Nitrazepam for the Treatment of Epilepsy in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Comparison of Short-And Long-Acting Benzodiazepine-Receptor Agonists
J Pharmacol Sci 107, 277 – 284 (2008)3 Journal of Pharmacological Sciences ©2008 The Japanese Pharmacological Society Full Paper Comparison of Short- and Long-Acting Benzodiazepine-Receptor Agonists With Different Receptor Selectivity on Motor Coordination and Muscle Relaxation Following Thiopental-Induced Anesthesia in Mice Mamoru Tanaka1, Katsuya Suemaru1,2,*, Shinichi Watanabe1, Ranji Cui2, Bingjin Li2, and Hiroaki Araki1,2 1Division of Pharmacy, Ehime University Hospital, Shitsukawa, Toon, Ehime 791-0295, Japan 2Department of Clinical Pharmacology and Pharmacy, Neuroscience, Ehime University Graduate School of Medicine, Shitsukawa, Toon, Ehime 791-0295, Japan Received November 7, 2007; Accepted May 15, 2008 Abstract. In this study, we compared the effects of Type I benzodiazepine receptor–selective agonists (zolpidem, quazepam) and Type I/II non-selective agonists (zopiclone, triazolam, nitrazepam) with either an ultra-short action (zolpidem, zopiclone, triazolam) or long action (quazepam, nitrazepam) on motor coordination (rota-rod test) and muscle relaxation (traction test) following the recovery from thiopental-induced anesthesia (20 mg/kg) in ddY mice. Zolpidem (3 mg/kg), zopiclone (6 mg/kg), and triazolam (0.3 mg/kg) similarly caused an approximately 2-fold prolongation of the thiopental-induced anesthesia. Nitrazepam (1 mg/kg) and quazepam (3 mg/kg) showed a 6- or 10-fold prolongation of the anesthesia, respectively. Zolpidem and zopiclone had no effect on the rota-rod and traction test. Moreover, zolpidem did not affect motor coordination and caused no muscle relaxation following the recovery from the thiopental-induced anesthesia. However, zopiclone significantly impaired the motor coordination at the beginning of the recovery. Triazolam significantly impaired the motor coordination and muscle relaxant activity by itself, and these impairments were markedly exacerbated after the recovery from anesthesia. -

Red with Nitrazepam and Placebo in Acute Emergency Driving Situations and in Monotonous Simulated Driving
109 A 1986 The Carry-over Effects of Triazolam Compa- red with Nitrazepam and Placebo in Acute Emergency Driving Situations and in Mono- tonous Simulated Driving Hans Laurell and Jan Törnroos Reprint from Acta Pharmacologica et toxicologica 1986 v Väg06/7 Efi/( Statens väg- och trafikinstitut (VTI) * 581 01 Linköping [St]tlltet Swedish Road and Traffic Research Institute * S-581 01 Linköping Sweden Acta pharmacol. et toxicol. 1986, 58, 182186. From the National Swedish Road and Traffic Research Institute, (V.T.I.), S-58 101 Linköping, Sweden The Carry-over Effects of Triazolam Compared with Nitrazepam and Placebo in Acute Emergency Driving Situations and in Monotonous Simulated Driving Hans Laurell and Jan Törnros (Received October 9, 1985; Accepted January 9, 1986) Abstract: Eighteen healthy volunteers of both sexes, aged 2034, were tested in the morning while undertaking real car driving avoidance manoeuvres and during monotonous simulated driving after 1 and 3 nights of medication with triazolam 0.25 mg, nitrazepam 5 mg or placebo. The study was a double-blind, randomized, cross-over study, where a minimum of 7 days wash-out separated the 3 treatment periods. Nitrazepam was found to impair performance in the simulated task after 1 but not after 3 nights of medication. Performance in the triazolam condition was not signicantly different from the other conditions on this task on either day. However, after one night of medication triazolam tended to score worse than placebo but better than nitrazepam. In real car driving a tendency was noted for nitrazepam to score worst, whereas the difference between placebo and triazolam was hardly noticeable. -

