Introduction to Quantitative EEG and Neurofeedback: Advanced Theory and Applications
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Truth About Fat: the Latest Update February 24Th 2016 Cathy Mazanec, MPH, RDN, CSSD, LDN
The Truth about Fat: The Latest Update February 24th 2016 Cathy Mazanec, MPH, RDN, CSSD, LDN I recently attended a Fat Summit hosted by Integrative and Functional Medicine physician, Mark Hyman, MD, Director of the Center for Functional Medicine at the Cleveland Clinic. Dr. Hyman invited some of the most prestigious U.S. researchers to join this online Summit to share their individual research data. This academic bench of researchers and thought leaders was deep, some of whom included: Ronald Krause, MD; Daniel Amen, MD; Jeffrey Bland, PhD; Michael Roizen, MD; Chris Kresser, MS, LAc; Walter Willett, MD; David Perlmutter, MD; Dean Ornish, MD. I was so excited to finally hear the latest update about dietary fats and end the great fat debate once and for all. What a long awaited relief this would be…… This could not have been further from the truth!! Consistent with the pattern I’ve seen over my 37 year career, nutrition research from highly respected scholars often conflicts. The reason for this is each researcher is looking at a different piece of the same puzzle. In this case, the effect of a certain dietary fat on one piece of the puzzle may be very different from the effect that fat has on another piece of the puzzle. Hence, each researcher may have a different viewpoint and recommendation about the dietary fat being studied. So a lot of questions still remain unanswered but some information is very clear. Here's a snippet of the latest research regarding dietary fat and what we need to know ………. -

Neurodevelopmental Correlates of the Emerging Adult Self T ⁎ Christopher G
Developmental Cognitive Neuroscience 36 (2019) 100626 Contents lists available at ScienceDirect Developmental Cognitive Neuroscience journal homepage: www.elsevier.com/locate/dcn Neurodevelopmental correlates of the emerging adult self T ⁎ Christopher G. Daveya,b,c, , Alex Fornitod,e, Jesus Pujolf, Michael Breakspearg,h, Lianne Schmaala,b, Ben J. Harrisonc a Orygen, The National Centre of Excellence in Youth Mental Health, Parkville, Australia b Centre for Youth Mental Health, The University of Melbourne, Parkville, Australia c Melbourne Neuropsychiatry Centre, Department of Psychiatry, The University of Melbourne, Parkville, Australia d Monash Clinical and Imaging Neuroscience, School of Psychological Sciences, Monash University, Clayton, Australia e Monash Biomedical Imaging, Monash University, Clayton, Australia f MRI Research Unit, Department of Radiology, Hospital del Mar, CIBERSAM G21, Barcelona, Spain g QIMR Berghofer Medical Research Institute, Brisbane, Australia h Hunter Medical Research Institute, University of Newcastle, Newcastle, Australia ARTICLE INFO ABSTRACT Keywords: The self-concept – the set of beliefs that a person has about themselves – shows significant development from Adolescent development adolescence to early adulthood, in parallel with brain development over the same period. We sought to in- Connectivity vestigate how age-related changes in self-appraisal processes corresponded with brain network segregation and Default mode network integration in healthy adolescents and young adults. We scanned 88 participants (46 female), aged from 15 to 25 Functional MRI years, as they performed a self-appraisal task. We first examined their patterns of activation to self-appraisal, and Self replicated prior reports of reduced dorsomedial prefrontal cortex activation with older age, with similar re- ductions in precuneus, right anterior insula/operculum, and a region extending from thalamus to striatum. -

