OO2657 A2 1, 2008 S 371 (c)(1), WO 2008OO2657 A2 1, 2008 (2), (4) Date: Jun. 9, 2011 WO 2008041246 A2 4/2008 (87) PCT Pub. No.: WO2010/066203 OTHER PUBLICATIONS PCT Pub. Date: Jun. 17, 2010 Crowley and Zhang, Pharmaceutical Application of Hot Melt Extru (65) Prior Publication Data sion: Part I, Drug Development and Industrial Pharmacy, 2007. 33:909-926.* US 2011/024.4043 A1 Oct. 6, 2011 The Use of Poly (L-Lactide) and RGD Modified Microspheres as Cell Carriers in a Flow Intermittency Bioreactor for Tissue Engi (30) Foreign Application Priority Data neering Cartilage. -

Confidential: for Review Only
BMJ Confidential: For Review Only The risk of fall and fracture with the initiation of a prostate - selective alpha antagonist Journal: BMJ Manuscript ID: BMJ.2015.028205 Article Type: Research BMJ Journal: BMJ Date Submitted by the Author: 17-Jul-2015 Complete List of Authors: Welk, Blayne; Western University, McArthur, Eric; Institute for Clinical Evaluative Sciences,, Fraser, Lisa-Ann; Western University, Medicine Hayward, Jade; Institute for Clinical Evaluative Sciences,, Dixon, Stephanie; Institute for Clinical Evaluative Sciences,, Hwang, Joseph; Case Western Reserve University School of Medicine, Ordon, Michael; University of Toronto, Surgery (Urology) Keywords: BPH, Fall, Fracture, Alpha antgonist https://mc.manuscriptcentral.com/bmj Page 1 of 45 BMJ 1 2 The risk of fall and fracture with the initiation of a prostate-selective alpha antagonist 3 4 1,2,3 2 4 2 5 Blayne Welk MD MSc , Eric McArthur MSc , Lisa-Ann Fraser MD MSc , Jade Hayward , 6 Stephanie Dixon MSc PhD 2,3 , Y. Joseph Hwang MSc 5, Michael Ordon MD MSc 6 7 8 1 DepartmentConfidential: of Surgery, Western University, For London Review, Ontario, Canada Only 9 2 Institute for Clinical Evaluative Sciences, London, Ontario, Canada 10 11 3 Department of Epidemiology and Biostatistics, Western University, London, Ontario, Canada 12 4 Department of Medicine, Western University, London, Ontario 13 5 MD Candidate, Case Western Reserve University School of Medicine, Cleveland, Ohio, USA 14 6 Division of Urology, Department of Surgery, University of Toronto, Toronto, Ontario, Canada 15 16 17 Correspondence: 18 Blayne Welk, MD MSc 19 Assistant Professor, Division of Urology and Epidemiology and Biostatistics 20 Western University 21 Room B4-667 22 23 St Joseph's Health Care 24 268 Grosvenor Street London ON N6A 4V2 25 Telephone: 519 646-6367 | Fax: 519 646-6037 26 [email protected] 27 28 29 Addresses: 30 Mr McArthur: [email protected] 31 LHSC – Victoria Hospital 32 ELL-101, 800 Commissioners Rd. -

Preferred Drug List 4-Tier
Preferred Drug List 4-Tier 21NVHPN13628 Four-Tier Base Drug Benefit Guide Introduction As a member of a health plan that includes outpatient prescription drug coverage, you have access to a wide range of effective and affordable medications. The health plan utilizes a Preferred Drug List (PDL) (also known as a drug formulary) as a tool to guide providers to prescribe clinically sound yet cost-effective drugs. This list was established to give you access to the prescription drugs you need at a reasonable cost. Your out- of-pocket prescription cost is lower when you use preferred medications. Please refer to your Prescription Drug Benefit Rider or Evidence of Coverage for specific pharmacy benefit information. The PDL is a list of FDA-approved generic and brand name medications recommended for use by your health plan. The list is developed and maintained by a Pharmacy and Therapeutics (P&T) Committee comprised of actively practicing primary care and specialty physicians, pharmacists and other healthcare professionals. Patient needs, scientific data, drug effectiveness, availability of drug alternatives currently on the PDL and cost are all considerations in selecting "preferred" medications. Due to the number of drugs on the market and the continuous introduction of new drugs, the PDL is a dynamic and routinely updated document screened regularly to ensure that it remains a clinically sound tool for our providers. Reading the Drug Benefit Guide Benefits for Covered Drugs obtained at a Designated Plan Pharmacy are payable according to the applicable benefit tiers described below, subject to your obtaining any required Prior Authorization or meeting any applicable Step Therapy requirement. -

