3D Printed Anatomy Series Human Anatomy Reproductions with an Extra Dimension
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ANGIOGRAPHY of the UPPER EXTREMITY Printed in the Netherlands by Koninklijke Drukkerij G.J.Thieme Bv, Nijmegen ANGIOGRAPHY of the UPPER EXTREMITY
1 f - h-' ^^ ANGIOGRAPHY OF THE UPPER EXTREMITY Printed in The Netherlands by Koninklijke drukkerij G.J.Thieme bv, Nijmegen ANGIOGRAPHY OF THE UPPER EXTREMITY PROEFSCHRIFT ter verkrijging van de graad van Doctor in de Geneeskunde aan de Rijksuniversiteit te Leiden, op gezag van de Rector Magni- ficus Dr. A. A. H. Kassenaar, Hoogleraar in de faculteit der Geneeskunde, volgens besluit van het college van dekanen te verdedigen op donderdag 6 mei 1982 te klokke 15.15 uur DOOR BLAGOJA K. JANEVSKI geborcn 8 februari 1934 te Gradsko, Joegoslavie MARTINUS NIJHOFF PUBLISHERS THE HAGUE - BOSTON - LONDON 1982 PROMOTOR: Prof. Dr. A. E. van Voorthuisen REPERENTEN: Prof. Dr. J. M. F. LandLandsmees r 1 Prof. Dr. J. L. Terpstra ! I Copyright © 1982 by Martinus Nijhoff Publishers, The Hague All rights reserved. No part of this publication may be repro- duced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, photocopying, recording, or otherwise, without the prior written permission of the pub- lishers, Martinus Nijhoff Publishers,P.O. Box 566,2501 CN The Hague, The Netherlands if ••»• 7b w^ wife Charlotte To Lucienne, Lidia and Dejan h {, ,;T1 ii-"*1 ™ ffiffp"!»3^>»'*!W^iyJiMBiaMMrar^ ACKNOWLEDGEMENTS This thesis was produced in the Department of Radiology, Sirit Annadal Hospital, Maastricht. i Case material: Prof. Dr. H. A. J. Lemmens, surgeon. Technical assistence: Miss J. Crijns, Mrs. A. Rousie-Panis, Miss A. Mordant and Miss H. Nelissen. Secretarial help: Mrs. M. Finders-Velraad and Miss Y. Bessems. Photography: Mr. C. Evers. Graphical illustrations: Mr. C. Voskamp. Correction English text: Dr. -

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -

The Variations of the Subclavian Artery and Its Branches Ahmet H
Okajimas Folia Anat. Jpn., 76(5): 255-262, December, 1999 The Variations of the Subclavian Artery and Its Branches By Ahmet H. YUCEL, Emine KIZILKANAT and CengizO. OZDEMIR Department of Anatomy, Faculty of Medicine, Cukurova University, 01330 Balcali, Adana Turkey -Received for Publication, June 19,1999- Key Words: Subclavian artery, Vertebral artery, Arterial variation Summary: This study reports important variations in branches of the subclavian artery in a singular cadaver. The origin of the left vertebral artery was from the aortic arch. On the right side, no thyrocervical trunk was found. The two branches which normally originate from the thyrocervical trunk had a different origin. The transverse cervical artery arose directly from the subclavian artery and suprascapular artery originated from the internal thoracic artery. This variation provides a short route for posterior scapular anastomoses. An awareness of this rare variation is important because this area is used for diagnostic and surgical procedures. The subclavian artery, the main artery of the The variations of the subclavian artery and its upper extremity, also gives off the branches which branches have a great importance both in blood supply the neck region. The right subclavian arises vessels surgery and in angiographic investigations. from the brachiocephalic trunk, the left from the aortic arch. Because of this, the first part of the right and left subclavian arteries differs both in the Subjects origin and length. The branches of the subclavian artery are vertebral artery, internal thoracic artery, This work is based on a dissection carried out in thyrocervical trunk, costocervical trunk and dorsal the Department of Anatomy in the Faculty of scapular artery. -

