Scaphoid Variation and an Anatomical Basis for Variable Carpal Mechanics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Proximal Interphalangeal Joint: Arthritis and Deformity
4.1800EOR0010.1302/2058-5241.4.180042 research-article2019 EOR | volume 4 | June 2019 DOI: 10.1302/2058-5241.4.180042 Instructional Lecture: Hand & Wrist www.efortopenreviews.org The proximal interphalangeal joint: arthritis and deformity Daniel Herren Finger joints are of the most common site of osteoarthritis Most authors, especially in the rheumatology and arthritis and include the DIP, PIP and the thumb saddle joint. literature, use a modification of the Kellgren and Lawrence 1 Joint arthroplasty provides the best functional outcome scale, initially described for patellofemoral arthritis, for for painful destroyed PIP joints, including the index finger. radiographic classification: Adequate bone stock and functional tendons are required for a successful PIP joint replacement Grade 1: doubtful narrowing of joint space and pos- sible osteophytic lipping Fixed swan-neck and boutonnière deformity are better served with PIP arthrodesis rather than arthroplasty. Grade 2: definite osteophytes, definite narrowing of joint space Silicone implants are the gold standard in terms of implant choice. Newer two-component joints may have potential Grade 3: moderate multiple osteophytes, definite nar- to correct lateral deformities and improve lateral stability. rowing of joint space, some sclerosis and possible deformation of bone contour Different surgical approaches are used for PIP joint implant arthroplasty according to the needs and the experience of Grade 4: large osteophytes, marked narrowing of joint the surgeon. space, severe sclerosis and definite deformation of bone contour Post-operative rehabilitation is as critical as the surgical procedure. Early protected motion is a treatment goal. Revision and exchange PIP arthroplasty may successfully Treatment be used to treat chronic pain, but will not correct defor- mity. -
Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole with Concurrent Scapholunate Dissociation
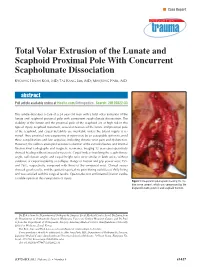
n Case Report Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole With Concurrent Scapholunate Dissociation KYOUNG HWAN KOH, MD; TAE KANG LIM, MD; MIN JONG PARK, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20120822-33 This article describes a case of a 24-year-old man with a total volar extrusion of the lunate and scaphoid proximal pole with concurrent scapholunate dissociation. The viability of the lunate and the proximal pole of the scaphoid are at high risk in this type of injury. Scaphoid nonunion, avascular necrosis of the lunate and proximal pole of the scaphoid, and carpal instability are inevitable unless the blood supply is re- stored. Thus, proximal row carpectomy at injury may be an acceptable option to avoid these complications and late sequelae, including chronic wrist pain and dysfunction. However, the authors attempted accurate reduction of the extruded bones and internal fixation.Final radiographs and magnetic resonance imaging 12 years postoperatively showed healing without avascular necrosis. Carpal indices involving the scapholunate angle, radiolunate angle, and carpal height ratio were similar in both wrists without evidence of carpal instability or collapse. Range of motion and grip power were 75% and 76%, respectively, compared with those of the uninjured wrist. Clinical scores showed good results, and the patient reported no pain during activities of daily living and was satisfied with his surgical results. Open reduction and internal fixation can be a viable option in this rare pattern of injury. Figure: Intraoperative photograph showing the me- dian nerve (arrow), which was compressed by the displaced lunate (asterisk) and scaphoid fracture. -

Module 6 : Anatomy of the Joints
Module 6 : Anatomy of the Joints In this module you will learn: About the classification of joints What synovial joints are and how they work Where the hinge joints are located and their functions Examples of gliding joints and how they work About the saddle joint and its function 6.1 Introduction The body has a need for strength and movement, which is why we are rigid. If our bodies were not made this way, then movement would be impossible. We are designed to grow with bones, tendons, ligaments, and joints that all play a part in natural movements known as articulations – these strong connections join up bones, teeth, and cartilage. Each joint in our body makes these links possible and each joint performs a specific job – many of them differ in shape and structure, but all control a range of motion between the body parts that they connect. 6.2 Classifying Joints Joints that do not allow movement are known as synarthrosis joints. Examples of synarthroses are sutures of the skull, and the gomphoses which connect our teeth to the skull. Amphiarthrosis joints allow a small range of movement, an example of this is your intervertebral discs attached to the spine. Another example is the pubic symphysis in your hip region. The freely moving joints are classified as diarthrosis joints. These have a higher range of motion than any other type of joint, they include knees, elbows, shoulders, and wrists. Joints can also be classified depending on the kind of material each one is structurally made up of. A fibrous joint is made up of tough collagen fiber, examples of this are previously mentioned sutures of the skull or the syndesmosis joint, which holds the ulna and radius of your forearm in place. -

