Treating Corneal Ulceration in Dogs Part 2: Deep Ulcers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

Neurotrophic Keratopathy and Diabetes Mellitus a Lockwood Et Al 838
Eye (2006) 20, 837–839 & 2006 Nature Publishing Group All rights reserved 0950-222X/06 $30.00 www.nature.com/eye 1 1 2 Neurotrophic A Lockwood , M Hope-Ross and P Chell CASE SERIES keratopathy and diabetes mellitus Abstract no history of previous corneal trauma or herpes simplex infection. Ocular examination revealed Diabetes mellitus is frequently associated a best-corrected visual acuity of 6/12 in both with microvascular complications such as eyes. There was an epithelial irregularity retinopathy, nephropathy, and peripheral extending across the inferonasal quadrant of the neuropathy. Neurotrophic keratopathy occurs right cornea. A diagnosis of exposure in response to a neuropathy of the ophthalmic keratopathy was made. She was treated with division of the trigeminal nerve. Rarely has artificial tears and a month later the epithelium diabetic neurotrophic keratopathy been had healed. A year later, an epithelial defect in described. This paper discusses the the same area was seen at follow-up. Again she ophthalmic histories of three patients who was asymptomatic and the visual acuity was presented with diabetic neurotrophic unchanged. Decreased corneal sensation was keratopathy. In one patient the corneal noted using a cotton swab to touch the ulceration was the sole presenting feature of peripheral and central cornea. A diagnosis of his diabetes. We discuss the need for increased diabetic neurotrophic keratopathy was made. vigilance in the ophthalmic community for She was treated with ocular lubricants. After suspecting diabetes in patients with 6 months, the defect had increased in size to unexplained corneal epithelial disease. 5.5 mm. There was associated corneal Eye (2006) 20, 837–839. -

Topical Serum for Treatment of Keratomalacia
PROCEDURES PRO > OPHTHALMOLOGY > PEER REVIEWED Topical Serum for Treatment of Keratomalacia Amy Knollinger, DVM, DACVO Eye Care for Animals Salt Lake City, Utah Corneal Anatomy An understanding of corneal anatomy is vital to determine if serum therapy for the treatment of keratomalacia should be initiated. The cornea makes up the anterior por- tion of the globe and provides multiple functions for vision: it is transparent (despite originating from surface ectoderm), thereby allowing for clear vision; it acts as the major refractive (bending of light) surface of the globe; and it provides a protective barrier between the globe and the environment The cornea consists of 4 layers in domestic species, being approximately 0.45–0.55 mm thick in the normal dog. The corneal epithelium is the most external layer overly- What You Will Need ing the stromal layer, which accounts for 90% of the total corneal thickness. The cor- n Sterile gloves neal epithelium in the dog and cat is 5–11 cells thick and has a turnover rate of n approximately 7 days.1 The stroma is made up of collagen fibers, which are precisely Clean #40 clipper blade arranged in parallel sheets running the entire diameter of the cornea, allowing for its n Chlorhexidine scrub and solution transparency. The third layer is an acellular membrane (ie, Descemet’s membrane), n Sterile needle and syringe which forms the basement membrane for the innermost layer, the endothelium. The n corneal endothelium is a single layer of hexagonally shaped cells forming the internal Red top sterile blood collection or barrier between the anterior chamber and the cornea.2 serum separator tube n Centrifuge Corneal Disease n Sterile pipette Corneal ulcers are classified by underlying cause. -