Antimicrotubule Effects of Estramustine, an Antiprostatic Tumor Drug
[CANCER RESEARCH 45, 3891-3897, August 1985] Antimicrotubule Effects of Estramustine, an Antiprostatic Tumor Drug Mark E. Stearns1 and Kenneth D. Tew2 Departments of Anatomy [M. E. S.] and of Medicine and Pharmacology [K. D, T.], Vincent T. Lombardi Cancer Research Center, Georgetown University Hospital, Washington, DC 20007 ABSTRACT cytomatrix effects of EM and learn how cytoplasmic related effects of EM might ultimately produce the reported antimitotic Estramustine [170-estradiol 3 N bis(2-chloroethyl)carbamate; events in dividing cells (6). EM] is a stable conjugate of estradiol and nor-nitrogen mustard In this paper, we have investigated possible cytotoxic effects that is used for the treatment of human prostatic carcinoma. We of EM at the cytological level. For these studies, the fish erythro- have studied the cytotoxic effects of EM on the cytoskeletal phore or red pigment cell has been used as a model system for organization of squirrelfish pigment cells (erythrophores) and investigation of the cytotoxic consequences of EM. There are a human prostatic tumor cells (DU 145) in culture. Light and whole- number of attractive reasons for utilizing erythrophores for the mount electron microscopy studies reveal that, at /¿Mlevels(60 work described here. Erythrophores are symmetrical cells with to 120 ¿IM),EMhas a dose-dependent disruptive effect on cell thousands of radially ordered microtubules which control the shape, cytoskeletal organization, and intracellular transport. directed motion of numerous red pigment granules (14, 19). At Upon removal of the drug, the cytological effects of EM are the light microscopic level, the pigment is observed to pulsate or rapidly reversible in fish cells but not DU 145s. -

Order in Council 1243/1995
PROVINCE OF BRITISH COLUMBIA ORDER OF THE LIEUTENANT GOVERNOR IN COUNCIL Order in Council No. 12 4 3 , Approved and Ordered OCT 121995 Lieutenant Governor Executive Council Chambers, Victoria On the recommendation of the undersigned, the Lieutenant Governor, by and with the advice and consent of the Executive Council, orders that Order in Council 1039 made August 17, 1995, is rescinded. 2. The Drug Schedules made by regulation of the Council of the College of Pharmacists of British Columbia, as set out in the attached resolution dated September 6, 1995, are hereby approved. (----, c" g/J1"----c- 4- Minister of Heal fandand Minister Responsible for Seniors Presidin Member of the Executive Council (This pan is for adnwustratlye purposes only and is not part of the Order) Authority under which Order Is made: Act and section:- Pharmacists, Pharmacy Operations and Drug Scheduling Act, section 59(2)(1), 62 Other (specify): - Uppodukoic1enact N6145; Resolution of the Council of the College of Pharmacists of British Columbia ("the Council"), made by teleconference at Vancouver, British Columbia, the 6th day of September 1995. RESOLVED THAT: In accordance with the authority established in Section 62 of the Pharmacists, Pharmacy Operations and Drug Scheduling Act of British Columbia, S.B.C. Chapter 62, the Council makes the Drug Schedules by regulation as set out in the attached schedule, subject to the approval of the Lieutenant Governor in Council. Certified a true copy Linda J. Lytle, Phr.) Registrar DRUG SCHEDULES to the Pharmacists, Pharmacy Operations and Drug Scheduling Act of British Columbia The Drug Schedules have been printed in an alphabetical format to simplify the process of locating each individual drug entry and determining its status in British Columbia. -

2021 Formulary List of Covered Prescription Drugs
2021 Formulary List of covered prescription drugs This drug list applies to all Individual HMO products and the following Small Group HMO products: Sharp Platinum 90 Performance HMO, Sharp Platinum 90 Performance HMO AI-AN, Sharp Platinum 90 Premier HMO, Sharp Platinum 90 Premier HMO AI-AN, Sharp Gold 80 Performance HMO, Sharp Gold 80 Performance HMO AI-AN, Sharp Gold 80 Premier HMO, Sharp Gold 80 Premier HMO AI-AN, Sharp Silver 70 Performance HMO, Sharp Silver 70 Performance HMO AI-AN, Sharp Silver 70 Premier HMO, Sharp Silver 70 Premier HMO AI-AN, Sharp Silver 73 Performance HMO, Sharp Silver 73 Premier HMO, Sharp Silver 87 Performance HMO, Sharp Silver 87 Premier HMO, Sharp Silver 94 Performance HMO, Sharp Silver 94 Premier HMO, Sharp Bronze 60 Performance HMO, Sharp Bronze 60 Performance HMO AI-AN, Sharp Bronze 60 Premier HDHP HMO, Sharp Bronze 60 Premier HDHP HMO AI-AN, Sharp Minimum Coverage Performance HMO, Sharp $0 Cost Share Performance HMO AI-AN, Sharp $0 Cost Share Premier HMO AI-AN, Sharp Silver 70 Off Exchange Performance HMO, Sharp Silver 70 Off Exchange Premier HMO, Sharp Performance Platinum 90 HMO 0/15 + Child Dental, Sharp Premier Platinum 90 HMO 0/20 + Child Dental, Sharp Performance Gold 80 HMO 350 /25 + Child Dental, Sharp Premier Gold 80 HMO 250/35 + Child Dental, Sharp Performance Silver 70 HMO 2250/50 + Child Dental, Sharp Premier Silver 70 HMO 2250/55 + Child Dental, Sharp Premier Silver 70 HDHP HMO 2500/20% + Child Dental, Sharp Performance Bronze 60 HMO 6300/65 + Child Dental, Sharp Premier Bronze 60 HDHP HMO -

