East Coast Drugsv3 with Appendi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

GAA Competition Report
Wicklow Centre of Excellence Ballinakill Rathdrum Co. Wicklow. Rathdrum Co. Wicklow. Co. Wicklow Master Fixture List 2019 A67 HW86 15-02-2019 (Fri) Division 1 Senior Football League Round 2 Baltinglass 20:00 Baltinglass V Kiltegan Referee: Kieron Kenny Hollywood 20:00 Hollywood V St Patrick's Wicklow Referee: Noel Kinsella 17-02-2019 (Sun) Division 1 Senior Football League Round 2 Blessington 11:00 Blessington V AGB Referee: Pat Dunne Rathnew 11:00 Rathnew V Tinahely Referee: John Keenan Division 1A Senior Football League Round 2 Kilmacanogue 11:00 Kilmacanogue V Bray Emmets Gaa Club Referee: Phillip Bracken Carnew 11:00 Carnew V Éire Óg Greystones Referee: Darragh Byrne Newtown GAA 11:00 Newtown V Annacurra Referee: Stephen Fagan Dunlavin 11:00 Dunlavin V Avondale Referee: Garrett Whelan 22-02-2019 (Fri) Division 3 Football League Round 1 Hollywood 20:00 Hollywood V Avoca Referee: Noel Kinsella Division 1 Senior Football League Round 3 Baltinglass 19:30 Baltinglass V Tinahely Referee: John Keenan Page: 1 of 38 22-02-2019 (Fri) Division 1A Senior Football League Round 3 Annacurra 20:00 Annacurra V Carnew Referee: Anthony Nolan 23-02-2019 (Sat) Division 3 Football League Round 1 Knockananna 15:00 Knockananna V Tinahely Referee: Chris Canavan St. Mary's GAA Club 15:00 Enniskerry V Shillelagh / Coolboy Referee: Eddie Leonard 15:00 Lacken-Kilbride V Blessington Referee: Liam Cullen Aughrim GAA Club 15:00 Aughrim V Éire Óg Greystones Referee: Brendan Furlong Wicklow Town 16:15 St Patrick's Wicklow V Ashford Referee: Eugene O Brien Division -