Ud,.Arihuaaa, Yoga Hypaosis
THEODORE X. BARBER UD,.ARIHUAAA, YOGA� HYPAOSIS LSD, Marihuana, Yoga, and Hypnosis Modern Applications of Psychology under the editorship of Joseph D. Matarazzo UNIVERSITY OF OREGON MEDICAL SCHOOL I I I I THEODORE XENOPHON BARBER Medfield State Hospital, Harding, Massachusetts ALDINE PUBLISHING COMPANY Chicago Copyright© 1970 by Theodore X. Barber All rights reserved. No part of this publication may be reproduced or transmitted in any fo rm or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publisher. First published 1970 by Aldine Publishing Company 529 South Wabash Avenue Chicago, lllinois 60605 Library of Congress Catalog Card Number 73-115935 SBN 202-25004-1 Printed in the United States of America To Catherine, Ted, Rania, and Elaine Preface This book is concerned with the psychological and physiological effects of yoga, hypnosis, major psychedelic drugs (LSD, mescaline, and psi locybin), and minor psychedelic drugs (marihuana, hashish, and other cannabis derivatives). These conditions have the following in common: It is generally believed that psychedelic drugs, yoga, and hypnosis give rise to altered states of awareness or consciousness. Psychedelics, yoga, and hypnosis are said to tap unu sed potentialities of man. Psychedelics, yoga, and hypnosis have traditionally been viewed as part of abnormal psychology and as discontinuous from other known psychological phenomena. Each of these conditions has aroused controversy and emotionalism. Although yoga, hypnosis, and some psychedelic drugs such as peyote and cannabis have been known for many years, research on these topics is rather recent. In fact, practically all of the rigorous research in these areas has been carried out by individuals alive today. -

Aesthetic Appreciation of Poetry Correlates with Ease of Processing in Event-Related Potentials
CORE Metadata, citation and similar papers at core.ac.uk Provided by Maastricht University Research Portal Aesthetic appreciation of poetry correlates with ease of processing in event-related potentials Citation for published version (APA): Obermeier, C., Kotz, S. A., Jessen, S., Raettig, T., von Koppenfels, M., & Menninghaus, W. (2016). Aesthetic appreciation of poetry correlates with ease of processing in event-related potentials. Cognitive, Affective, & Behavioral Neuroscience, 16(2), 362-373. https://doi.org/10.3758/s13415-015-0396-x Document status and date: Published: 01/04/2016 DOI: 10.3758/s13415-015-0396-x Document Version: Publisher's PDF, also known as Version of record Please check the document version of this publication: • A submitted manuscript is the version of the article upon submission and before peer-review. There can be important differences between the submitted version and the official published version of record. People interested in the research are advised to contact the author for the final version of the publication, or visit the DOI to the publisher's website. • The final author version and the galley proof are versions of the publication after peer review. • The final published version features the final layout of the paper including the volume, issue and page numbers. Link to publication General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. -

Quantitative EEG (QEEG) Analysis of Emotional Interaction Between Abusers and Victims in Intimate Partner Violence: a Pilot Study
brain sciences Article Quantitative EEG (QEEG) Analysis of Emotional Interaction between Abusers and Victims in Intimate Partner Violence: A Pilot Study Hee-Wook Weon 1, Youn-Eon Byun 2 and Hyun-Ja Lim 3,* 1 Department of Brain & Cognitive Science, Seoul University of Buddhism, Seoul 08559, Korea; [email protected] 2 Department of Youth Science, Kyonggi University, Suwon 16227, Korea; [email protected] 3 Department of Community Health & Epidemiology, University of Saskatchewan, Saskatoon, SK S7N 2Z4, Canada * Correspondence: [email protected] Abstract: Background: The perpetrators of intimate partner violence (IPV) and their victims have different emotional states. Abusers typically have problems associated with low self-esteem, low self-awareness, violence, anger, and communication, whereas victims experience mental distress and physical pain. The emotions surrounding IPV for both abuser and victim are key influences on their behavior and their relationship. Methods: The objective of this pilot study was to examine emotional and psychological interactions between IPV abusers and victims using quantified electroencephalo- gram (QEEG). Two abuser–victim case couples and one non-abusive control couple were recruited from the Mental Image Recovery Program for domestic violence victims in Seoul, South Korea, from Citation: Weon, H.-W.; Byun, Y.-E.; 7–30 June 2017. Data collection and analysis were conducted using BrainMaster and NeuroGuide. Lim, H.-J. Quantitative EEG (QEEG) The emotional pattern characteristics between abuser and victim were examined and compared to Analysis of Emotional Interaction those of the non-abusive couple. Results: Emotional states and reaction patterns were different for between Abusers and Victims in the non-abusive and IPV couples. -
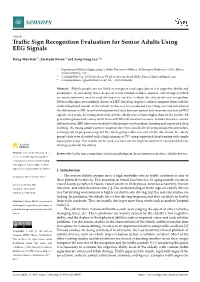
Traffic Sign Recognition Evaluation for Senior Adults Using EEG Signals
sensors Article Traffic Sign Recognition Evaluation for Senior Adults Using EEG Signals Dong-Woo Koh 1, Jin-Kook Kwon 2 and Sang-Goog Lee 1,* 1 Department of Media Engineering, Catholic University of Korea, 43 Jibong-ro, Bucheon-si 14662, Korea; [email protected] 2 CookingMind Cop. 23 Seocho-daero 74-gil, Seocho-gu, Seoul 06621, Korea; [email protected] * Correspondence: [email protected]; Tel.: +82-2-2164-4909 Abstract: Elderly people are not likely to recognize road signs due to low cognitive ability and presbyopia. In our study, three shapes of traffic symbols (circles, squares, and triangles) which are most commonly used in road driving were used to evaluate the elderly drivers’ recognition. When traffic signs are randomly shown in HUD (head-up display), subjects compare them with the symbol displayed outside of the vehicle. In this test, we conducted a Go/Nogo test and determined the differences in ERP (event-related potential) data between correct and incorrect answers of EEG signals. As a result, the wrong answer rate for the elderly was 1.5 times higher than for the youths. All generation groups had a delay of 20–30 ms of P300 with incorrect answers. In order to achieve clearer differentiation, ERP data were modeled with unsupervised machine learning and supervised deep learning. The young group’s correct/incorrect data were classified well using unsupervised machine learning with no pre-processing, but the elderly group’s data were not. On the other hand, the elderly group’s data were classified with a high accuracy of 75% using supervised deep learning with simple signal processing. -