Head & Neck Muscle Table
Robert Frysztak, PhD. Structure of the Human Body Loyola University Chicago Stritch School of Medicine HEAD‐NECK MUSCLE TABLE PROXIMAL ATTACHMENT DISTAL ATTACHMENT MUSCLE INNERVATION MAIN ACTIONS BLOOD SUPPLY MUSCLE GROUP (ORIGIN) (INSERTION) Anterior floor of orbit lateral to Oculomotor nerve (CN III), inferior Abducts, elevates, and laterally Inferior oblique Lateral sclera deep to lateral rectus Ophthalmic artery Extra‐ocular nasolacrimal canal division rotates eyeball Inferior aspect of eyeball, posterior to Oculomotor nerve (CN III), inferior Depresses, adducts, and laterally Inferior rectus Common tendinous ring Ophthalmic artery Extra‐ocular corneoscleral junction division rotates eyeball Lateral aspect of eyeball, posterior to Lateral rectus Common tendinous ring Abducent nerve (CN VI) Abducts eyeball Ophthalmic artery Extra‐ocular corneoscleral junction Medial aspect of eyeball, posterior to Oculomotor nerve (CN III), inferior Medial rectus Common tendinous ring Adducts eyeball Ophthalmic artery Extra‐ocular corneoscleral junction division Passes through trochlea, attaches to Body of sphenoid (above optic foramen), Abducts, depresses, and medially Superior oblique superior sclera between superior and Trochlear nerve (CN IV) Ophthalmic artery Extra‐ocular medial to origin of superior rectus rotates eyeball lateral recti Superior aspect of eyeball, posterior to Oculomotor nerve (CN III), superior Elevates, adducts, and medially Superior rectus Common tendinous ring Ophthalmic artery Extra‐ocular the corneoscleral junction division -

Normal Gross and Histologic Features of the Gastrointestinal Tract
NORMAL GROSS AND HISTOLOGIC 1 FEATURES OF THE GASTROINTESTINAL TRACT THE NORMAL ESOPHAGUS left gastric, left phrenic, and left hepatic accessory arteries. Veins in the proximal and mid esopha- Anatomy gus drain into the systemic circulation, whereas Gross Anatomy. The adult esophagus is a the short gastric and left gastric veins of the muscular tube measuring approximately 25 cm portal system drain the distal esophagus. Linear and extending from the lower border of the cri- arrays of large caliber veins are unique to the distal coid cartilage to the gastroesophageal junction. esophagus and can be a helpful clue to the site of It lies posterior to the trachea and left atrium a biopsy when extensive cardiac-type mucosa is in the mediastinum but deviates slightly to the present near the gastroesophageal junction (4). left before descending to the diaphragm, where Lymphatic vessels are present in all layers of the it traverses the hiatus and enters the abdomen. esophagus. They drain to paratracheal and deep The subdiaphragmatic esophagus lies against cervical lymph nodes in the cervical esophagus, the posterior surface of the left hepatic lobe (1). bronchial and posterior mediastinal lymph nodes The International Classification of Diseases in the thoracic esophagus, and left gastric lymph and the American Joint Commission on Cancer nodes in the abdominal esophagus. divide the esophagus into upper, middle, and lower thirds, whereas endoscopists measure distance to points in the esophagus relative to the incisors (2). The esophagus begins 15 cm from the incisors and extends 40 cm from the incisors in the average adult (3). The upper and lower esophageal sphincters represent areas of increased resting tone but lack anatomic landmarks; they are located 15 to 18 cm from the incisors and slightly proximal to the gastroesophageal junction, respectively. -

Complications Associated with Clavicular Fracture
NOR200061.qxd 9/11/09 1:23 PM Page 217 Complications Associated With Clavicular Fracture George Mouzopoulos ▼ Emmanuil Morakis ▼ Michalis Stamatakos ▼ Mathaios Tzurbakis The objective of our literature review was to inform or- subclavian vein, due to its stable connection with the thopaedic nurses about the complications of clavicular frac- clavicle via the cervical fascia, can also be subjected to ture, which are easily misdiagnosed. For this purpose, we injuries (Casbas et al., 2005). Damage to the internal searched MEDLINE (1965–2005) using the key words clavicle, jugular vein, the suprascapular artery, the axillary, and fracture, and complications. Fractures of the clavicle are usu- carotid artery after a clavicular fracture has also been ally thought to be easily managed by symptomatic treatment reported (Katras et al., 2001). About 50% of injuries to the subclavian arteries are in a broad arm sling. However, it is well recognized that not due to fractures of the clavicle because the proximal all clavicular fractures have a good outcome. Displaced or part is dislocated superiorly by the sternocleidomas- comminuted clavicle fractures are associated with complica- toid, causing damage to the vessel (Sodhi, Arora, & tions such as subclavian vessels injury, hemopneumothorax, Khandelwal, 2007). If no injury happens during the ini- brachial plexus paresis, nonunion, malunion, posttraumatic tial displacement of the fractured part, then it is un- arthritis, refracture, and other complications related to os- likely to happen later, because the distal segment is dis- teosynthesis. Herein, we describe what the orthopaedic nurse placed downward and forward due to shoulder weight, should know about the complications of clavicular fractures. -