Calculating Equivalent Doses of Oral Benzodiazepines
Calculating equivalent doses of oral benzodiazepines Background Benzodiazepines are the most commonly used anxiolytics and hypnotics (1). There are major differences in potency between different benzodiazepines and this difference in potency is important when switching from one benzodiazepine to another (2). Benzodiazepines also differ markedly in the speed in which they are metabolised and eliminated. With repeated daily dosing accumulation occurs and high concentrations can build up in the body (mainly in fatty tissues) (2). The degree of sedation that they induce also varies, making it difficult to determine exact equivalents (3). Answer Advice on benzodiazepine conversion NB: Before using Table 1, read the notes below and the Limitations statement at the end of this document. Switching benzodiazepines may be advantageous for a variety of reasons, e.g. to a drug with a different half-life pre-discontinuation (4) or in the event of non-availability of a specific benzodiazepine. With relatively short-acting benzodiazepines such as alprazolam and lorazepam, it is not possible to achieve a smooth decline in blood and tissue concentrations during benzodiazepine withdrawal. These drugs are eliminated fairly rapidly with the result that concentrations fluctuate with peaks and troughs between each dose. It is necessary to take the tablets several times a day and many people experience a "mini-withdrawal", sometimes a craving, between each dose. For people withdrawing from these potent, short-acting drugs it has been advised that they switch to an equivalent dose of a benzodiazepine with a long half life such as diazepam (5). Diazepam is available as 2mg tablets which can be halved to give 1mg doses. -

Intermittent Treatment of Febrile Convulsions with Nitrazepam Michel Vanasse, Pierre Masson, Guy Geoffroy, Albert Larbrisseau and Pierre C
LE JOURNAL CANADIEN DES SCIENCES NEUROLOGIQUES Intermittent Treatment of Febrile Convulsions with Nitrazepam Michel Vanasse, Pierre Masson, Guy Geoffroy, Albert Larbrisseau and Pierre C. David ABSTRACT: Intermittent oral or rectal administration of diazepam for the prophylactic treatment of febriie convulsions has given results comparable to the continuous use of phenobarbital while limiting side effects and risks of toxicity. Since we believe that nitrazepam is a better anticonvulsant than diazepam, we performed a study to evaluate the effectiveness of this medication in the prophylactic treatment of febrile convulsions. Nitrazepam was given only when the children had fever and almost exclusively in children with a high risk of recurrence (less than 12 months of age at first convulsion; atypical convulsion; one or several previous convulsions). Thirty one children with a high risk of recurrence received nitrazepam. The rate of recurrence in this group was 19.3% after a follow-up of 16 months, compared to 45.8% in 24 children who also had a high risk of recurrence but in whom the parents refused the medication or gave it inadequately (p<0.05). Fifty one children with a low risk of recurrence also were evaluated and followed for at least 12 months (mean 15.4 months). Six were treated with nitrazepam, mostly because of parental anxiety, and none had a recurrence; of the 45 untreated children in this group, 6 (13.6%) had another convulsion. These results show the efficiency of nitrazepam in the prophylactic treatment of febrile convulsions. RESUME: L'utilisation intermittente du diazepam par voie orale ou rectale pour le traitement prophylactique des convulsions febriles a donne d'aussi bons resultats que l'utilisation continue du phenobarbital. -

Pharmacology
STATE ESTABLISHMENT «DNIPROPETROVSK MEDICAL ACADEMY OF HEALTH MINISTRY OF UKRAINE» V.I. MAMCHUR, V.I. OPRYSHKO, А.А. NEFEDOV, A.E. LIEVYKH, E.V.KHOMIAK PHARMACOLOGY WORKBOOK FOR PRACTICAL CLASSES FOR FOREIGN STUDENTS STOMATOLOGY DEPARTMENT DNEPROPETROVSK - 2016 2 UDC: 378.180.6:61:615(075.5) Pharmacology. Workbook for practical classes for foreign stomatology students / V.Y. Mamchur, V.I. Opryshko, A.A. Nefedov. - Dnepropetrovsk, 2016. – 186 p. Reviewed by: N.I. Voloshchuk - MD, Professor of Pharmacology "Vinnitsa N.I. Pirogov National Medical University.‖ L.V. Savchenkova – Doctor of Medicine, Professor, Head of the Department of Clinical Pharmacology, State Establishment ―Lugansk state medical university‖ E.A. Podpletnyaya – Doctor of Pharmacy, Professor, Head of the Department of General and Clinical Pharmacy, State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ Approved and recommended for publication by the CMC of State Establishment ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ (protocol №3 from 25.12.2012). The educational tutorial contains materials for practical classes and final module control on Pharmacology. The tutorial was prepared to improve self-learning of Pharmacology and optimization of practical classes. It contains questions for self-study for practical classes and final module control, prescription tasks, pharmacological terms that students must know in a particular topic, medical forms of main drugs, multiple choice questions (tests) for self- control, basic and additional references. This tutorial is also a student workbook that provides the entire scope of student’s work during Pharmacology course according to the credit-modular system. The tutorial was drawn up in accordance with the working program on Pharmacology approved by CMC of SE ―Dnipropetrovsk medical academy of Health Ministry of Ukraine‖ on the basis of the standard program on Pharmacology for stomatology students of III - IV levels of accreditation in the specialties Stomatology – 7.110105, Kiev 2011. -

