Heart Sound Segmentation Algorithm Based on Instantaneous Energy of Electrocardiogram
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 20 *Lecture Powerpoint the Circulatory System: Blood Vessels and Circulation
Chapter 20 *Lecture PowerPoint The Circulatory System: Blood Vessels and Circulation *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • The route taken by the blood after it leaves the heart was a point of much confusion for many centuries – Chinese emperor Huang Ti (2697–2597 BC) believed that blood flowed in a complete circuit around the body and back to the heart – Roman physician Galen (129–c. 199) thought blood flowed back and forth like air; the liver created blood out of nutrients and organs consumed it – English physician William Harvey (1578–1657) did experimentation on circulation in snakes; birth of experimental physiology – After microscope was invented, blood and capillaries were discovered by van Leeuwenhoek and Malpighi 20-2 General Anatomy of the Blood Vessels • Expected Learning Outcomes – Describe the structure of a blood vessel. – Describe the different types of arteries, capillaries, and veins. – Trace the general route usually taken by the blood from the heart and back again. – Describe some variations on this route. 20-3 General Anatomy of the Blood Vessels Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Capillaries Artery: Tunica interna Tunica media Tunica externa Nerve Vein Figure 20.1a (a) 1 mm © The McGraw-Hill Companies, Inc./Dennis Strete, photographer • Arteries carry blood away from heart • Veins -

Physiology Lessons for Use with the Biopac Student Lab Lesson 5
Physiology Lessons Lesson 5 for use with the ELECTROCARDIOGRAPHY I Biopac Student Lab Components of the ECG Richard Pflanzer, Ph.D. Associate Professor Emeritus Indiana University School of Medicine Purdue University School of Science William McMullen Vice President BIOPAC Systems, Inc. BIOPAC® Systems, Inc. 42 Aero Camino, Goleta, CA 93117 (805) 685-0066, Fax (805) 685-0067 Email: [email protected] Web: www.biopac.com Manual Revision PL3.7.5 03162009 BIOPAC Systems, Inc. Page 2 Biopac Student Lab 3.7.5 I. INTRODUCTION The main function of the heart is to pump blood through two circuits: 1. Pulmonary circuit: through the lungs to oxygenate the blood and remove carbon dioxide; and 2. Systemic circuit: to deliver oxygen and nutrients to tissues and remove carbon dioxide. Because the heart moves blood through two separate circuits, it is sometimes described as a dual pump. In order to beat, the heart needs three types of cells: 1. Rhythm generators, which produce an electrical signal (SA node or normal pacemaker); 2. Conductors to spread the pacemaker signal; and 3. Contractile cells (myocardium) to mechanically pump blood. The Electrical and Mechanical Sequence of a Heartbeat The heart has specialized pacemaker cells that start the electrical sequence of depolarization and repolarization. This property of cardiac tissue is called inherent rhythmicity or automaticity. The electrical signal is generated by the sinoatrial node (SA node) and spreads to the ventricular muscle via particular conducting pathways: internodal pathways and atrial fibers, the atrioventricular node (AV node), the bundle of His, the right and left bundle branches, and Purkinje fibers (Fig 5.1). -

Blood Vessels: Part A
Chapter 19 The Cardiovascular System: Blood Vessels: Part A Blood Vessels • Delivery system of dynamic structures that begins and ends at heart – Arteries: carry blood away from heart; oxygenated except for pulmonary circulation and umbilical vessels of fetus – Capillaries: contact tissue cells; directly serve cellular needs – Veins: carry blood toward heart Structure of Blood Vessel Walls • Lumen – Central blood-containing space • Three wall layers in arteries and veins – Tunica intima, tunica media, and tunica externa • Capillaries – Endothelium with sparse basal lamina Tunics • Tunica intima – Endothelium lines lumen of all vessels • Continuous with endocardium • Slick surface reduces friction – Subendothelial layer in vessels larger than 1 mm; connective tissue basement membrane Tunics • Tunica media – Smooth muscle and sheets of elastin – Sympathetic vasomotor nerve fibers control vasoconstriction and vasodilation of vessels • Influence blood flow and blood pressure Tunics • Tunica externa (tunica adventitia) – Collagen fibers protect and reinforce; anchor to surrounding structures – Contains nerve fibers, lymphatic vessels – Vasa vasorum of larger vessels nourishes external layer Blood Vessels • Vessels vary in length, diameter, wall thickness, tissue makeup • See figure 19.2 for interaction with lymphatic vessels Arterial System: Elastic Arteries • Large thick-walled arteries with elastin in all three tunics • Aorta and its major branches • Large lumen offers low resistance • Inactive in vasoconstriction • Act as pressure reservoirs—expand -