Dr. Neelesh Kanasker Original Research Paper Anatomy Dr.Preeti
Original Research Paper Volume - 11 | Issue - 04 | April - 2021 | PRINT ISSN No. 2249 - 555X | DOI : 10.36106/ijar Anatomy SURGICAL IMPORTANCE OF VARIABLE BRANCHING PATTERN OF THYROCERVICAL TRUNK IN NECK ROOT SURGERIES Dr. Neelesh Associate professor, Department of Anatomy, Dr. D. Y. Patil Medical College, Hospital Kanasker and Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. Professor, Department of Anatomy, Dr. D. Y. Patil Medical College, Hospital and Dr.Preeti Sonje* Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. *Corresponding Author Dr. P. Professor and Director Academics, Department of Anatomy, Dr. D. Y. Patil Medical Vatsalaswamy College, Hospital and Research Center, Dr.D.Y.Patil Vidyapeeth , Pimpri Pune. ABSTRACT Objectives: Variations in the arteries of human body are important clinically as well as anatomically. Accurate knowledge and understanding of anomalous variations in the origin and course of arteries have serious implications in angiographic and surgical procedures hence it is of great importance to be aware of such possibilities of variations. Background and Results: Thyrocervical Trunk is short wide vessel arising from rst part of subclavian artery and divides into its three terminal branches i.e. Suprascapular, Inferior Thyroid and Transverse cervical artery. 30 formalin xed cadavers were dissected to study variations in Thyrocervical Trunk and its branches if any. Conclusion: Awareness of variations in the origin and branching pattern is of utmost importance during Doppler scanning of blood vessels for clinical diagnosis and surgical management and to avoid major complications in head and neck surgeries. KEYWORDS : Thyrocervical Trunk, Anomalous variations, Doppler scanning, Head and neck surgeries. INTRODUCTION anterior muscle and then arches medially at the level of C7 vertebra Subclavian artery is the artery of upper limb, but is supplies a between the vertebral vessels behind and carotid sheath in front. -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz. -
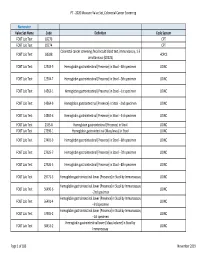
2020 Measure Value Set Colorectal Cancer Screening
PT ‐ 2020 Measure Value Set_Colorectal Cancer Screening Numerator Value Set Name Code Definition Code System FOBT Lab Test 82270 CPT FOBT Lab Test 82274 CPT Colorectal cancer screening; fecal occult blood test, immunoassay, 1‐3 FOBT Lab Test G0328 HCPCS simultaneous (G0328) FOBT Lab Test 12503‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐4th specimen LOINC FOBT Lab Test 12504‐7 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐5th specimen LOINC FOBT Lab Test 14563‐1 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐1st specimen LOINC FOBT Lab Test 14564‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐2nd specimen LOINC FOBT Lab Test 14565‐6 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐3rd specimen LOINC FOBT Lab Test 2335‐8 Hemoglobin.gastrointestinal [Presence] in Stool LOINC FOBT Lab Test 27396‐1 Hemoglobin.gastrointestinal [Mass/mass] in Stool LOINC FOBT Lab Test 27401‐9 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐6th specimen LOINC FOBT Lab Test 27925‐7 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐7th specimen LOINC FOBT Lab Test 27926‐5 Hemoglobin.gastrointestinal [Presence] in Stool ‐‐8th specimen LOINC FOBT Lab Test 29771‐3 Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay LOINC Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 56490‐6 LOINC ‐‐2nd specimen Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 56491‐4 LOINC ‐‐3rd specimen Hemoglobin.gastrointestinal.lower [Presence] in Stool by Immunoassay FOBT Lab Test 57905‐2 -