Feminizing Gender-Affirming Hormone Care the Michigan Medicine Approach
Feminizing Gender-Affirming Hormone Care The Michigan Medicine Approach Our goal is to partner with you to provide the medical care you need in affirming your gender. Our focus is on your lifelong health, safety, and individual medical and transition-related needs. The Michigan Medicine approach is based on the limited but growing medical evidence surrounding gender-affirming hormone care. Based on the available science, we believe mimicking normal physiology will provide you with the best balance of physical and emotional changes and long-term health. This philosophy aligns with current national and international medical guidelines in the care of gender diverse people. We are committed to staying up-to-date with the latest research and medical evidence to ensure you are getting the highest quality care. We know that there are competing approaches to gender-affirming care that are not based on validated scientific evidence. These approaches make scientifically unsubstantiated claims and have unknown short and long-term risks. We are happy to discuss these with you. Below are some answers to questions our patients have asked us about gender- affirming hormone care. We hope the Q&A will help you understand the medical evidence behind our approach to your gender-affirming hormone care, and how it may differ from other approaches, including the approach other well-known clinics in Southeast Michigan. Is there a benefit for monitoring both estrone (E1) and estradiol (E2) levels and aiming for a particular ratio? There are 3 naturally occurring human estrogens: estrone (E1), estradiol (E2), and estriol (E3). Your body naturally balances your estradiol and estrone ratio. -

Binding Characteristics of a Major Protein in Rat Ventral Prostate Cytosol That Interacts with Estramustine, a Nitrogen Mustard Derivative of 17ß-Estradiol
[CANCER RESEARCH 39, 5155-5164, December 1979] 0008-5472/79/0039-OOOOS02.00 Binding Characteristics of a Major Protein in Rat Ventral Prostate Cytosol That Interacts with Estramustine, a Nitrogen Mustard Derivative of 17ß-Estradiol BjörnForsgren, Jan-Àke Gustafsson, Ake Pousette, and Bertil Hogberg AB Leo Research Laboratories. Pack. S-251 00 Helsingborg, Sweden [B.F.. B.H.], and Departments of Chemistry and Medical Nutrition. ¡J-ÄG.. A P.¡and Pharmacology [BH.], Karolinska Institute!. S-104 01 Stockholm 60. Sweden ABSTRACT causes atrophy of the testes and accessory sex organs; re duces the uptake of zinc by the prostate; depresses the 5a- The tissue distribution of [3H]estramustine, the dephospho- reductase, arginase, and acid phosphatase activities in the rylated metabolite of estramustine phosphate (Estracyt), in the male rat was compared to that of [3H]estradiol 30 min and 2 hr prostate; and affects lipid and carbohydrate metabolism (10, 11, 20, 29, 31 -33, 42). Although the observed effects in many following i.p. administration. In contrast to estradiol, estramus respects are similar to estrogenic effects, several experimental tine was found to be efficiently concentrated in the ventral and clinical results indicate that estramustine phosphate affects prostate gland by a soluble protein. The binding characteristics normal and neoplastic prostate tissue in a way that cannot be of this protein were studied in vitro using cytosol preparations attributed solely to its antigonadotropic or weak estrogenic of the gland. With a dextran-coated charcoal technique, the properties (15, 16, 30, 38). protein was found to bind estramustine with a broad pH opti Plym Forshell and Nilsson (35), using labeled compounds (1 mum between pH 7 and pH 8.5, with an apparent Kd of 10 to to 10 mg/kg body weight), found considerably higher levels of 30 nw, and with a binding capacity of about 5 nmol/mg cytosol radioactivity in the rat ventral prostate following i.v.