CJRDP JCDRP Volume 8, No
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
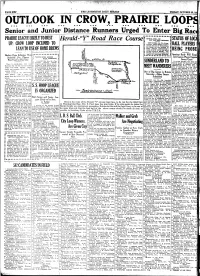
OUTLOOK in GROW, PRAIRIE LOOP! R
f i: (THE LETHBRIDGE DAILY HERALD PAGE sis* 'FRIDAY, OCTOBER 23,10: OUTLOOK IN GROW, PRAIRIE LOOP! » «. + » * » • • • • • • • •• • • • • • • • ! • • • • • • • • • • • • • • • Senior and Junior Distance Runners Urged To Enter Big Rac • • RITOLA WILL GO PRAIRIE LEAGUE LIKELY TO BUST • STATUS OFUO Herald-"Y" Road Race Course OUT FOR NEW RECORDS • NEW YORK, Oct. 23.—Twen UP; CROW LOOP INCLINED TO ty-seven United States outdoor records will fall if Willie Ritoia BALLPLAYERS! his hopes for ms attempt to lower Hannes Koblemainen's IAN TO USE OF HOME BREWS mark of 51:03 2-5 for ten miles BE1NG_PR0BE in New York on Sunday. The records all held by himself, are mostly for fractional distances. Hockey Dope Indicates That .;. .j. .j. .;. • * •> Amateur Body Will Enquf Scramble For Players TIGERS OPEN SEASON • Into Games Played Againsj WITH ROSEBUDS Won't Go Far This \ear Si! Sweet Grass VANCOUVER, Oct. 22.—The It is just possible that final gan, tentative Western Hockey — yg—" f SUNDERLAND TO will be played for the junior bnsetj There is considerable talk that League schedule drawn up, ac championship ot Alberta, Bays Ti Medicine Hat will line up in a hookey cording to word received here 5 Medicine Hat News. The Typo j from the headquarters of Presi iors of Medicine Hat and Maclt ieague with Swift Current, Maple dent Richardson of the league, MEET WANDERERS juniors were fighting it out, with i Creek and probable Gull Lake the • at Calgary, increases the num Hatters needing but one win to gi coming winter.. ber of home games for each the honors. However, that game v Taber is not at all enthusiastic team from 14 to 15. -

Women's Suffrage in Ontario the Beginning of Women’S Suffrage Movements
LEGISLATIVE ASSEMBLY an educational resource OF ONTARIO MESSAGE TO TEACHERS This educational resource was developed to compliment the documentary Women Should Vote: A Short History of how Women Won the Franchise in Ontario (www.ola.org/en/visit-learn/ about-ontarios-parliament/womens-suffrage-ontario), A NOTE ON LANGUAGE which tells the story of the struggle for women’s Some historical terms used in this resource are suffrage in Ontario at the turn of the 20th century. no longer in common use. First Nations peoples in Canada were initially called “Indians” by colonial It invites students to deepen their understanding of Europeans. This term is no longer used, though gender equality and democracy through examining and “Status Indian” is still a legal definition and is analyzing the suffrage movement, and facilitates mentioned throughout this guide. “Status Indian” engaging discussions and activities. Students will does not include all Indigenous peoples – for examine issues of identity, equity, activism and example, Métis and Inuit are excluded (see the justice in historical and contemporary contexts. Glossary on Page 22 for more information). CONTENTS The Suffrage Movement in Running the Good Race ............. 9 Glossary ......................... 22 Ontario: Votes for Women ............ 2 Indigenous Suffrage ............... 11 Activities The Beginning of Women’s Clues from the Archives Suffrage Movements ................ 3 Final Reflections ..................13 (Designed for Grades 8-12) .......23 Should I Support the Vote? The Long Road Timeline of Women’s Suffrage (Designed for Grades 4-7) ........24 to Women’s Suffrage ................ 4 in Ontario and Canada ............. 14 Our Rights Today ................25 A New Century ..................... 5 Feature Figures Appendix A ...................... -