JMSCR Vol||08||Issue||02||Page 208-210||February 2020
JMSCR Vol||08||Issue||02||Page 208-210||February 2020 http://jmscr.igmpublication.org/home/ ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v8i2.40 Keratomalacia - A Case Report Authors Deepthi Pullepu1*, Deepthi Janga2, V Murali Krishna3 *Corresponding Author Deepthi Pullepu Department of Ophthalmology, Rangaraya Medical College, Kakinada, Andhra Pradesh, India Abstract Xerophthalmia refers to an ocular condition of destructive dryness of conjunctiva and cornea caused due to severe vitamin A deficiency. Usually affects infants, children and women of reproductive age group. It is estimated to affect about one-third of children under the age of five around the world. Keratomalacia means dry and cloudy cornea which melts and perforates, caused due to severe vitamin A deficiency. Here we describe a case of 21 year old female with neurofibromatosis type 1 presenting with keratomalacia. Keywords: Vitamin A deficiency, Xerophthalmia, Keratomalacia. Introduction blindness is a significant contributor Vitamin A is essential for the functioning of the In India, it is estimated that there are immune system, healthy growth and development approximately 6.8 million people who have vision of body and is usually acquired through diet. less than 6/60 in at least one eye due to corneal Globally, 190 million children under five years of diseases; of these, about a million have bilateral age are affected by vitamin A deficiency involvement. They suffer from an increased risk of visual Corneal blindness resulting due to this disease can impairment, illness and death from childhood be completely prevented by institution of effective infections such as measles and those causing preventive or prophylactic measures at the diarrhoea community level. -
Corneal Ulcers in Cats
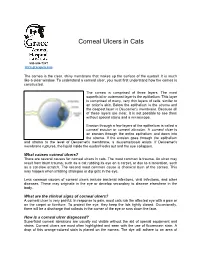
Corneal Ulcers in Cats 803-808-7387 www.gracepets.com The cornea is the clear, shiny membrane that makes up the surface of the eyeball. It is much like a clear window. To understand a corneal ulcer, you must first understand how the cornea is constructed. The cornea is comprised of three layers. The most superficial or outermost layer is the epithelium. This layer is comprised of many, very thin layers of cells, similar to an onion’s skin. Below the epithelium is the stroma and the deepest layer is Descemet's membrane. Because all of these layers are clear, it is not possible to see them without special stains and a microscope. Erosion through a few layers of the epithelium is called a corneal erosion or corneal abrasion. A corneal ulcer is an erosion through the entire epithelium and down into the stroma. If the erosion goes through the epithelium and stroma to the level of Descemet's membrane, a descemetocele exists. If Descemet's membrane ruptures, the liquid inside the eyeball leaks out and the eye collapses. What causes corneal ulcers? There are several causes for corneal ulcers in cats. The most common is trauma. An ulcer may result from blunt trauma, such as a cat rubbing its eye on a carpet, or due to a laceration, such as a cat-claw scratch. The second most common cause is chemical burn of the cornea. This may happen when irritating shampoo or dip gets in the eye. Less common causes of corneal ulcers include bacterial infections, viral infections, and other diseases. -

Involvement of the Eye in Protein Malnutrition * -303
Bull. Org. mond. Sante 1958, 19, 303-314 Bull. Wld Hith Org. INVOLVEMENT OF THE EYE IN PROTEIN MALNUTRITION * D. S. McLAREN, M.D., Ph.D., D.T.M. & H. Medical Research Officer, East African Institute for Medical Research, Mwanza, Tanganyika Formerly at the MRC Human Nutrition Research Unit, National Institute for Medical Research, London SYNOPSIS An extensive review of the literature on protein malnutrition, with special reference to the frequency of involvement of the eyes, has been made by the author. Consideration of accounts from all parts of the world and in many different languages, including early as well as more recent descriptions of the syndrome, indicates that this important complication has not received sufficient attention hitherto. The evidence available suggests that it is nearly always an accompanying deficiency of vitamin A that is responsible. Less commonly reported-and producing less severe effects-is deficiency of the B-complex vitamins, and there is no clear evidence to date that protein deficiency itself damages the eyes in these cases. The ways in which protein lack might interfere with various aspects of vitamin-A metabolism are discussed, but it is pointed out that their actual significance in human disease is not yet known. A low dietary intake of vitamin A is regarded by the author as being the prime factor in the causation of eye complications, and attention is drawn to the necessity to correct this as part of any prophylactic or therapeutic programme aimed primarily at combat- ing protein malnutrition. The syndrome known by such various names as kwashiorkor, nutritional oedema syndrome, sindrome pluricarencial, and many others (Trowell, Davies & Dean, 1954), and characterized chiefly by a dietary deficiency ofprotein, has been reported as occurring amongst most of the malnourished communities of the world. -