The Evidence-Base for Neurofeedback As a Reimbursable Healthcare Service to Treat Attention Deficit/Hyperactivity Disorder
The Evidence-Base for Neurofeedback as a Reimbursable Healthcare Service to Treat Attention Deficit/Hyperactivity Disorder By H. Edmund Pigott, Ph.D.,a Lindsay De Biase, Ph.D.,b c d Eugenia Bodenhamer-Davis, Ph.D. & Richard E. Davis, M.S. a Ed Pigott, Ph.D. is a licensed psychologist and Director of Neurotherapy Services at Behavioral Health of the Palm Beaches. He is also in private practice at The Center for Brain Training in Jupiter, FL. b Lindsay De Biase, Ph.D. is a neuroscientist and post-doctoral fellow. C Eugenia Bodenhamer-Davis, Ph.D. is an Associate Professor and Director, Neurotherapy Program, University of North Texas and a Board member of the Biofeedback Certification International Alliance. D Richard E. Davis, M.S. is a Licensed Professional Counselor in private practice in Denton, TX, specializing in neurofeedback and Quantitative EEG. He is also a Past President of the International Society of Neurofeedback and Research. Acknowledgements: Preparation of this white paper was guided by extensive discussion and critical review from Henry Harbin with assistance from Thomas Bearden and Robert Thatcher along with the invaluable help from Alexei Berd in securing articles for review. The authors would like to thank the Board of the International Society of Neurofeedback and Research for their support of this project. 1 Table of Contents Executive Summary 3 An Overview of Neurofeedback Practice 6 The Inadequacy of Current ADHD Treatments 8 Neurofeedback: The Operant Conditioning of Trainees’ EEG 12 Neurofeedback: An Evidence-Based -