Drug Interactions and Lethal Drug Combinations
J Clin Pathol: first published as 10.1136/jcp.s3-9.1.94 on 1 January 1975. Downloaded from J. clin. Path., 28, Suppl. (Roy. Coll. Path.), 9, 94-98 The drug dilemma-benefits and hazards Drug interactions and lethal drug combinations ALAN RICHENS From the Department of Clinical Pharmacology, St Bartholomew's Hospital, London Although the development of drugs of greater example, aspirin can displace oral anticoagulants potency and efficacy confers on the physician from their plasma-protein-binding sites, and in- increasing power to treat serious diseases, it also directly acting sympathomimetics contained in cough increases the number and seriousness of potential mixtures can cause a hypertensive crisis in patients adverse effects and drug interactions which can on monoamine oxidase inhibitors. Self-medication is occur. Most hospital patients receive more than one common, and often involves drugs obtained on drug at a time, the average number often being prescription for a previous illness. greater than five (Smith, Seidl, and Cluff, 1966). The 4 When several clinics or doctors are involved in incidence of drug reactions rises with the number of the care of a patient, one doctor may not be aware of drugs prescribed simultaneously. In patients pre- what another has prescribed. scribed one to five drugs the incidence of reactions is 5 When preparations which contain more than 18-6%, while in patients prescribed six or more one ingredient are prescribed by their trade names. it rises to 814 % (Hurwitz and Wade, 1969). There are a number of ways in which drugs may The Boston Collaborative Drug Surveillance interact. -

Nitrazepam 5Mg Tablets
Package leaflet: Information for the patient Nitrazepam 5mg Tablets Read all of this leaflet carefully before you start Make sure that you can sleep without interruptions for 7 to 8 hours after taking this medicine because it contains important taking the tablets. information for you. Because Nitrazepam tablets relax the muscles, elderly patients should • Keep this leaflet. You may need to read it again. take extra care when they get up at night as there is a risk of falls and • If you have any further questions, ask your doctor or consequently of injuries including hip fractures. pharmacist. • This medicine has been prescribed for you only. Do Other considerations • Dependence - when taking this medicine there is a risk of dependence, not pass it on to others. It may harm them, even if their which increases with the dose and duration of treatment and also in signs of illness are the same as yours. patients with a history of alcoholism and drug abuse. • If you get any side effects, talk to your doctor or • Tolerance - if after a few weeks you notice that the tablets are not pharmacist. This includes any possible side effects not working as well as they did when first starting treatment, you should listed in this leaflet. See section 4. speak to your doctor. • Withdrawal - treatment should be gradually withdrawn. Withdrawal What is in this leaflet symptoms occur with nitrazepam even when normal doses are given 1 What Nitrazepam tablets are and what they for short periods of time. See section 3, ‘If you stop taking Nitrazepam are used for tablets’. -