Corneal Cross-Linking in Infectious Keratitis David Tabibian1,5*, Cosimo Mazzotta2 and Farhad Hafezi1,3,4
Tabibian et al. Eye and Vision (2016) 3:11 DOI 10.1186/s40662-016-0042-x REVIEW Open Access PACK-CXL: Corneal cross-linking in infectious keratitis David Tabibian1,5*, Cosimo Mazzotta2 and Farhad Hafezi1,3,4 Abstract Background: Corneal cross-linking (CXL) using ultraviolet light-A (UV-A) and riboflavin is a technique developed in the 1990’s to treat corneal ectatic disorders such as keratoconus. It soon became the new gold standard in multiple countries around the world to halt the progression of this disorder, with good long-term outcomes in keratometry reading and visual acuity. The original Dresden treatment protocol was also later on used to stabilize iatrogenic corneal ectasia appearing after laser-assisted in situ keratomileusis (LASIK) and photorefractive keratectomy (PRK). CXL efficiently strengthened the cornea but was also shown to kill most of the keratocytes within the corneal stroma, later on repopulated by those cells. Review: Ultraviolet-light has long been known for its microbicidal effect, and thus CXL postulated to be able to sterilize the cornea from infectious pathogens. This cytotoxic effect led to the first clinical trials using CXL to treat advanced infectious melting corneal keratitis. Patients treated with this technique showed, in the majority of cases, a stabilization of the melting process and were able to avoid emergent à chaud keratoplasty. Following those primary favorable results, CXL was used to treat beginning bacterial keratitis as a first-line treatment without any adjunctive antibiotics with positive results for most patients. In order to distinguish the use of CXL for infectious keratitis treatment from its use for corneal ectatic disorders, a new term was proposed at the 9th CXL congress in Dublin to rename its use in infections as photoactivated chromophore for infectious keratitis -corneal collagen cross-linking (PACK-CXL). -

Ocular Emergencies for the Primary Care Optometrist
Ocular Emergencies Ocular Emergencies for the Disclosure Statement Primary Care Optometrist . Honorarium, Speaker, Consultant, Research Grant: Aerie, Alcon, Allergan, B+L, Carl Zeiss, Glaukos, Heidelberg, Novartis, Topcon, Michael Chaglasian, OD, FAAO Associate Professor Illinois Eye Institute Illinois College of Optometry [email protected] What is a “True” Emergency? “True” Emergency . Pain (vs. discomfort) . History is key to differentiating emergency versus urgency . Current or potential for: Phone or in person Vision loss Proper triage is essential Structural damage After hours protocol Needs immediate (same day) attention Your office and your specialists Medico-legal implications History Emergency Exam Vision Recent ocular disease or One or both eyes? surgery . Acuity . External examination Visual field Other diseases . Visual fields . SLE Sudden or gradual cardiac, vascular, or . Pupils Blurred or lost? autoimmune . IOP Diplopia? viruses . Ocular Motility . Fundus exam Mono or Bino Medications or recent Pain changes to medications Redness Nausea/vomiting Onset Trauma Contact lenses M. Chaglasian, OD 1 Ocular Emergencies Emergency Kit “True” Emergency . Chemical Burns . Eye shield . pH paper Alkaline . Pressure patch . Bandage CL’s . Sterile eye wash . Diamox . Central Retinal Artery Occlusion . Alger brush . Topical drops . Forceps Antibiotics NSAID’s . Golf spud . Both have extremely high risk of severe and permanent Steroids vision loss which can be prevented via immediate Cycloplegics intervention and treatment Chemical Trauma Chemical Burns . Copious irrigation anesthetic . Acid exposure speculum Only penetrate through epithelium sterile saline v tap water car battery, vinegar, and some refrigerants . Contacts can be removed after irrigation . Sweep fornices – repeatedly . Alkaline exposure Penetrates tissues more easily and . Examination after irrigation and neutralization of pH have a prolonged effect . -

