Gynecologic Anatomy and Physiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sexual Reproduction & the Reproductive System Visual
Biology 202: Sexual Reproduction & the Reproductive System 1) Label the diagram below. Some terms may be used more than once. Spermatozoa (N) Mitosis Spermatogonium (2N) Spermatids (N) Primary Oocyte (2N) Polar bodies (N) Ootid (N) Second polar body (N) Meiosis I Primary spermatocyte (2N) Oogonium (2N) Secondary oocyte (2N) Ovum (N) Secondary spermatocytes (2N) First polar body Meiosis II Source Lesson: Gametogenesis & Meiosis: Process & Differences 2) Label the diagram of the male reproductive system below. Seminal vesicle Testis Scrotum Pubic bone Penis Prostate gland Urethra Epididymis Vas deferens Bladder Source Lesson: Male Reproductive System: Structures, Functions & Regulation 3) Label the image below. Rectum Testis Ureter Bulbourethral gland Urethra Urinary bladder Pubic bone Penis Seminal vesicle Ductus deferens Epididymis Prostate gland Anus Source Lesson: Semen: Composition & Production 4) Label the structures below. Inner and outer lips of the vagina Mons pubis Vaginal opening Clitoris Anus Urethral opening Perineum Vulva Source Lesson: Female Reproductive System: Structures & Functions 5) Label the diagram below. Some terms may be used more than once. Clitoris Vulva Labia majora Labia minora Perineum Clitoral hood Vaginal opening Source Lesson: Female Reproductive System: Structures & Functions 6) Label the internal organs that make up the female reproductive system. Uterus Fallopian tubes Ovaries Cervix Vagina Endometrium Source Lesson: Female Reproductive System: Structures & Functions 7) Label the diagram below. LH Follicular -

Chapter 28 *Lecture Powepoint
Chapter 28 *Lecture PowePoint The Female Reproductive System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • The female reproductive system is more complex than the male system because it serves more purposes – Produces and delivers gametes – Provides nutrition and safe harbor for fetal development – Gives birth – Nourishes infant • Female system is more cyclic, and the hormones are secreted in a more complex sequence than the relatively steady secretion in the male 28-2 Sexual Differentiation • The two sexes indistinguishable for first 8 to 10 weeks of development • Female reproductive tract develops from the paramesonephric ducts – Not because of the positive action of any hormone – Because of the absence of testosterone and müllerian-inhibiting factor (MIF) 28-3 Reproductive Anatomy • Expected Learning Outcomes – Describe the structure of the ovary – Trace the female reproductive tract and describe the gross anatomy and histology of each organ – Identify the ligaments that support the female reproductive organs – Describe the blood supply to the female reproductive tract – Identify the external genitalia of the female – Describe the structure of the nonlactating breast 28-4 Sexual Differentiation • Without testosterone: – Causes mesonephric ducts to degenerate – Genital tubercle becomes the glans clitoris – Urogenital folds become the labia minora – Labioscrotal folds -

The Cyclist's Vulva
The Cyclist’s Vulva Dr. Chimsom T. Oleka, MD FACOG Board Certified OBGYN Fellowship Trained Pediatric and Adolescent Gynecologist National Medical Network –USOPC Houston, TX DEPARTMENT NAME DISCLOSURES None [email protected] DEPARTMENT NAME PRONOUNS The use of “female” and “woman” in this talk, as well as in the highlighted studies refer to cis gender females with vulvas DEPARTMENT NAME GOALS To highlight an issue To discuss why this issue matters To inspire future research and exploration To normalize the conversation DEPARTMENT NAME The consensus is that when you first start cycling on your good‐as‐new, unbruised foof, it is going to hurt. After a “breaking‐in” period, the pain‐to‐numbness ratio becomes favourable. As long as you protect against infection, wear padded shorts with a generous layer of chamois cream, no underwear and make regular offerings to the ingrown hair goddess, things are manageable. This is wrong. Hannah Dines British T2 trike rider who competed at the 2016 Summer Paralympics DEPARTMENT NAME MY INTRODUCTION TO CYCLING Childhood Adolescence Adult Life DEPARTMENT NAME THE CYCLIST’S VULVA The Issue Vulva Anatomy Vulva Trauma Prevention DEPARTMENT NAME CYCLING HAS POSITIVE BENEFITS Popular Means of Exercise Has gained popularity among Ideal nonimpact women in the past aerobic exercise decade Increases Lowers all cause cardiorespiratory mortality risks fitness DEPARTMENT NAME Hermans TJN, Wijn RPWF, Winkens B, et al. Urogenital and Sexual complaints in female club cyclists‐a cross‐sectional study. J Sex Med 2016 CYCLING ALSO PREDISPOSES TO VULVAR TRAUMA • Significant decreases in pudendal nerve sensory function in women cyclists • Similar to men, women cyclists suffer from compression injuries that compromise normal function of the main neurovascular bundle of the vulva • Buller et al. -