The Woman Candidate for the Ontario Legislative Assembly, 1919-1929 Frederick Brent Scollie
Document généré le 27 sept. 2021 11:37 Ontario History The Woman Candidate for the Ontario Legislative Assembly, 1919-1929 Frederick Brent Scollie Volume 104, numéro 2, fall 2012 Résumé de l'article L’histoire brosse un tableau sombre du manque de succès électoral des femmes URI : https://id.erudit.org/iderudit/1065435ar ontariennes après 1919, l’année où elles ont obtenu le droit d’être élues à la DOI : https://doi.org/10.7202/1065435ar législature et aux conseils municipaux. Nous examinons de près treize des 21 femmes qui ont posé leur candidature à l’Assemblée législative de l’Ontario Aller au sommaire du numéro avant 1943, notamment les douze qui furent candidates entre 1919-1929, toutes vaincues, le succès politique de quelques-unes de leurs prédécesseurs élues à des commissions scolaires dès 1892, et l’expérience de ces femmes avec les Éditeur(s) partis politiques. Cela nous permet de vérifier les thèses et explications offertes par la politologue Sylvia Bashevkin et la sociologue Thelma McCormack sur le The Ontario Historical Society comportement politique des femmes au Canada anglais. ISSN 0030-2953 (imprimé) 2371-4654 (numérique) Découvrir la revue Citer cet article Scollie, F. B. (2012). The Woman Candidate for the Ontario Legislative Assembly, 1919-1929. Ontario History, 104(2), 1–27. https://doi.org/10.7202/1065435ar Copyright © The Ontario Historical Society, 2012 Ce document est protégé par la loi sur le droit d’auteur. L’utilisation des services d’Érudit (y compris la reproduction) est assujettie à sa politique d’utilisation que vous pouvez consulter en ligne. -

Exhibit 5.2A
Ontario Stroke Evaluation Report 2011 Supplementary Materials Exhibit 5.2a 184 Age- and sex-adjusted revisit or readmission rates within 365 days following stroke or transient ischemic attack (TIA), in Ontario and by stroke type, OSS region, OSS classification and Local Health Integration Network, 2003/04 to 2008/09 Adjusted1 Revisit/Readmission Rate (%) Group/Sub-Group 2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 Ontario2 11.8 11.9 10.9 10.7 10.8 10.6 Stroke Type Intracerebral hemorrhage 9.0 10.6 8.9 8.2 7.8 7.2 Ischemic stroke 10.8 11.0 9.9 9.9 9.7 9.9 Subarachnoid hemorrhage 7.8 7.5 7.0 6.5 7.1 6.6 Transient ischemic attack 14.2 13.8 13.0 12.8 13.3 12.5 Ontario Stroke System Region Central East 12.6 11.2 11.3 11.4 11.5 11.2 Central South 11.4 11.1 11.6 10.1 10.1 10.3 East – Champlain 11.5 14.4 10.6 11.9 11.5 10.4 Northeast 12.6 12.9 10.6 12.4 13.0 10.3 Northwest 12.5 14.8 11.5 10.3 12.2 9.4 South East 13.2 14.1 8.1 11.1 11.5 10.8 Southwest 11.9 10.9 12.2 10.8 11.0 10.7 Toronto – North & East 10.7 10.8 9.4 8.4 9.1 9.7 Toronto – Southeast 11.7 12.2 11.3 13.1 9.9 9.9 Toronto – West 9.8 13.0 10.3 9.9 11.4 11.6 West GTA 12.3 11.1 10.3 9.6 9.2 10.8 Ontario Stroke System Classification Regional stroke centre 10.8 11.3 9.8 9.9 10.6 10.3 District stroke centre 12.7 12.2 10.7 10.2 10.7 9.8 Non-designated 12.0 12.1 11.5 11.3 10.9 11.0 Local Health Integration Network 1. -
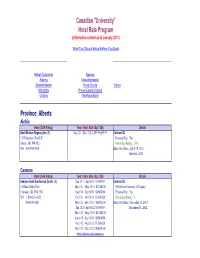
2011-2012 Canadian University Hotel Rate Program.Xlsx