13Th Valley John M. Del Vecchio Fiction 25.00 ABC of Architecture
13th Valley John M. Del Vecchio Fiction 25.00 ABC of Architecture James F. O’Gorman Non-fiction 38.65 ACROSS THE SEA OF GREGORY BENFORD SF 9.95 SUNS Affluent Society John Kenneth Galbraith 13.99 African Exodus: The Origins Christopher Stringer and Non-fiction 6.49 of Modern Humanity Robin McKie AGAINST INFINITY GREGORY BENFORD SF 25.00 Age of Anxiety: A Baroque W. H. Auden Eclogue Alabanza: New and Selected Martin Espada Poetry 24.95 Poems, 1982-2002 Alexandria Quartet Lawrence Durell ALIEN LIGHT NANCY KRESS SF Alva & Irva: The Twins Who Edward Carey Fiction Saved a City And Quiet Flows the Don Mikhail Sholokhov Fiction AND ETERNITY PIERS ANTHONY SF ANDROMEDA STRAIN MICHAEL CRICHTON SF Annotated Mona Lisa: A Carol Strickland and Non-fiction Crash Course in Art History John Boswell From Prehistoric to Post- Modern ANTHONOLOGY PIERS ANTHONY SF Appointment in Samarra John O’Hara ARSLAN M. J. ENGH SF Art of Living: The Classic Epictetus and Sharon Lebell Non-fiction Manual on Virtue, Happiness, and Effectiveness Art Attack: A Short Cultural Marc Aronson Non-fiction History of the Avant-Garde AT WINTER’S END ROBERT SILVERBERG SF Austerlitz W.G. Sebald Auto biography of Miss Jane Ernest Gaines Fiction Pittman Backlash: The Undeclared Susan Faludi Non-fiction War Against American Women Bad Publicity Jeffrey Frank Bad Land Jonathan Raban Badenheim 1939 Aharon Appelfeld Fiction Ball Four: My Life and Hard Jim Bouton Time Throwing the Knuckleball in the Big Leagues Barefoot to Balanchine: How Mary Kerner Non-fiction to Watch Dance Battle with the Slum Jacob Riis Bear William Faulkner Fiction Beauty Robin McKinley Fiction BEGGARS IN SPAIN NANCY KRESS SF BEHOLD THE MAN MICHAEL MOORCOCK SF Being Dead Jim Crace Bend in the River V. -

Intensive Lifestyle Changes for Reversal of Coronary Heart Disease
Intensive Lifestyle Changes for Reversal of Coronary Heart Disease Dean Ornish, MD; Larry W. Scherwitz, PhD; James H. Billings, PhD, MPH; K. Lance Gould, MD; Terri A. Merritt, MS; Stephen Sparler, MA; William T. Armstrong, MD; Thomas A. Ports, MD; Richard L. Kirkeeide, PhD; Charissa Hogeboom, PhD; Richard J. Brand, PhD Context.—The Lifestyle Heart Trial demonstrated that intensive lifestyle THE LIFESTYLE Heart Trial was the changes may lead to regression of coronary atherosclerosis after 1 year. first randomized clinical trial to investi- Objectives.—To determine the feasibility of patients to sustain intensive lifestyle gate whether ambulatory patients could changes for a total of 5 years and the effects of these lifestyle changes (without be motivated to make and sustain com- lipid-lowering drugs) on coronary heart disease. prehensive lifestyle changes and, if so, whether the progression of coronary Design.—Randomized controlled trial conducted from 1986 to 1992 using a atherosclerosis could be stopped or re- randomized invitational design. versed without using lipid-lowering Patients.—Forty-eight patients with moderate to severe coronary heart disease drugs as measured by computer-as- were randomized to an intensive lifestyle change group or to a usual-care control sisted quantitative coronary arteriogra- group, and 35 completed the 5-year follow-up quantitative coronary arteriography. phy. This study derived from earlier Setting.—Two tertiary care university medical centers. studies that used noninvasive mea- Intervention.—Intensive lifestyle changes (10% fat whole foods vegetarian diet, sures.1,2 aerobic exercise, stress management training, smoking cessation, group psycho- After 1 year, we found that experi- social support) for 5 years. -

The Brain That Changes Itself
The Brain That Changes Itself Stories of Personal Triumph from the Frontiers of Brain Science NORMAN DOIDGE, M.D. For Eugene L. Goldberg, M.D., because you said you might like to read it Contents 1 A Woman Perpetually Falling . Rescued by the Man Who Discovered the Plasticity of Our Senses 2 Building Herself a Better Brain A Woman Labeled "Retarded" Discovers How to Heal Herself 3 Redesigning the Brain A Scientist Changes Brains to Sharpen Perception and Memory, Increase Speed of Thought, and Heal Learning Problems 4 Acquiring Tastes and Loves What Neuroplasticity Teaches Us About Sexual Attraction and Love 5 Midnight Resurrections Stroke Victims Learn to Move and Speak Again 6 Brain Lock Unlocked Using Plasticity to Stop Worries, OPsessions, Compulsions, and Bad Habits 7 Pain The Dark Side of Plasticity 8 Imagination How Thinking Makes It So 9 Turning Our Ghosts into Ancestors Psychoanalysis as a Neuroplastic Therapy 10 Rejuvenation The Discovery of the Neuronal Stem Cell and Lessons for Preserving Our Brains 11 More than the Sum of Her Parts A Woman Shows Us How Radically Plastic the Brain Can Be Appendix 1 The Culturally Modified Brain Appendix 2 Plasticity and the Idea of Progress Note to the Reader All the names of people who have undergone neuroplastic transformations are real, except in the few places indicated, and in the cases of children and their families. The Notes and References section at the end of the book includes comments on both the chapters and the appendices. Preface This book is about the revolutionary discovery that the human brain can change itself, as told through the stories of the scientists, doctors, and patients who have together brought about these astonishing transformations. -