Joints Classification of Joints
Joints Classification of Joints . Functional classification (Focuses on amount of movement) . Synarthroses (immovable joints) . Amphiarthroses (slightly movable joints) . Diarthroses (freely movable joints) . Structural classification (Based on the material binding them and presence or absence of a joint cavity) . Fibrous mostly synarthroses . Cartilagenous mostly amphiarthroses . Synovial diarthroses Table of Joint Types Functional across Synarthroses Amphiarthroses Diarthroses (immovable joints) (some movement) (freely movable) Structural down Bony Fusion Synostosis (frontal=metopic suture; epiphyseal lines) Fibrous Suture (skull only) Syndesmoses Syndesmoses -fibrous tissue is -ligaments only -ligament longer continuous with between bones; here, (example: radioulnar periosteum short so some but not interosseous a lot of movement membrane) (example: tib-fib Gomphoses (teeth) ligament) -ligament is periodontal ligament Cartilagenous Synchondroses Sympheses (bone united by -hyaline cartilage -fibrocartilage cartilage only) (examples: (examples: between manubrium-C1, discs, pubic epiphyseal plates) symphesis Synovial Are all diarthrotic Fibrous joints . Bones connected by fibrous tissue: dense regular connective tissue . No joint cavity . Slightly immovable or not at all . Types . Sutures . Syndesmoses . Gomphoses Sutures . Only between bones of skull . Fibrous tissue continuous with periosteum . Ossify and fuse in middle age: now technically called “synostoses”= bony junctions Syndesmoses . In Greek: “ligament” . Bones connected by ligaments only . Amount of movement depends on length of the fibers: longer than in sutures Gomphoses . Is a “peg-in-socket” . Only example is tooth with its socket . Ligament is a short periodontal ligament Cartilagenous joints . Articulating bones united by cartilage . Lack a joint cavity . Not highly movable . Two types . Synchondroses (singular: synchondrosis) . Sympheses (singular: symphesis) Synchondroses . Literally: “junction of cartilage” . Hyaline cartilage unites the bones . Immovable (synarthroses) . -

38.3 Joints and Skeletal Movement.Pdf
1198 Chapter 38 | The Musculoskeletal System Decalcification of Bones Question: What effect does the removal of calcium and collagen have on bone structure? Background: Conduct a literature search on the role of calcium and collagen in maintaining bone structure. Conduct a literature search on diseases in which bone structure is compromised. Hypothesis: Develop a hypothesis that states predictions of the flexibility, strength, and mass of bones that have had the calcium and collagen components removed. Develop a hypothesis regarding the attempt to add calcium back to decalcified bones. Test the hypothesis: Test the prediction by removing calcium from chicken bones by placing them in a jar of vinegar for seven days. Test the hypothesis regarding adding calcium back to decalcified bone by placing the decalcified chicken bones into a jar of water with calcium supplements added. Test the prediction by denaturing the collagen from the bones by baking them at 250°C for three hours. Analyze the data: Create a table showing the changes in bone flexibility, strength, and mass in the three different environments. Report the results: Under which conditions was the bone most flexible? Under which conditions was the bone the strongest? Draw a conclusion: Did the results support or refute the hypothesis? How do the results observed in this experiment correspond to diseases that destroy bone tissue? 38.3 | Joints and Skeletal Movement By the end of this section, you will be able to do the following: • Classify the different types of joints on the basis of structure • Explain the role of joints in skeletal movement The point at which two or more bones meet is called a joint, or articulation. -