Canadian "University" Hotel Rate Program (information current as of January 2011) What You Should Know Before You Book British Columbia Quebec Alberta New Brunswick Saskatchewan Nova Scotia Yukon Manitoba Prince Edward Island Ontario Newfoundland Province: Alberta Airdrie Hotel (CAA Rating) Term / Univ. Rate (Sgl / Dbl) Details Best Western Regency Inn (1) Jan 1/11 - Dec 31/12 $99.99/$99.99 Contract ID: 121 Edmonton Trail S.E. Personal Use: Yes Airdrie, AB T4B 1S2 Green Key Rating : N/A Tel: 403-948-3838 Black Out Dates: July 8-18, 2011 July 6-16, 2012 Canmore Hotel (CAA Rating) Term / Univ. Rate (Sgl / Dbl) Details Radison Hotel Conference Center (3) Jan 1/11 - Apr 30/11 $ 109/109 Contract ID: 511 Bow Valley Trail May 1/11 - May 31/11 $124/$124 90 km from University of Calgary Canmore, AB T1W 1N7 Jun 1/11 - Sep 30/11 $154/$154 Personal Use: Yes Tel: 1-800-263-3625 Oct 1/11 - Oct 31/11 $124/$124 Green Key Rating : 4 403-678-3625 Nov 1/11 - Dec 31/11 $109/$109 Black Out Dates: December 31, 2011 Jan 1/12 - Apr 30/12 $ 109/109 December 31, 2012 May 1/12 - May 31/12 $124/$124 Jun 1/12 - Sep 30/12 $154/$154 Oct 1/12 - Oct 31/12 $124/$124 Nov 1/12 - Dec 31/12 $109/$109 www.radison.com/canmoreca Calgary Hotel (CAA Rating) Term / Univ. Rate (Sgl / Dbl) Details The Westin Calgary (4) Jan 01/11 - Jul 10/11 $239/$239 Contract ID: 328193 320-4th Ave SW Jul 11/11 - Jul 14/11 $299/$299 5 km from University of Calgary Calgary, AB T2P 2S6 Jul 15/11 - Dec 31/11 $239/$239 Personal Use: No Tel: 1-800-937-8461 Jan 1/12 - Jul 7/12 $249/249 Green Key Rating : 4 403-266-1611 Jul 8/12 - Jul 12/12 $299/$299 Black Out Dates: 2012/06/10 - 2012/06/14 Jul 13/12 - Dec 31/12 $249/$249 www.westin.com/calgary Hyatt Regency Calgary (4) Jan 1/11 - Dec 31/12 $239/$239 Contract ID: Book "Univ" Rate 700 Centre St. -

2007 to 31 December 2007
A N N U A L R E P O R T of the JUSTICES OF THE PEACE APPOINTMENTS ADVISORY COMMITTEE for the Period from 1 January 2007 to 31 December 2007 Toronto, Ontario January 2009 A N N U A L R E P O R T of the JUSTICES OF THE PEACE APPOINTMENTS ADVISORY COMMITTEE for the Period from 1 January 2007 to 31 December 2007 Toronto, Ontario January 2009 ISSN 1918-4166 (Bilingual print) ISSN 1918-4174 (English Internet) ISSN 1918-4182 (French Internet) Persons wishing to comment on the process of the Justices of the Peace Appointments Advisory Committee are invited to write to: The Chair Justices of the Peace Appointments Advisory Committee 3rd Floor 720 Bay Street Toronto, Ontario M5G 2K1 TABLE OF CONTENTS LETTER OF TRANSMITTAL ................................................................................ 1 CHAIR‟S SUMMARY ............................................................................................ 3 INTRODUCTION .................................................................................................. 5 THE COMMITTEE‟S PROCESS ........................................................................... 6 STATISTICS ......................................................................................................... 9 APPENDICES: APPENDIX A – Legislation ................................................................................. 11 APPENDIX B – Justices of the Peace Appointments Advisory Committee Member Biographies ................................................................. 15 APPENDIX C – Application Form ...................................................................... -

Protestants, the Liberal State, and the Practice of Politics: Revisiting R.J