Electrical Activity of the Heart: Action Potential, Automaticity, and Conduction 1 & 2 Clive M
Electrical Activity of the Heart: Action Potential, Automaticity, and Conduction 1 & 2 Clive M. Baumgarten, Ph.D. OBJECTIVES: 1. Describe the basic characteristics of cardiac electrical activity and the spread of the action potential through the heart 2. Compare the characteristics of action potentials in different parts of the heart 3. Describe how serum K modulates resting potential 4. Describe the ionic basis for the cardiac action potential and changes in ion currents during each phase of the action potential 5. Identify differences in electrical activity across the tissues of the heart 6. Describe the basis for normal automaticity 7. Describe the basis for excitability 8. Describe the basis for conduction of the cardiac action potential 9. Describe how the responsiveness relationship and the Na+ channel cycle modulate cardiac electrical activity I. BASIC ELECTROPHYSIOLOGIC CHARACTERISTICS OF CARDIAC MUSCLE A. Electrical activity is myogenic, i.e., it originates in the heart. The heart is an electrical syncitium (i.e., behaves as if one cell). The action potential spreads from cell-to-cell initiating contraction. Cardiac electrical activity is modulated by the autonomic nervous system. B. Cardiac cells are electrically coupled by low resistance conducting pathways gap junctions located at the intercalated disc, at the ends of cells, and at nexus, points of side-to-side contact. The low resistance pathways (wide channels) are formed by connexins. Connexins permit the flow of current and the spread of the action potential from cell-to-cell. C. Action potentials are much longer in duration in cardiac muscle (up to 400 msec) than in nerve or skeletal muscle (~5 msec). -

Cardiology Self Learning Package
Cardiology Self Learning Package Module 1: Anatomy and Physiology of the Module 1: Anatomy and Physiology of the Heart Heart. Page 1 Developed by Tony Curran (Clinical Nurse Educator) and Gill Sheppard (Clinical Nurse Specialist) Cardiology (October 2011) CONTENT Introduction…………………………………………………………………………………Page 3 How to use the ECG Self Learning package………………………………………….Page 4 Overview of the Heart…………………………………………………...…………..…….Page 5 Location, Size and Shape of the Heart…………………………………………………Page 5 The Chambers of the Heart…………….………………………………………..……….Page 7 The Circulation System……………………………………….………………..…………Page 8 The Heart Valve Anatomy………………………….…………………………..…………Page 9 Coronary Arteries…………………………………………….……………………..……Page 10 Coronary Veins…………………………………………………………………..……….Page 11 Cardiac Muscle Tissue……………………………………………………………..……Page 12 The Conduction System………………………………………………………………...Page 13 Cardiac Cycle……………………………………………………………………………..Page 15 References…………………………………………………………………………………Page 18 Module Questions………………………………………………………………………..Page 19 Module Evaluation Form………………………………………………………………..Page 22 [Module 1: Anatomy and Physiology of the Heart Page 2 Developed by Tony Curran (Clinical Nurse Educator) and Gill Sheppard (Clinical Nurse Specialist) Cardiology (October 2011) INTRODUCTION Welcome to Module 1: Anatomy and Physiology of the Heart. This self leaning package is designed to as tool to assist nurse in understanding the hearts structure and how the heart works. The goal of this module is to review: Location , size and shape of the heart The chambers of the heart The circulation system of the heart The heart’s valve anatomy Coronary arteries and veins Cardiac muscle tissue The conduction system The cardiac cycle This module will form the foundation of your cardiac knowledge and enable you to understand workings of the heart that will assist you in completing other modules. Learning outcomes form this module are: To state the position of the heart, the size and shape. -