Management of Corneal Perforation Vishal Jhanji, MD,1,2,3 Alvin L
SURVEY OF OPHTHALMOLOGY VOLUME 56 NUMBER 6 NOVEMBER–DECEMBER 2011 MAJOR REVIEW Management of Corneal Perforation Vishal Jhanji, MD,1,2,3 Alvin L. Young, MMedSc (Hons), FRCSI,3 Jod S. Mehta, MD,4 Namrata Sharma, MD,5 Tushar Agarwal, MD,5 and Rasik B. Vajpayee, MS, FRCS (Edin), FRANZCO1,5,6 1Centre for Eye Research Australia, University of Melbourne, Australia; 2Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong, Hong Kong; 3Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong; 4Singapore National Eye Centre, Singapore; 5Dr Rajendra Prasad Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi, India; and 6Royal Victorian Eye and Ear Hospital, Melbourne, Australia Abstract. Corneal perforation may be associated with prolapse of ocular tissue and requires prompt diagnosis and treatment. Although infectious keratitis is an important cause, corneal xerosis and collagen vascular diseases should be considered in the differential diagnosis, especially in cases that do not respond to conventional medical therapy. Although medical therapy is a useful adjunct, a surgical approach is required for most corneal perforations. Depending on the size and location of the corneal perforation, treatment options include gluing, amniotic membrane transplantation, and corneal transplantation. (Surv Ophthalmol 56:522--538, 2011. Ó 2011 Elsevier Inc. All rights reserved.) Key words. corneal perforation diagnosis keratoplasty management patch graft therapeutic keratoplasty I. Introduction The selection of an appropriate treatment option is Corneal perforation is a cause of ocular morbidity mostly guided by size and location of the perfora- and profound visual loss.13,119 It is the end result of tion and the status of the underlying disease. -

Is Myopia Related to Intraocular Pressure
Br J Ophthalmol: first published as 10.1136/bjo.88.1.1-a on 23 December 2003. Downloaded from Creig Hoyt Editor IS MYOPIA RELATED TO empirical treatment of corneal ulcers—for example, aminoglycosides, cephalospor- ins, and fluoroquinones. Emergence of resistant strains is a major concern when INTRAOCULAR PRESSURE? antibiotics such as fluoroquinones are used as monotherapy. Bosscha and coworkers The precise aetiological factors respon- report the results of a retrospective study of 91 patients with bacterial ulcers treated sible for the development of myopia are with a topical combination of polymyxin B, neomycin, and gramicidin. In this study incompletely understood. Intraocular this combination was effective in the safe treatment of suspected corneal ulceration. pressure is one of several factors impli- Among 91 patients there were four perforations and one evisceration. cated in the pathogenesis of myopia. It See p 25 has been postulated that elevated intraocular pressure would create RISK FACTORS FOR ACUTE ENDOPHTHALMITIS scleral stress resulting in axial elonga- Acute infectious endophthalmitis remains a vision threatening complication of tion. Lee and coworkers report a study cataract. Although rare, it is a serious and dreaded complication. Wong and Chee of 636 Chinese children age 9–11 years report a retrospective case controlled study of 34 patients with acute endophthalmi- who underwent non-contact tonome- tis presenting within 6 weeks after cataract surgery. Three controls per case were try, cycloplegic autorefraction, and A- randomly selected from cataract surgery lists matched on the date of operation of scan biometry. There were no signifi- cases. This study suggests that the use of silicone intraocular lenses and/or rupture of cant intraocular pressure differences posterior capsule are risk factors for the development of acute endophthalmitis after between low or high myopes and cataract surgery. -