Document generated on 10/01/2021 12:31 a.m. Journal of the Canadian Historical Association Revue de la Société historique du Canada Protestants, the Liberal State, and the Practice of Politics: Revisiting R.J. Fleming and the 1890s Toronto Streetcar Controversy Marguerite Van Die Volume 24, Number 1, 2013 Article abstract Through the lens of R. J. Fleming, Irish Methodist businessman, alderman, and URI: https://id.erudit.org/iderudit/1024998ar four times mayor of Toronto in the 1890s, this paper re-examines the moral DOI: https://doi.org/10.7202/1024998ar reform campaigns of middle-class Protestants described by Christopher Armstrong and H. V. Nelles in their now classic study, The Revenge of the See table of contents Methodist Bicycle Company (1977). Instead of looking at the Sunday car issue from the perspective of the promoters and as evidence of secularization, it presents as a case study Fleming’s conflicted and controversial role as an Publisher(s) evangelical politician confronted with a divisive moral and religious issue within the late nineteenth-century liberal state. Scholarly debates on the The Canadian Historical Association / La Société historique du Canada process of secularization in late nineteenth-century Canada have given little attention to the influence of the timing and nature of the country’s political ISSN arrangements and have thus neglected the contradictions and tensions devout politicians faced within the new state and social order. This paper argues the 0847-4478 (print) need to make an important but often overlooked distinction between political 1712-6274 (digital) and social secularization. With close attention to detail, it examines Fleming as an “evangelical modernizer” who as a politician had to maintain the neutrality Explore this journal of the state and at the same time address the concerns of a religious constituency that feared a favourable vote on Sunday cars would lead to social secularization. -
"Whose Servant I Am" : Speakers of the Assemblies of the Province Of
Legislative Library '"^^VMfiose SewcmtDS^ U)B7 ^--j(ji,i*^?**6^=^^i ^ ~ LIBRARFo^ TORONTO JAN 2 1994 A CAZON LL "7 ^ .- ; -a. "Whose Servant I Am " Speakers of the Assemblies of the Provinces of Upper Canada, Canada and Ontario, 1792-1992 Clare A. Dale iToronto )ntario Legislative Library [1992 Canadian Cataloguing in Publication Data Dale, Clare A., 1964- "Whose servant I am" : speakers of the assemblies of the provinces of Upper Canada, Canada and Ontario, 1792-1992 Includes bibliographical references. ISBN 0-7729-9343-2 1. Ontario. Legislative Assembly—Speaker—History. 2. Upper Canada. Legislature. House of Assembly—Speaker—History. 3. Canada. Legislature. Legislative Assembly—Speaker—History. 4. Legislative bodies—Ontario- Presiding officer. I. Ontario. Legislative Library. II. Title. III. Title: Speakers of the assemblies of the provinces of Upper Canada, Canada and Ontario, 1792-1992. JL274.S65D34 1992 328.713*0762 C92-092524-3 Cover: "The First Legislature of Upper Canada," by Frederick S. Challener based on a watercolour sketch by Charles W. Jefferys. (The Ontario Art Collection.) Photo: Thomas Moore Photography Inc. Cette publication existe 6galement en frangais sous le titre : «Dontje suis le serviteur» : les presidents des assemblies des provinces du Haut-Canada, du Canada et de I 'Ontario de 1792 d 1992. Errata, page 330. ® "Whose Servant I Am" Contents Foreword i Introduction iv The House of Assembly of the Province of Upper Canada, 1792-1841 John McDonell (Aberchalder) 1 David William Smith 8 Samuel Street 17 Richard Beasley 27 Alexander McDonell (Collachie) 34 Allan McLean 41 Levius Peters Sherwood 49 John Willson -. 56 Marshall Spring Bidwell 62 Archibald McLean 69 Allan Napier MacNab 77 Henry Ruttan 85 The Legislative Assembly of the Province of Canada, 1841-1867 Austin (Augustin) Cuvillier 91 Allan Napier MacNab (Photograph only) Augustin-Norbert Morin 98 John Sandfield Macdonald 106 Louis-Victor Sicotte 114 Henry Smith, Jr. -