Time-Varying Elastance and Left Ventricular Aortic Coupling Keith R
Walley Critical Care (2016) 20:270 DOI 10.1186/s13054-016-1439-6 REVIEW Open Access Left ventricular function: time-varying elastance and left ventricular aortic coupling Keith R. Walley Abstract heart must have special characteristics that allow it to respond appropriately and deliver necessary blood flow Many aspects of left ventricular function are explained and oxygen, even though flow is regulated from outside by considering ventricular pressure–volume characteristics. the heart. Contractility is best measured by the slope, Emax, of the To understand these special cardiac characteristics we end-systolic pressure–volume relationship. Ventricular start with ventricular function curves and show how systole is usefully characterized by a time-varying these curves are generated by underlying ventricular elastance (ΔP/ΔV). An extended area, the pressure– pressure–volume characteristics. Understanding ventricu- volume area, subtended by the ventricular pressure– lar function from a pressure–volume perspective leads to volume loop (useful mechanical work) and the ESPVR consideration of concepts such as time-varying ventricular (energy expended without mechanical work), is linearly elastance and the connection between the work of the related to myocardial oxygen consumption per beat. heart during a cardiac cycle and myocardial oxygen con- For energetically efficient systolic ejection ventricular sumption. Connection of the heart to the arterial circula- elastance should be, and is, matched to aortic elastance. tion is then considered. Diastole and the connection of Without matching, the fraction of energy expended the heart to the venous circulation is considered in an ab- without mechanical work increases and energy is lost breviated form as these relationships, which define how during ejection across the aortic valve. -

CARDIAC CYCLE & CONTROL (All Cd References Refer to Interactiv
Biology 251 Fall 2015 TOPIC 15: CARDIOVASCULAR SYSTEM: CARDIAC CYCLE & CONTROL (All cd references refer to Interactive Physiology cd, Cardiovascular menu) I. Mechanical Events in the Cardiac Cycle (Figs 13.18 to 13.21; cd cardiac cycle 5 to 17) A. Introduction 1. Systole: Contraction and emptying of the chambers 2. Diastole: Relaxation and filling of the chambers 3. Atria and Ventricles go through separate cycles of systole and diastole 4. The contraction status (being in systole or diastole) determines heart chamber pressure which determines whether valves are open or closed. B. TP interval: Ventricular diastole 1. Atria and ventricles are in diastole (i.e., relaxed). 2. Blood flows from veins into atria 3. Ventricuclar Pressure < Aortic Pressure = Aortic Valve closed 4. Atrial pressure > Ventricular Pressure = AV valve open so 5. Blood flows from atria directly into ventricles. C. P wave and PQ interval: Late ventricular diastole 1. Ventricuclar Pressure < Aortic Pressure = aortic valve closed 2. SA node reaches threshold and fires. 3. Atrial depolarization occurs. 4. Atria contract = atrial systole 5. Atrial Pressure > Ventricular Pressure = AV valves open. 6. Blood squeezed by atrial contraction from atria into ventricles. D. QR Interval: End of ventricular diastole 1. Ventricuclar pressure < Aortic Pressure = Aortic Valve closed 2. Atrial Pressure > Ventricular Pressure = AV valves open. 3. Blood squeezed from atria into ventricles. 4. Electrical impulse enters ventricles from the AV node. 5. Ventricles begin to depolarize. 6. R peak is end of ventricular diastole and start of ventricular systole. E. RS interval: Early ventricluar systole 1. Ventricles begin to contract. 2. Atrial Pressure < Ventricle Pressure = AV valves close 3. -