The Rare Origin of the Suprascapular Artery Arising Off The
eISSN 1308-4038 International Journal of Anatomical Variations (2011) 4: 182–184 Case Report The rare origin of the suprascapular artery arising off the internal thoracic artery in the presence of the thyrocervical trunk: clinical and surgical implications Published online December 2nd, 2011 © http://www.ijav.org Stavros ATSAS ABSTRACT Jacob N. FOX During routine dissection of the subclavian artery and its branches, the suprascapular artery was found arising from H. Wayne LAMBERT the proximal end of the internal thoracic artery in only the left side of a 68-year-old Caucasian male, despite the presence of the thyrocervical trunk on the ipsilateral side. The suprascapular artery ran deep to the proximal one- third of the clavicle then continued its usual course, running parallel to the suprascapular nerve and passing over the superior transverse scapular ligament distally. Knowledge of this variant origin of the suprascapular artery is clinically Department of Neurobiology and Anatomy, West Virginia University School of Medicine, important because the internal thoracic artery is utilized for a majority of the 800,000 coronary artery bypass surgeries Robert C. Byrd Health Sciences Center, Morgantown, West Virginia, USA. performed worldwide each year. Its course deep to the clavicle is also significant due to clavicular fractures accounting for approximately 5-15% of adult bone fractures. © IJAV. 2011; 4: 182–184. Dr. H. Wayne Lambert, PhD Associate Professor West Virginia University School of Medicine Robert C. Byrd Health Sciences Center Department of Neurobiology and Anatomy HSN 4052; P.O. Box 9128 Morgantown, WV, 26506-9128, USA. +1 304 293-0610 [email protected] Key words [anatomical variant] [suprascapular artery] [internal thoracic artery] [branches of subclavian artery] [thyrocervical trunk] [coronary bypass Received June 21st, 2011; accepted October 12th, 2011 surgery] [radical and modified neck dissections] Introduction In 2005, Weiglein et al. -

Thieme: Lymphedema Management
8 1 Anatomy tween a proximal and a distal pair of valves is called lymph angion (Fig. 1−4). The media in valvular areas of lymph collectors contains less smooth musculature than the angion area. Lymph angions have an autonomic contraction frequency of ෂ10 to 12 contractions per minute at rest (lymphangiomotoricity). In healthy lymph collectors, the proximal valve is open during the systole, whereas the distal valve is closed; in the diastole, the op- posite is the case. This permits directional flow of lymph fluid from distal to proximal angions. In lymphangiectasia (dilation) with valvular insufficiency, the lymph flow may reverse into distal lymph angions (lymphatic reflux). Lymph collectors have the ability to react to an increase in lymph formation with an in- crease in contraction frequency. The increase in lymph fluid entering the lymph angion will cause a stretch on the wall of the angion, which Figure 1−4 Lymph collectors. 1. Lymph collector; 2. Afferent lymph collector to lymph node; 3. Efferent in turn results in an increase in lymphangio- lymph collector from lymph node; 4. Lymph node; 5. motoricity (lymphatic safety factor; see also Cross section through a lymph collector in the area of Chapter 2, Safety Factor of the Lymphatic Sys- the valves; 6. Lymph angion. tem). Other factors that may influence lymphan- giomotoricity are external stretch on the It is postulated that the main purpose of pre- lymph angion wall (e.g., manual lymph collectors is the transport of lymph fluid from drainage), temperature, activity of muscle and the capillaries to lymph collectors. Due to the joint pumps, diaphragmatic breathing, pulsa- capillary-like wall structure in some areas, pre- tion of adjacent arteries, and certain tissue collectors are able to absorb lymphatic loads. -

Arterial Variations of the Subclavian-Axillary Arterial Tree: Its Association with the Supply of the Rotator Cuff Muscles
Int. J. Morphol., 32(4):1436-1443, 2014. Arterial Variations of the Subclavian-Axillary Arterial Tree: Its Association with the Supply of the Rotator Cuff Muscles Variaciones Arteriales del Árbol Arterial Subclavio-Axilar. Su Asociación con la Irrigación del Manguito de los Rotadores N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial variations of the subclavian-axillary arterial tree: Its association with the supply of the rotator cuff muscles. Int. J. Morphol., 32(4):1436-1443, 2014. SUMMARY: The subclavian-axillary arterial tree is responsible for the arterial supply to the rotator cuff muscles as well as other shoulder muscles. This study comprised the bilateral dissection of the shoulder and upper arm region in thirty-one adult and nineteen fetal cadaveric specimens. The variable origins and branching patterns of the axillary, subscapular, circumflex scapular, thoracodorsal, posterior circumflex humeral and suprascapular arteries identified in this study corroborated the findings of previous studies. In addition, unique variations that are unreported in the literature were also observed. The precise anatomy of the arterial distribution to the rotator cuff muscles is important to the surgeon and radiologist. It will aid proper interpretation of radiographic images and avoid injury to this area during surgical procedures. KEY WORDS: Subclavian-axillary arterial tree; Variations; Supply; Rotator cuff muscles. INTRODUCTION Standard anatomical textbooks divide the axillary identified by Saralaya et al. (2008) to arise as a large artery into three parts using its relation to the pectoralis minor collateral branch from the first part of the axillary artery muscle (Salopek et al., 2007).