86 CONSTITUTION and GOVERNMENT -Population Of
86 CONSTITUTION AND GOVERNMENT -Population of Electoral Districts, Voters on Lists and Votes Polled, Names and Addresses of members of the House of Commons, as Elected at the Seventeenth General Election—continued. Province and Popula Voters Votes Electoral District. tion, Name of Member. P.O. Address. 1931. on List. Polled. Ontario—continued. 83,808 43,231 27,993 Robinson, S. C Walkerville, Ont. Fort William 36,040 14,412 10,861 Vlanion, Hon. R. J.. Fort William, Ont. Frontenac-Addington 29,434 17,058 11,537 18,666 10,615 8,948 McGillis, A 32,425 20,645 14,612 ^asselman, A. C.. 30,288 18,899 15,068 Porteous, V. C 27,411 16,912 13,028 Macphail, Agnes C 21.428 12,835 11,064 Senn, M. C 26,558 16,035 12,826 Milton, Ont. 66,771 36,829 21,475 Rennie, G. S.2 56,305 30,928 17,335 Bell, C. W Hastings-Peterborough.... 27,160 14,80^ 10,034 Embury, A. T Bancroft, Ont. 39,327 22,563 18,548 Tummon, W. E Tweed, Ont. 22,662 14,488 12,116 Spotton, Geo 22,518 14,146 12,035 McMillan, T.= Kenora-Rainy River 33,925 15,661 12,178 Kenora, Ont. 54,715 29,006 23,051 Rutherford, J. W.... Kent 26,180 14,569 11,164 26,736 16,391 12,622 Sproule, J. T 34,040 18,957 15,236 32,856 20,816 16,815 Gray, R. W 35,157 20,987 15,699 Thompson, T. A.... 54,199 30,802 21,076 Stewart, Hon. -

An Ethnic Coalition: the Liberal Party of Canada and the Engagement of Ethnocultural Communities, 1959-1974
An Ethnic Coalition: the Liberal Party of Canada and the Engagement of Ethnocultural Communities, 1959-1974 by Thirstan Falconer B.A., University of Waterloo 2010 M.A., University of Waterloo 2012 A Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree of DOCTOR OF PHILOSOPHY In the Department of History © Thirstan Falconer, 2017 University of Victoria All rights reserved. This dissertation may not be reproduced in whole or in part, by photocopy or other means, without the permission of the author. ii Supervisory Committee An Ethnic Coalition: The Liberal Party of Canada and the Engagement of Ethnocultural Communities, 1959-1974 by Thirstan Falconer B.A., University of Waterloo, 2010 M.A., University of Waterloo, 2012 Supervisory Committee Dr. Penny Bryden, (Department of History) Supervisor Dr. Jordan Stanger-Ross, (Department of History) Department Member Dr. Matt James, (Department of Political Science) Outside Member iii Abstract Supervisory Committee Dr. Penny Bryden, (Department of History) Supervisor Dr. Jordan Stanger-Ross, (Department of History) Department Member Dr. Matt James, (Department of Political Science) Outside Member During the 1960s and 1970s the Liberal Party of Canada sought to engage ethnocultural communities in an effort to win federal elections. The author argues that the Liberal Party’s relationship with ethnocultural communities in Metro Toronto during the 1960s was characterized by indifference. Though it adopted a programme that encouraged the courting of ethnocultural communities, the Pearson-led Liberal Party showed limited interest in recognizing ethnocultural communities as a part of the party’s electoral coalition. The efforts of Andrew Thompson, the Liberal Party’s Ethnic Liaison Officer during the Pearson years, were separated from the rest of party’s organization and campaign structure. -