Focus on Benzodiazepines
Graylands Hospital Drug Bulletin Focus on Benzodiazepines North Metropolitan Health Service – Mental Health March 2015 Vol 22 No.1 ISSN 1323–1251 The Non -BZD hypnotics such as zolpidem and Introduction zopiclone (Z-drugs) are more selective for the alpha-1 subclass which seems to drive sleepiness but not anti-anxiety. Benzodiazepines (BZDs) are one of the most commonly prescribed medications for the treatment Table 1: BZDs and relative half-lives9,10 of insomnia and anxiety. 1 They are also frequently used to treat psychiatric emergencies, epilepsy, severe muscle spasm, acute alcohol withdrawal, Drug name Half -life (hours) anaesthesia and intensive care. Short -acting Triazolam 2 However, the use of BZDs is often controversial as Alprazolam 6-12 they are widely acknowledged to be addictive and Oxazepam 4-15 withdrawal symptoms can occur after 4-6 weeks of Temazepam 8-22 continuous use. This had led to the recommendation Medium -acting that they should not be used as hypnotics or Bromazepam 10 -20 anxiolytics for longer than 4 weeks. 2 In older age, Lorazepam 10 -20 BZDs also have serious adverse effects, including increased risk of falls, road traffic accidents and Long -acting 3,4 Clobazam 12 -60 cognitive impairment. Clonazepam 18 -50 More recently the risks of long term BZD use have Diazepam 20 -100 received greater focus with new evidence Flunitrazepam 18 -26 demonstrating a link between BZD use and the Nitrazepam 15 -38 5 development of Alzheimer’s disease and also 6 increased risk of mortality. Benzodiazepine use in Psychiatry Given the wide spread usage of these medications and the associated risk, this bulletin reviews BZDs Sleep disorders with particular emphasis upon adverse effects, dependence and abuse potential. -

Benzodiazepines and Dementia
Dementia Q&A 25 Benzodiazepines and dementia Benzodiazepines are a class of drugs commonly used to treat anxiety and insomnia. However, long-term regular treatment with benzodiazepines carries a number of risks. This sheet provides information about how these drugs work as well as the impact that they may have in respect to dementia risk and cognitive functioning. What are benzodiazepines? Benzodiazepines are psychotropic medications (that is, medications that impact on mood and behaviour) that have been in use since the 1960s primarily for the treatment of anxiety, panic disorders and insomnia. They are a ‘depressant’ medication, also known as ‘minor tranquilizers’ and can also be used for treatment of seizures, muscle spasms, alcohol withdrawal and as a preoperative medication for medical or dental procedures. Benzodiazepines are widely available in Australia (Table 1) and are used regularly by around 15% of Australian adults aged 65 years and over.1 Although prescribing rates have fallen over the past decade, there is a continued high rate of prescription among the population.2,3 1 Windle A, Elliot E, Duszynski K, Moore V. Benzodiazepine prescribing in elderly Australian general practice patients. Australian & New Zealand Journal of Public Health. 2007;31(4):379–381. 2 Stephenson CP, Karanges,E, McGreggor IS. Trends in the utilisation of psychotropic medications in Australia from 2000 to 2011. Australian & New Zealand Journal of Psychiatry. 2013;47(1):74–87. 3 Islam MM, Conigrave KM, Day CA, Nguyen Y, Haber PS. Twenty-year trends in benzodiazepine dispensing in the Australian population. Internal Medicine Journal. 2014;44(1):57–64. -
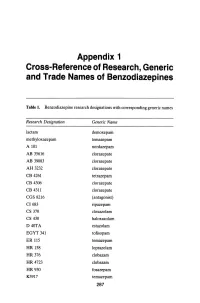
Appendix 1 Cross-Reference of Research, Generic and Trade Names of Benzodiazepines
Appendix 1 Cross-Reference of Research, Generic and Trade Names of Benzodiazepines Table 1. Benzodiazepine research designations with corresponding generic names Research Designation Generic Name lactam demoxepam methyloxazepam temazepam A 101 nordazepam AB 35616 clorazepate AB 39083 clorazepate AH 3232 clorazepate CB 4261 tetrazepam CB 4306 clorazepate CB 4311 clorazepate CGS 8216 (antagonist) CI683 ripazepam CS 370 cloxazolam CS 430 haloxazolam D40TA estazolam EGYT 341 tofisopam ER 115 temazepam HR 158 loprazolam HR376 clobazam HR 4723 clobazam HR930 fosazepam K3917 temazepam 287 THE BENZODIAZEPINES Research Designation Generic Name LA 111 diazepam LM 2717 clobazam ORF 8063 triflubazam Ro 4-5360 nitrazepam Ro 5-0690 chlordiazepoxide Ro 5-0883 desmethy1chlordiazepoxide Ro 5-2092 demoxepam Ro 5-2180 desmethyldiazepam Ro 5-2807 diazepam Ro 5-2925 desmethylmedazepam Ro 5-3059 nitrazepam Ro 5-3350 bromazepam Ro 5-3438 fludiazepam Ro 5-4023 clonazepam Ro 5-4200 flunitrazepam Ro 5-4556 medazepam Ro 5-5345 temazepam Ro 5-6789 oxazepam Ro 5-6901 flurazepam Ro 15-1788 (antagonist) Ro 21-3981 midazolam RU 31158 loprazolam S 1530 nimetazepam SAH 1123 isoquinazepam SAH 47603 temazepam SB 5833 camazepam SCH 12041 halazepam SCH 16134 quazepam U 28774 ketazolam U 31889 alprazolam U 33030 triazolam W4020 prazepam We 352 triflubazam 288 RESEARCH, GENERIC AND TRADE NAMES Research Designation Generic Name We 941 brotizolam Wy 2917 temazepam Wy 3467 diazepam Wy 3498 oxazepam Wy 3917 temazepam Wy 4036 lorazepam Wy 4082 lormetazepam Wy 4426 oxazepam Y 6047 -
Identification and Quantification of 22 Benzodiazepines in Postmortem Fluids and Tissues Using UPLC/MS/MS
DOT/FAA/AM-18/1 Office of Aerospace Medicine Washington, DC 20591 Identification and Quantification of 22 Benzodiazepines in Postmortem Fluids and Tissues using UPLC/MS/MS Michael K. Angier Sunday R. Saenz Roxane M. Ritter Russell J. Lewis May 2018 Final Report NOTICE This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The United States Government assumes no liability for the contents thereof. ___________ This publication and all Office of Aerospace Medicine technical reports are available in full-text from the Civil Aerospace Medical Institute’s publications website: http://www.faa.gov/go/oamtechreports Technical Report Documentation Page 1. Report No. 2. Government Accession No. 3. Recipient's Catalog No. DOT/FAA/AM-18/1 4. Title and Subtitle 5. Report Date Identification and Quantification of 22 Benzodiazepines in Postmortem May 2018 Fluids and Tissues using UPLC/MS/MS 6. Performing Organization Code 7. Author(s) 8. Performing Organization Report No. Angier MK, Saenz SR, Ritter RM, and Lewis RJ 9. Performing Organization Name and Address 10. Work Unit No. (TRAIS) FAA Civil Aerospace Medical Institute P.O. Box 25082 11. Contract or Grant No. Oklahoma City, OK 73125 12. Sponsoring Agency name and Address 13. Type of Report and Period Covered Office of Aerospace Medicine Federal Aviation Administration 800 Independence Ave., S.W. Washington, DC 20591 14. Sponsoring Agency Code 15. Supplemental Notes 16. Abstract Benzodiazepines, a class of drugs known to cause central nervous system depression, are widely prescribed for a variety of different medical conditions such as anxiety, insomnia, and as a preoperative sedative in conjunction with anesthesia. -