Spline Joints for Multibody Dynamics
To appear in the ACM SIGGRAPH conference proceedings Spline Joints for Multibody Dynamics Sung-Hee Lee∗ Demetri Terzopoulos† University of California, Los Angeles Figure 1: A spline joint can much more accurately model complex biological joints than is possible using conventional joint models. Abstract When it comes to designing practical machines, using only the lower pair joints seems reasonable, not because they are ideal Spline joints are a novel class of joints that can model general scle- choices for every mechanism, but because it is difficult to man- ronomic constraints for multibody dynamics based on the minimal- ufacture more complex types of joints. For the same reason, coordinates formulation. The main idea is to introduce spline the creation of more sophisticated joints has been largely ne- curves and surfaces in the modeling of joints: We model 1-DOF glected in multibody dynamics research. Not surprisingly, there- joints using splines on SE(3), and construct multi-DOF joints as fore, most dynamics simulators and game physics engines, such the product of exponentials of splines in Euclidean space. We as ADAMS (www.mscsoftware.com), the Open Dynamics Engine present efficient recursive algorithms to compute the derivatives of (www.ode.org), and SD/FAST (www.sdfast.com), provide only the spline joint, as well as geometric algorithms to determine op- fairly simple types of joint models limited to fixed joint axes. timal parameters in order to achieve the desired joint motion. Our spline joints can be used to create interesting new simulated mecha- By contrast, more complex joints are common in biological sys- nisms for computer animation and they can more accurately model tems. -

Lunate Flattening in Rheumatoid Wrists
Central Annals of Orthopedics & Rheumatology Research Article *Corresponding author Ryogo Nakamura, Nagoya Hand Center, Chunichi Hospital, 3-12-3 Marunouchi, Naka-ku, Nagoya 460- Lunate Flattening in 0002, Japan, Email: Submitted: 04 February 2014 Accepted: 28 May 2014 Rheumatoid Wrists Published: 30 May 2014 Ryogo Nakamura1, Satoshi Niwa1, Sayako Takahashi1, Etushiro Copyright © 2014 Nakamura et al. Naka1 and Masahiro Tatebe2* 1Nagoya Hand Center Chunichi Hospital, Nagoya, Japan OPEN ACCESS 2Hand and Microsurgery Center Anjo Kosei Hospital, Japan Abstract Lunate flattening was studied in 36 patients (62 wrists) with rheumatoid arthritis (RA) who were age- and gender-matched to people with normal wrists. The carpal height ratio (CHR) and lunate compression ratio (LCR; lunate height/ lunate diameter×100, Ståhl index) were measured from wrist radiographs of both groups and the lunate flattening ratio (LFR) was calculated by dividing the LCR by the CHR. The LFR reflects lunate flattening compared to carpal collapse. Twenty-four wrists underwent MRI study. T1-weighted images were evaluated for bone necrosis of the lunate. Results: the normal LFR value obtained from normal wrists ranged from 79.9 to 113.5 (mean±2SD). Lunates with RA could be classified into three groups by LFR values- lunates with a LFR above 113.5 (10 wrists, 16%), lunates with a LFR within the normal range (34 wrists, 55%), and lunates with a LFR lower than 79.9 (18 wrists, 29%). Twelve (50%) of the 24 wrists that underwent MRI study showed a low signal of the lunate in T1-weighted images showing osteonecrosis. Although a satisfactory cor- relation was not confirmed between a LFR value and a low signal on T1-weighted im- ages, lunate avascular necrosis was suspected to play a role in flattening of the lunate. -