Female Perineum Doctors Notes Notes/Extra Explanation Please View Our Editing File Before Studying This Lecture to Check for Any Changes
Color Code Important Female Perineum Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, the student should be able to describe the: ✓ Boundaries of the perineum. ✓ Division of perineum into two triangles. ✓ Boundaries & Contents of anal & urogenital triangles. ✓ Lower part of Anal canal. ✓ Boundaries & contents of Ischiorectal fossa. ✓ Innervation, Blood supply and lymphatic drainage of perineum. Lecture Outline ‰ Introduction: • The trunk is divided into 4 main cavities: thoracic, abdominal, pelvic, and perineal. (see image 1) • The pelvis has an inlet and an outlet. (see image 2) The lowest part of the pelvic outlet is the perineum. • The perineum is separated from the pelvic cavity superiorly by the pelvic floor. • The pelvic floor or pelvic diaphragm is composed of muscle fibers of the levator ani, the coccygeus muscle, and associated connective tissue. (see image 3) We will talk about them more in the next lecture. Image (1) Image (2) Image (3) Note: this image is seen from ABOVE Perineum (In this lecture the boundaries and relations are important) o Perineum is the region of the body below the pelvic diaphragm (The outlet of the pelvis) o It is a diamond shaped area between the thighs. Boundaries: (these are the external or surface boundaries) Anteriorly Laterally Posteriorly Medial surfaces of Intergluteal folds Mons pubis the thighs or cleft Contents: 1. Lower ends of urethra, vagina & anal canal 2. External genitalia 3. Perineal body & Anococcygeal body Extra (we will now talk about these in the next slides) Perineum Extra explanation: The perineal body is an irregular Perineal body fibromuscular mass. -

Microlymphatic Surgery for the Treatment of Iatrogenic Lymphedema
Microlymphatic Surgery for the Treatment of Iatrogenic Lymphedema Corinne Becker, MDa, Julie V. Vasile, MDb,*, Joshua L. Levine, MDb, Bernardo N. Batista, MDa, Rebecca M. Studinger, MDb, Constance M. Chen, MDb, Marc Riquet, MDc KEYWORDS Lymphedema Treatment Autologous lymph node transplantation (ALNT) Microsurgical vascularized lymph node transfer Iatrogenic Secondary Brachial plexus neuropathy Infection KEY POINTS Autologous lymph node transplant or microsurgical vascularized lymph node transfer (ALNT) is a surgical treatment option for lymphedema, which brings vascularized, VEGF-C producing tissue into the previously operated field to promote lymphangiogenesis and bridge the distal obstructed lymphatic system with the proximal lymphatic system. Additionally, lymph nodes with important immunologic function are brought into the fibrotic and damaged tissue. ALNT can cure lymphedema, reduce the risk of infection and cellulitis, and improve brachial plexus neuropathies. ALNT can also be combined with breast reconstruction flaps to be an elegant treatment for a breast cancer patient. OVERVIEW: NATURE OF THE PROBLEM Clinically, patients develop firm subcutaneous tissue, progressing to overgrowth and fibrosis. Lymphedema is a result of disruption to the Lymphedema is a common chronic and progres- lymphatic transport system, leading to accumula- sive condition that can occur after cancer treat- tion of protein-rich lymph fluid in the interstitial ment. The reported incidence of lymphedema space. The accumulation of edematous fluid mani- varies because of varying methods of assess- fests as soft and pitting edema seen in early ment,1–3 the long follow-up required for diagnosing lymphedema. Progression to nonpitting and irre- lymphedema, and the lack of patient education versible enlargement of the extremity is thought regarding lymphedema.4 In one 20-year follow-up to be the result of 2 mechanisms: of patients with breast cancer treated with mastec- 1. -