An Update on Sleep Disorders and Their Treatment
CMHP Review Sleep_Layout 1 26/09/2013 11:19 Page 1 Sleep disorders z Review An update on sleep disorders and their treatment Michele Sie GPhC, MCMHP In the third of this series of updated reviews on the major psychiatric drug groups, produced in association with the College of Mental Health Pharmacy (CMHP; www.cmhp.org.uk), Michele Sie describes the main types of sleep disorder and their features, and provides an overview of their treatment. leep is a fundamental necessity that is required by • Have a good bedtime routine, go to bed and get up all of us. Sleep requirements vary with age and S at the same time every day and avoid daytime naps between individuals but in general the average • Avoid stimulants such as caffeine, nicotine, chocolate requirement for a healthy adult is between seven and and alcohol six hours before bedtime 1 eight hours of sleep per night. • Take regular exercise during the day, but avoid Sleep is divided into two types. Rapid eye move- strenuous exercise within four hours of bedtime ment (REM) sleep and non-rapid eye movement • Avoid large meals close to bedtime (non-REM) sleep. REM sleep, as the name suggests, • Associate your bed with sleep. Do not watch TV or is characterised by rapid movements of the eyes, while listen to music when retiring to bed in non-REM sleep there is little or no movement of • The bedroom should be a quiet, relaxing place to the eyes and any eye movement is slow.2 sleep; make sure the room is not too hot or too cold • If after 30 minutes you cannot get off to sleep then get up.