Brain Responses Before and After Intensive Second Language Learning: Proficiency Based Changes and First Language Background Effects in Adult Learners
Brain Responses before and after Intensive Second Language Learning: Proficiency Based Changes and First Language Background Effects in Adult Learners Erin Jacquelyn White1,2*, Fred Genesee1,2, Karsten Steinhauer1,3* 1 Centre for Research on Brain, Language and Music, Montreal, Canada, 2 Department of Psychology, McGill University, Montreal, Canada, 3 School of Communication Sciences and Disorders, McGill University, Montreal, Canada Abstract This longitudinal study tracked the neuro-cognitive changes associated with second language (L2) grammar learning in adults in order to investigate how L2 processing is shaped by a learner’s first language (L1) background and L2 proficiency. Previous studies using event-related potentials (ERPs) have argued that late L2 learners cannot elicit a P600 in response to L2 grammatical structures that do not exist in the L1 or that are different in the L1 and L2. We tested whether the neuro- cognitive processes underlying this component become available after intensive L2 instruction. Korean- and Chinese late- L2-learners of English were tested at the beginning and end of a 9-week intensive English-L2 course. ERPs were recorded while participants read English sentences containing violations of regular past tense (a grammatical structure that operates differently in Korean and does not exist in Chinese). Whereas no P600 effects were present at the start of instruction, by the end of instruction, significant P600s were observed for both L1 groups. Latency differences in the P600 exhibited by Chinese and Korean speakers may be attributed to differences in L1–L2 reading strategies. Across all participants, larger P600 effects at session 2 were associated with: 1) higher levels of behavioural performance on an online grammaticality judgment task; and 2) with correct, rather than incorrect, behavioural responses. -
Vegetarianism’ Is a Case for Returning to Our Essence As Beings Created in the Image and Likeness of God
“This important pamphlet helps us advance the supreme Jewish goals of tikkun olam (healing and improving our world) and kiddush haShem (sanctifying the Divine Name).” —RABBI DAVID ROSEN, FORMER CHIEF RABBI OF IRELAND “The authors have powerfully united scientific and spiritual perspectives on why we—as Jews, as human beings, and as members of the global commons—should ‘go vegetarian.’” —RABBI FRED SCHERLINDER DOBB, COALITION ON THE ENVIRONMENT AND JEWISH LIFE A CASE FOR ‘“A Case for Jewish Vegetarianism’ is a case for returning to our essence as beings created in the image and likeness of God. It is a guide to be ... read and a guideline to be followed.” —RABBI RAMI M. SHAPIRO, SIMPLY JEWISH AND ONE RIVER FOUNDATION EWISH “Judaism … inspires and compels us to think before we eat. ‘A Case for J Jewish Vegetarianism’ provides many powerful reasons for us to be even VEGETARIANISM more compassionate through the foods we choose to consume.” —RABBI JONATHAN K. CRANE, HARVARD HILLEL “The case for Jewish vegetarianism is increasingly compelling, for ethical, environmental and health reasons--this provocative and important booklet makes that case lucidly from all three perspectives.” —RABBI BARRY SCHWARTZ, CENTRAL CONFERENCE OF AMERICAN RABBIS TASK FORCE ON KASHRUT FOR ANIMALS, FOR YOURSELF, AND FOR THE ENVIRONMENT People for the Ethical Treatment of Animals • GoVeg.com VEG314 1/05 RABBINIC STATEMENTS OF SUPPORT INTRODUCTION The Variety of Jewish Arguments for Vegetarianism “In contemporary society, more than ever before, vegetarianism should be an imperative Vegetarianism is becoming more and more popular in North for Jews who seek to live in accordance with Judaism’s most sublime teachings.