Clinical Case Revista Colombiana De Ciencias Pecuarias
Estrada RD et al Melting ulcer in a colt 31 Clinical case Revista Colombiana de Ciencias Pecuarias Melting ulcer in a colt: clinical management and evolution ¤ Úlcera fundente en un potro: manejo clínico y evolución Úlcera colagenolítica em um potro: manejo clínico e evolução Rubén D Estrada 1, MV; Susana Penagos 2, est MV; Elizabeth Viera 2, est MV; Paula A Angulo 2, est MV; Maria P Arias 2*, MV, MS, PhD. 1MV Actividad independiente 2Facultad de Medicina Veterinaria y Zootecnia, Universidad CES, AA 054591, Medellín, Colombia (Received: June 1, 2012; accepted: November 19, 2012) Summary Anamnesis : a colt showing a whitish coloration accompanied by abundant secretion on the left eye was examined. Clinical and laboratory findings: at ophthalmological examination, signs of melting ulcer were observed. Culture isolation revealed positive growing of Flavobacterium sp. and Gram-negative rods. Treatment approach : several keratectomies and tarsorrhaphies, as well as exhaustive antiproteinases, anti- inflammatory, and antibiotic treatments, were conducted. Treatment focused on reducing inflammatory response, eliminating infective organisms, and promoting epithelial healing. Colt showed complete recovery of vision after 3 months. Conclusions: clinical management of melting ulcer implies exhaustive, though unexpensive, treatment. Key words: cornea, keratectomy, keratomalacia, ophthalmology, tarsorrhaphy Resumen Anamnesis : se examinó un potro que presentó una coloración blanquecina acompañada de abundante secreción en el ojo izquierdo. Hallazgos clínicos y de laboratorio : al examen oftalmológico se observaron signos de ulcera fundente. El aislamiento por cultivo mostró crecimiento de Flavobacterium sp. y cocos Gram negativos. Abordaje terapéutico : se realizaron varias queratectomías y tarsorrafias, además de un tratamiento exhaustivo con antiproteinasas, antiinflamatorios y antibióticos enfocado a reducir la respuesta inflamatoria, eliminar los microorganismos infecciosos y promover la cicatrización epitelial. -

Treatment of Peripheral Corneal Ulcers by Limbal Conjunctivectomy
Brit. 7. Ophthal. (I 976) 6o, 713 Br J Ophthalmol: first published as 10.1136/bjo.60.10.713 on 1 October 1976. Downloaded from Treatment of peripheral corneal ulcers by limbal conjunctivectomy FRED M. WILSON II, MERRILL GRAYSON, AND FORREST D. ELLIS From the Department of Ophthalmology, Indiana University School of Medicine, Indianapolis, Indiana Peripheral corneal ulcers can still pose difficult appear within the ulcer about one week later, followed clinical problems despite therapeutic advances such in a few days by superficial vascularization. The ulcer as specific antimicrobial agents, collagenase inhibi- had healed and epithelialized three weeks after surgery tors, heparin, ocular lubricants, biological adhe- (Fig. ib) and L-cysteine and heparin drops were con- sives, and soft contact lenses. This paper reports tinued for three weeks after it had healed. The ulcer has the healing of several types of progressive marginal ulcers after the excision and recession of adjacent limbal conjunctiva (limbal conjunctivectomy), in some cases after other modes of treatment had been unsuccessful. copyright. Case reports CASE I, MOOREN )S ULCER A 54-year-old Black woman developed a severely painful, largely non-infiltrative ulcer of the nasal left cornea. The ulcer had an overhanging central edge and progressed circumferentially during a period of one year to involve nearly the entire comeal periphery http://bjo.bmj.com/ (Fig. ia). Progression occurred despite treatment at various times with acetylcysteine drops, L-cysteine drops, topical and subconjunctival heparin, artificial soft contact a short trial of tears, lens, topical cortico- (Ia.) steroids, and a trial without any treatment to minimize the possibility of overtreatment.