A Thesis Entitled the Effects of Radial Core Decompression on Lunate
A Thesis entitled The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering Dr. Mohamed Samir Hefzy, Committee Chair Dr. Vijay Goel, Committee Member Dr. Michael Dennis, Committee Member Dr. Abdul-Azim Mustapha, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo May 2012 Copyright 2012, Andrew E. Smith This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering The University of Toledo May 2012 Kienbocks disease causes degeneration of the lunate bone in the wrist leading to pain and reduced function of the joint. Clinical studies have found a new technique, radial core decompression (RCD) to be clinically effective in improving early stage Kienbock's disease. However, there have been no biomechanical studies characterizing the changes in wrist kinematics following the RCD procedure. The purpose of this study is to determine the changes in lunate and scaphoid motions following the RCD procedure. This study employs an electromagnetic 3-dimensional tracking system, Polhemus 3-SPACE to measure the motions of the lunate, scaphoid, and third metacarpal in four cadaveric specimens. Specimens were partially dissected and sutures were attached to five major tendons used for wrist motion. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Biomechanics
BIOMECHANICS SAGAR BIOMECHANICS The study of mechanics in the human body is referred to as biomechanics. Biomechanics Kinematics Kinetics U Kinematics: Kinematics is the area of biomechanics that includes descriptions of motion without regard for the forces producing the motion. [It studies only the movements of the body.] Kinematics variables for a given movement may include following: y Type of motion. y Location of motion. y Direction of motion. y Magnitude of motion. y Rate or Duration of motion. Ö Type of Motion: There are four types of movement that can be attributed to any rigid object or four pathways through which a rigid object can travel. < Rotatory (Angular) Motion: It is movement of an object or segment around a fixed axis in a curved path. Each point on the object or segment moves through the same angle, at the same time, at a constant distance from the axis of rotation. Eg – Each point in the forearm/hand segment moves through the same angle, in the same time, at a constant distance from the axis of rotation during flexion at the elbow joint. < Translatory (Linear) Motion: It is the movement of an object or segment in a straight line. Each point on the object moves through the same distance, at the same time, in parallel paths. Translation of a body segment without some concomitant rotation rarely occurs. EgSAGAR – The movement of the combined forearm/hand segment to grasp an object, in this all points on the forearm/hand segment move through the same distance at the same time but the translation of the forearm/hand segment is actually produced by rotation of both the shoulder and the elbow joints. -

Ulnar Variance and the Shape of the Lunate Bone a Radiological Investigation
ULNAR VARIANCE AND THE SHAPE OF THE LUNATE BONE A RADIOLOGICAL INVESTIGATION A. H. SCHUURMAN1, M. MAAS2, P. F. DIJKSTRA2, J. M. G. KAUER3 The authors designed a study to test the hypothesis Ulnar variance is the roentgenographic difference that the length of the ulna might affect the shape of of the length of the ulna relative to the radius. the lunate bone because of long-term molding during Positive ulna variance or ulna plus refers to an ulna life. This might then be useful to predict the presence longer than the radius, while the opposite is true in or absence of a dynamic or static ulna plus by the the ulna minus or negative ulnar variance. shape of the lunate bone. Obermann (6) correlated lunate shape and ulnar In a prospective study, posterior-anterior wrist xrays length in 68 patients. Although he found a 13% were taken in a standard fashion in 68 patients with a mean age of 34.5 years. Dominance, grip strength, incidence of type 1, 62% type 2 and 25% type 3, he ulnar variance and the shape of the lunate were found no correlation between type 1 and ulna recorded. length (even distribution in all). Type 2 was found Lunate shape, type 1, which is the least molded, was less often in the ulna minus group and type 3 was seen most frequently on both the left and right side most often found in the ulna plus group. Unfortu- and did not correlate with the dominant side. The nately no statistical analysis was performed. -

Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child
ISSN: 2469-5726 Roberts et al. J Rheum Dis Treat 2018, 4:063 DOI: 10.23937/2469-5726/1510063 Volume 4 | Issue 2 Journal of Open Access Rheumatic Diseases and Treatment CASE REPORT Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child with Systemic Lupus Erythematosus Roberts DC1*, Jester A1, Southwood T2, Johnson K3 and Oestreich K1 1 Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK Check for 2Department of Rheumatology, Birmingham Children’s Hospital, UK updates 3Department of Radiology, Birmingham Children’s Hospital, UK *Corresponding author: Darren Roberts, Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK, E-mail: [email protected] We present, to our knowledge, the first case of syn- Abstract chronous lunate and triquetral AVN in a child with SLE. Avascular necrosis is a known complication of systemic lu- The aetiology and management of carpal AVN in child- pus erythematosus. We report an unusual case of avas- cular necrosis affecting both the lunate and triquetrum in a hood SLE are also discussed based on the available lit- child with this condition. Vasculitis, synovitis and IgM anti- erature. cardiolipin antibodies were probable predisposing factors. The use of arthroscopic synovial debridement improves Case Report symptoms even in the presence of carpal chondromalacia and potentially delays the need for salvage surgery. A 14-year-old girl, diagnosed with SLE five years pre- viously, presented with a two-year history of non-trau- Introduction matic pain and stiffness of her right dominant wrist. She was able to write and self-care, however she was unable Avascular necrosis (AVN) of the carpus typically af- to partake in hand-held ball and racquet sports at school.