The Cardiovascular System
11 The Cardiovascular System WHAT The cardiovascular system delivers oxygen and HOW nutrients to the body tissues The heart pumps and carries away wastes blood throughout the body such as carbon dioxide in blood vessels. Blood flow via blood. requires both the pumping action of the heart and changes in blood pressure. WHY If the cardiovascular system cannot perform its functions, wastes build up in tissues. INSTRUCTORS Body organs fail to function properly, New Building Vocabulary and then, once oxygen becomes Coaching Activities for this depleted, they will die. chapter are assignable in hen most people hear the term cardio- only with the interstitial fluid in their immediate Wvascular system, they immediately think vicinity. Thus, some means of changing and of the heart. We have all felt our own “refreshing” these fluids is necessary to renew the heart “pound” from time to time when we are ner- nutrients and prevent pollution caused by vous. The crucial importance of the heart has been the buildup of wastes. Like a bustling factory, the recognized for ages. However, the cardiovascular body must have a transportation system to carry system is much more than just the heart, and its various “cargoes” back and forth. Instead of from a scientific and medical standpoint, it is roads, railway tracks, and subways, the body’s important to understand why this system is so vital delivery routes are its hollow blood vessels. to life. Most simply stated, the major function of the Night and day, minute after minute, our tril- cardiovascular system is transportation. Using lions of cells take up nutrients and excrete wastes. -

04. the Cardiac Cycle/Wiggers Diagram
Part I Anaesthesia Refresher Course – 2018 4 University of Cape Town The Cardiac Cycle The “Wiggers diagram” Prof. Justiaan Swanevelder Dept of Anaesthesia & Perioperative Medicine University of Cape Town Each cardiac cycle consists of a period of relaxation (diastole) followed by ventricular contraction (systole). During diastole the ventricles are relaxed to allow filling. In systole the right and left ventricles contract, ejecting blood into the pulmonary and systemic circulations respectively. Ventricles The left ventricle pumps blood into the systemic circulation via the aorta. The systemic vascular resistance (SVR) is 5–7 times greater than the pulmonary vascular resistance (PVR). This makes it a high-pressure system (compared with the pulmonary vascular system), which requires a greater mechanical power output from the left ventricle (LV). The free wall of the LV and the interventricular septum form the bulk of the muscle mass in the heart. A normal LV can develop intraventricular pressures up to 300 mmHg. Coronary perfusion to the LV occurs mainly in diastole, when the myocardium is relaxed. The right ventricle receives blood from the venae cavae and coronary circulation, and pumps it via the pulmonary vasculature into the LV. Since PVR is a fraction of SVR, pulmonary arterial pressures are relatively low and the wall thickness of the right ventricle (RV) is much less than that of the LV. The RV thus resembles a passive conduit rather than a pump. Coronary perfusion to the RV occurs continuously during systole and diastole because of the low intraventricular and intramural pressures. In spite of the anatomical differences, the mechanical behaviour of the RV and LV is very similar. -