MR Imaging of Vaginal Morphology, Paravaginal Attachments and Ligaments
MR imaging of vaginal morph:ingynious 05/06/15 10:09 Pagina 53 Original article MR imaging of vaginal morphology, paravaginal attachments and ligaments. Normal features VITTORIO PILONI Iniziativa Medica, Diagnostic Imaging Centre, Monselice (Padova), Italy Abstract: Aim: To define the MR appearance of the intact vaginal and paravaginal anatomy. Method: the pelvic MR examinations achieved with external coil of 25 nulliparous women (group A), mean age 31.3 range 28-35 years without pelvic floor dysfunctions, were compared with those of 8 women who had cesarean delivery (group B), mean age 34.1 range 31-40 years, for evidence of (a) vaginal morphology, length and axis inclination; (b) perineal body’s position with respect to the hymen plane; and (c) visibility of paravaginal attachments and lig- aments. Results: in both groups, axial MR images showed that the upper vagina had an horizontal, linear shape in over 91%; the middle vagi- na an H-shape or W-shape in 74% and 26%, respectively; and the lower vagina a U-shape in 82% of cases. Vaginal length, axis inclination and distance of perineal body to the hymen were not significantly different between the two groups (mean ± SD 77.3 ± 3.2 mm vs 74.3 ± 5.2 mm; 70.1 ± 4.8 degrees vs 74.04 ± 1.6 degrees; and +3.2 ± 2.4 mm vs + 2.4 ± 1.8 mm, in group A and B, respectively, P > 0.05). Overall, the lower third vaginal morphology was the less easily identifiable structure (visibility score, 2); the uterosacral ligaments and the parau- rethral ligaments were the most frequently depicted attachments (visibility score, 3 and 4, respectively); the distance of the perineal body to the hymen was the most consistent reference landmark (mean +3 mm, range -2 to + 5 mm, visibility score 4). -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -
Understanding Cancer of the Vulva
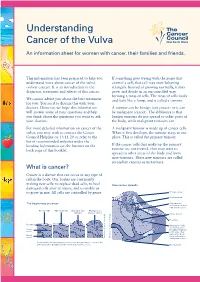
Understanding Cancer of the Vulva An information sheet for women with cancer, their families and friends. This information has been prepared to help you If something goes wrong with the genes that understand more about cancer of the vulva control a cell, that cell may start behaving (vulvar cancer). It is an introduction to the strangely. Instead of growing normally, it may diagnosis, treatment and effects of this cancer. grow and divide in an uncontrolled way, forming a mass of cells. The mass of cells looks We cannot advise you about the best treatment and feels like a lump, and is called a tumour. for you. You need to discuss this with your doctors. However, we hope this information A tumour can be benign (not cancer) or it can will answer some of your questions and help be malignant (cancer). The difference is that you think about the questions you want to ask benign tumours do not spread to other parts of your doctors. the body, while malignant tumours can. For more detailed information on cancer of the A malignant tumour is made up of cancer cells. vulva, you may wish to contact the Cancer When it first develops, the tumour stays in one Council Helpline on 13 11 20 or refer to the place. This is called the primary tumour. list of recommended websites under the heading Information on the Internet on the If the cancer cells that make up the primary back page of this booklet. tumour are not treated, they may start to spread to other areas of the body and form new tumours. -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -

Benign Vulvar Lesions
PEER REVIEWED FEATURE 2 CPD POINTS A GP’s guide to benign vulvar lesions IAN JONES ChM, PhD, FRANZCOG, FRCOG Vulvar lesions may cause pain but are often asymptomatic. Identifying the type of lesion and the appropriate treatment course is an important role of the GP. arious lesions of the vulva are seen by GPs during routine Epithelial lesions examinations and when assessing women with symp- Epithelial lesions include benign cysts and squamous non- tomatic vulvar lumps. Although many lesions are neoplastic proliferations. asymptomatic and do not require treatment, some lesions Vcan cause symptoms when sitting or during coitus. Also, women Benign cysts may be concerned that the lesions are cancerous, which leads them Mucinous cysts to present to their GPs for assessment and reassurance. Mucinous cysts usually occur in adults (Figure 1). They can present Benign vulvar lesions can be classified several ways: anywhere on the vulva but are most commonly found in the • as common or uncommon (Box) vestibule, which extends from the clitoris to the fourchette and • of epithelial or connective tissue origin (Table) laterally from the hymenal ring to the labia minora. The major • by their appearance – many are similar in appearance to and minor vestibular glands are located on the lateral part of the skin lesions in other parts of the body and their manage- vestibule. ment is identical. The bilateral major vestibular glands, better known as Bartholin’s glands, are situated at about the four and eight o’clock positions on the vulva and vary in size from 1 to 10 cm. These glands contain a clear and sometimes mucoid material and mucinous cysts are caused by a blockage in a gland’s duct. -

Female Reproductive System Chapter 28
The Female Reproductive System Chapter 28 • Female Reproductive System Anatomy • Oogenesis and the Sexual Cycle – Ovarian Cycle – Menstrual Cycle Female Reproductive System Functions: • Produce female sex hormones and gametes • Provide nutrition for fetal development • Nourish the infant after birth The Uterus • Thick-walled, pear-shaped, muscular chamber opening into vagina. • Cervix is the rounded opening of the uterus. • Two uterine tubes (also called Fallopian tubes or oviducts) branch off the uterus and terminate near the ovaries. Uterine Tubes • Also called Fallopian Tubes or Oviducts • Open-ended, muscular tube lined with secretory cells and ciliated cells that sweep secretions and peritoneal fluid towards the uterus. • Uterine Tube Regions: – narrow isthmus near the uterus – middle portion is the ampulla – flared distally into infundibulum with fimbriae • Fertilization usually occurs in ampulla or isthmus Epithelium lining the uterine tube consists of ciliated cells, goblet cells and other secretory cells. Cilia move peritoneal fluid and uterine tube secretions towards the uterus. Cervix and Vagina normally have a stratified squamous epithelium Test developed by Dr. G.N. Papanicolaou can detect cervical cancer by identifying transformed squamous cells. normal PAP smear abnormal PAP smear Histology of the Uterus • Perimetrium is the external serosa layer • Myometrium is the middle muscular layer – 1 cm thick in nonpregnant uterus – composed of smooth muscle – produces labor contractions to expel fetus during childbirth • Endometrium – simple columnar epithelium with tubular glands – stratum functionalis is superficial layer that is shed with each menstrual cycle – stratum basalis is deeper layer that regenerates a new stratum functionalis with each menstrual cycle Ovary • Ovaries produce oocytes and female hormones. -

Clinical Pelvic Anatomy
SECTION ONE • Fundamentals 1 Clinical pelvic anatomy Introduction 1 Anatomical points for obstetric analgesia 3 Obstetric anatomy 1 Gynaecological anatomy 5 The pelvic organs during pregnancy 1 Anatomy of the lower urinary tract 13 the necks of the femora tends to compress the pelvis Introduction from the sides, reducing the transverse diameters of this part of the pelvis (Fig. 1.1). At an intermediate level, opposite A thorough understanding of pelvic anatomy is essential for the third segment of the sacrum, the canal retains a circular clinical practice. Not only does it facilitate an understanding cross-section. With this picture in mind, the ‘average’ of the process of labour, it also allows an appreciation of diameters of the pelvis at brim, cavity, and outlet levels can the mechanisms of sexual function and reproduction, and be readily understood (Table 1.1). establishes a background to the understanding of gynae- The distortions from a circular cross-section, however, cological pathology. Congenital abnormalities are discussed are very modest. If, in circumstances of malnutrition or in Chapter 3. metabolic bone disease, the consolidation of bone is impaired, more gross distortion of the pelvic shape is liable to occur, and labour is likely to involve mechanical difficulty. Obstetric anatomy This is termed cephalopelvic disproportion. The changing cross-sectional shape of the true pelvis at different levels The bony pelvis – transverse oval at the brim and anteroposterior oval at the outlet – usually determines a fundamental feature of The girdle of bones formed by the sacrum and the two labour, i.e. that the ovoid fetal head enters the brim with its innominate bones has several important functions (Fig.