Woodbine & Steeles Corporate Centre
WOODBINE & STEELES CORPORATE CENTRE OFFICE SPACE FOR LEASE WOODBINE & STEELES CORPORATE CENTRE 7030 WOODBINE AVENUE Suite 400C 6,400 sf – Improved Suite 900A 4,709 sf – Improved 13,915 sf contiguous Suite 900B 9,206 sf – Base building 7050 WOODBINE AVENUE Suite 201 4,007 sf – Improved with quality boardroom Suite 400 13,949 sf – Full floor – building signage available 7100 WOODBINE AVENUE Suite 110 1,332 sf – Corner suite, 4 offices & kitchenette Suite 202 3,436 sf – Available January 1, 2018 Suite 215b 2,611 sf – Improved WOODBINE & STEELES CORPORATE CENTRE FACT SHEET Net Rent $15.75 psf per annum Additional Rent $13.99 psf per annum Parking Ratio 3.1 per 1,000 sf Year Built 1984 Woodbine & Steeles Corporate Centre is a premier, suburban 7030 WOODBINE AVENUE FEATURES office complex totaling approximately 295,000 square feet. The Building Size 120,000 sf Underground Parking property is situated on 12 acres and comprises three office buildings ranging from four to nine storeys, fronting on Woodbine and Steeles. Typical Floor Plate 13,550 sf Surface Parking (3.1/1000) Number of Floors 9 The complex, located in the City of Markham, has a prominent and Public Transit highly visible location at Highway 404 and Steeles Avenue, five minutes 7050 WOODBINE AVENUE Direct Subway Connection north of the Highway 401 interchange. The property offers excellent highway access to several 400 series highways, making it a strong Building Size 52,000 sf Modern Renovated Lobby location for tenants who want to attract employees from across the Typical Floor Plate 13,577 sf Satellite Dish Capability GTA. -
Chapter Page
Missing Links A History of Toronto’s Controversial Unfinished Expressway System James B. Alcock 2 This book is dedicated to Sam Cass, Commissioner of Metropolitan Toronto Roads and Traffic 1968 to 1989 3 4 TABLE OF CONTENTS Chapter Page 1 Introduction 7 2 The Creation of Metropolitan Toronto 1945-1954 10 3 The Age Of New Expressways 1954-1969 16 4 Revolt Against Expressways 1969-1975 26 5 A Brief Revival Of Expressways 1975-1980 34 6 Arterial Highways 1980-1998 39 7 Amalgamation 1998-2006 53 8 Expressways To Boulevards 2006-2015 65 9 Toll Roads 2015-Present 74 MAPS Metropolitan Toronto Expressways 1966 2 1947 Plan for Lake Shore (later Gardiner) Expressway 14 Early Toronto Highways Plans from the 1940’s 15 Plans for the Spadina Expressway south from Lawrence Avenue West 21 Scarborough Expressway Plan – 1967 Alignment 22 Crosstown Expressway Plan – 1961 Alignment 23 Highway 400 Extension Plan 24 Richview Expressway Plans 25 Scarborough Expressway Plan – 1973 Alignment 31 Proposed Alignments for the Highway 400 Extension 33 Schedule of repairs to the elevated Gardiner Expressway 70 City of Toronto Expressways Today 75 TORONTO EXPRESSWAY HISTORY TIMELINE 1958 Gardiner Expressway opens Humber River to Dunn Avenue 1961 Don Valley Parkway opens Bloor Street to Eglinton Avenue 1962 Gardiner Expressway opens to York Street 1963 Don Valley Parkway opens to Lawrence Avenue 1964 Gardiner Expressway and Don Valley Parkway connected at the Don River mouth 1966 Gardiner Expressway opens to Leslie Street, Don Valley Parkway opens to Sheppard Avenue,