Grade 6: the Heart and Circulatory System Lesson 1: the Heart Lesson 2: the Heart Rate Lesson 3: the Circulatory System and Blood
Grade 6: The Heart and Circulatory System Lesson 1: The Heart Lesson 2: The Heart Rate Lesson 3: The Circulatory System and Blood Objectives: 1. Students will identify the four chambers of the heart 2. Students will identify four important structures of the Circulatory System and what they do. 3. Students will explain heart rate and be able to take their resting and active heart rates. 4. Students will describe the major functions of the Circulatory System. 5. Students will explain the role of the heart in circulation 6. Students will give a basic explanation of the cardio-pulmonary sequence. 7. Students will describe systemic circulation. Materials: Lesson 1: • Animal heart (Example: cow, pig, sheep) • Note cards • Picture of the heart (See Figure 1) • Dissection tools (Scissors, pan, etc.) Lesson 2: • Small drum • Watch or clock with second hand, or time • Optional: Stethoscope Lesson 3: • Corn Syrup • Plastic Beads: flat red disks, white ovals, green or blue seed beads • “Explain” experiment (per group): o Two small balloons or large finger cots o One clear tube (1/2” diameter) about 8” long o One clear tube (3/4” diameter) about 8” long o 16 - 20 oz. water o Red food coloring o Measuring cup o Funnel o Two empty plastic containers (such as cottage cheese or yogurt cartons) Activity Summary: In this lesson students will learn the basic functioning of the heart, Circulatory System and blood, the connection to lung functioning, and the activity of the Grade 6: The Heart & Circulatory System – Revised 2008 Page 1 Circulatory System in the body. -
The Heart the Pulse and the ECG Booklet.Indd
AF A ® www.afa.org.uk The heart, the pulse and the electrocardiograph Providing information, support and access to established, new or innovative treatments for atrial fi brillation www.afa.org.uk Registered Charity No. 1122442 Glossary Arrhythmia Heart rhythm disorder Contents Arrhythmia Nurse Specialist A nurse who is Glossary trained in heart rhythm disorders The heart Atrial Fibrillation (AF) An irregular heart rhythm due to a rapid, disorganised electrical disturbance of The pulse the heart’s upper chambers (the atria) How to take a pulse Atrial Flutter (Afl ) A rhythm disorder of a more organised electrical disturbance in the heart’s upper The electrocardiograph chambers. The heart rhythm may be either regular (ECG) or irregular Bradycardia A rhythm disorder characterised by a slow heart rate of less than 60 beats per minute Cardiologist A doctor who specialises in the diagnosis and treatment of patients with heart conditions Echocardiogram An image of the heart using echocardiography or soundwave-based technology. An echocardiogram (echo) shows a three dimensional shot of the heart Electrocardiograph (ECG) A 2D graphic of the heart’s electrical activity. An ECG is taken from electrodes on the skin surface Heart Failure The inability (failure) of the heart to pump suffi cient oxygenated blood around the body to meet physiological requirements Sinus Rhythm Normal behaviour of the heart Syncope Fainting/passing out from a temporary lack of oxygen going to certain areas of the brain Tachycardia A rhythm disorder characterised by a rapid heart rate of more than 100 beats per minute 2 The heart The heart Structurally, the heart consists of two sides, a right and normal and a left. -
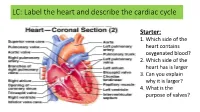
LC: Label the Heart and Describe the Cardiac Cycle
LC: Label the heart and describe the cardiac cycle Starter: 1. Which side of the heart contains oxygenated blood? 2. Which side of the heart has is larger 3. Can you explain why it is larger? 4. What is the purpose of valves? Can you label your heart………you can use a text book http://highered.mheducation.com/sites/00 72507470/student_view0/chapter20/anima tion__the_cardiac_cycle__quiz_1_.html Heart Valves The heart valves open and close passively because of pressure differences on either side of the valve. When pressure is greater behind the valve, the leaflets are blown open and the blood flows through the valve. However, when pressure is greater in front of the valve, the leaflets snap shut and blood flow is stopped AV Valves • The atrioventricular valves (AV valves), which separate the atria from the ventricles, allow blood to flow from the atria to the ventricles, but prevent flow in the opposite direction. • The right AV valves is called the tricuspid valve. The left AV valve is called the mitral valve. The opening and closing of the AV valves is dependent on pressure differences between the atria and ventricles. • When the ventricles relax, atrial pressure exceeds ventricular pressure, the AV valves are pushed open and blood flows into the ventricles. However, when the ventricles contract, ventricular pressure exceeds atrial pressure causing the AV valves to snap shut. Semi-lunar valves • The semilunar valves (pulmonary valve and aortic valve) are one-way valves that separate the ventricles from major arteries. The aortic valve separates the left ventricle from the aorta, while the pulmonary valve separates the right ventricle from the pulmonary artery.