Wicklow Coaching Calendar 2020
WICKLOW GAA 2020 Coach Education Calendar Because Knowledge is Power TURAS – the Irish word for Journey – it was chosen to support the journey taken by both coaches and players up through the age grades. Player Centered and Coach Driven Better Coaches + Better Players = Better Teams Join, like or follow us for updates on social media Twitter Facebook Website Officialwicklowgaa.ie Wicklow GAA Coach Education Education Programme 2020 Coaches are encouraged to participate practically to maximize their opportunity for learning. Our programme is designed to support all coaches working at child, youth and adult level through specifically planned courses and workshops incorporating all that is good in terms of coaching best practice. Again this year in attempting to meet the mandatory coaching standards as set out by the GAA we are organising the required amount of coaching courses to meet these targets.The Games Development programme for this year provides the best possible support for coaches in relation to Coach Education and Coaching Workshops.TURAS principles should run throughout the coaching & games programme at all levels. As such, all stakeholders Players, Coaches, Managers, Academy leaders & Parents will speak a common language and follow a common pathway as they progress on their TURAS Pathway. TURAS Principals The kep principals underpinning coaching on the Wicklow GAA Coach Development are presented using the acronym TURAS. TURAS is the Irish for journey, it was purposefully chosed to reflect the journey that is player coach development. -
Listing and Index of Evening Herald Articles 1938 ~ 1975 by J
Listing and Index of Evening Herald Articles 1938 ~ 1975 by J. B. Malone on Walks ~ Cycles ~ Drives compiled by Frank Tracy SOUTH DUBLIN LIBRARIES - OCTOBER 2014 SOUTH DUBLIN LIBRARIES - OCTOBER 2014 Listing and Index of Evening Herald Articles 1938 ~ 1975 by J. B. Malone on Walks ~ Cycles ~ Drives compiled by Frank Tracy SOUTH DUBLIN LIBRARIES - OCTOBER 2014 Copyright 2014 Local Studies Section South Dublin Libraries ISBN 978-0-9575115-5-2 Design and Layout by Sinéad Rafferty Printed in Ireland by GRAPHPRINT LTD Unit A9 Calmount Business Park Dublin 12 Published October 2014 by: Local Studies Section South Dublin Libraries Headquarters Local Studies Section South Dublin Libraries Headquarters County Library Unit 1 County Hall Square Industrial Complex Town Centre Town Centre Tallaght Tallaght Dublin 24 Dublin 24 Phone 353 (0)1 462 0073 Phone 353 (0)1 459 7834 Email: [email protected] Fax 353 (0)1 459 7872 www.southdublin.ie www.southdublinlibraries.ie Contents Page Foreword from Mayor Fintan Warfield ..............................................................................5 Introduction .......................................................................................................................7 Listing of Evening Herald Articles 1938 – 1975 .......................................................9-133 Index - Mountains ..................................................................................................134-137 Index - Some Popular Locations .................................................................................. -
Mangans Loop Tinahely 9.2 Km - Moderate (Allow 2.5 Hours) Looped Walks Terrain: Laneways & Hillside Tracks General Information Suitable for Regular Walkers
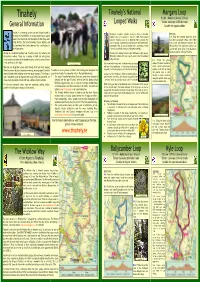
Tinahely’s National Mangans Loop Tinahely 9.2 km - Moderate (allow 2.5 hours) Looped Walks Terrain: Laneways & hillside tracks General Information Suitable for regular walkers Tinahely is a charming picture postcard village located in Tinahely is a walkers’ paradise, offering a choice of beautiful DIRECTIONS: the heart of South Wicklow. Its unique Market Square layout walking trails and a welcome to match. In 2009, Fáilte Ireland A-B: From the trailhead follow the green makes it the ideal start and finish point for the many walks selected Tinahely as one of six WALKING HUBS in Ireland. The (and blue and purple) arrows. After 100m in the locality. The attractive Market Square Building and local community, in partnership with landowners and Fáilte Ireland, cross a stile and continue to junction with the Courthouse Arts Centre dominate the architecture of constructed 31km of off-road walking trails, consisting of three Wicklow Way. Turn right here and the loop the village centre. National Looped Walks; Mangans, Ballycumber and Kyle. ascends with great views of the Blackstairs Mountains and the valley of Tinahely. Already an established walking hub, Tinahely caters for national and Tinahely’s first Walking Festival in April 2010 was attended by over international walkers. There are a number of B&B and self-catering 500 visiting walkers and is now a yearly event on the first weekend Dr. James Mc Namara’s Memorial Cross accommodation providers in the immediate area, as well as several places in May each year. B-C: Follow the green to eat and drink in the village. -
2016 – 2022 Record of Protected Structures
COUNTY Record of Protected Structures 2016 – 2022 WICKLOW COUNTY DEVELOPMENT PLAN Comhairle Contae Chill Mhantáin DECEMBER 2016 Wicklow County Council - Record of Protected Structures Each development plan must include policy objectives to protect structures or parts of structures of special interest within its functional area under Section 10 of the Planning and Development Act, 2000. The primary means of achieving this objective is for the planning authority to compile and maintain a record of protected structures to be included in the development plan. A planning authority is obliged to include in the Record of Protected Structures every structure which, in its opinion, is of special architectural, historical, archaeological, artistic, cultural, scientific, social or technical interest. A ‘protected structure’ is defined as any structure or specified part of a structure, which is included in the Record of Protected Structures. A structure is defined by the Planning and Development Act, 2000 as ‘any building, structure, excavation, or other thing constructed or made on, in or under any land, or any part of a structure’. In relation to a protected structure, the meaning of the term ‘structure’ is expanded to include: (a) the interior of the structure; (b) the land lying within the curtilage of the structure; (c) any other structures lying within that curtilage and their interiors, and (d) all fixtures and features which form part of the interior or exterior of the above structures. Where indicated in the Record of Protected Structures, protection may also include any specified feature within the attendant grounds of the structure which would not otherwise be included. -

RPII –03/1 Radon in Drinking Water in Co. Wicklow
RPII –03/1 Radon in Drinking Water in Co. Wicklow – a Pilot Study T.P. Ryan S. Sequeira L. McKittrick P.A. Colgan February 2003 Table of Contents List of Tables .............................................................................................................................ii List of Figures............................................................................................................................ii Summary...................................................................................................................................iii 1. INTRODUCTION....................................................................................................... 1 2. PILOT STUDY OBJECTIVES................................................................................... 2 3. SAMPLING AND ANALYSIS .................................................................................. 2 3.1 Radon in Drinking Water Sampling Protocol ............................................................. 2 3.2 Radon in Drinking Water Analysis ............................................................................. 4 3.3 Analysis of Other Radionuclides................................................................................. 5 4. RESULTS AND DISCUSSION ................................................................................. 5 4.1 Radon in Drinking Water ............................................................................................ 5 4.2 Detailed Investigations............................................................................................... -
Marref-2015-Wicklow-Tally.Pdf
Box No LEA Polling District Polling Station Yes No Postal 188 137 1 Arklow Annacurragh Annacurra N.S. 134 127 2 Arklow Arklow Rock Carysfort N.S., Booth 5A 245 180 3 Arklow Arklow Town Carysfort N.S., Booth 1 345 102 4 Arklow Arklow Town Carysfort N.S., Booth 2 287 195 5 Arklow Arklow Town Carysfort N.S., Booth 3 363 113 6 Arklow Arklow Town Carysfort N.S., Booth 4 281 170 7 Arklow Arklow Town St Peters N.S. Bth 1 Castle Park 259 144 8 Arklow Arklow Town St Peters N.S. Bth 2 Castle Park 200 157 9 Arklow Arklow Town St Peters N.S. Bth 3 Castle Park 223 178 10 Arklow Arklow Town St Peters N.S. Bth 4 Castle Park 204 151 11 Arklow Arklow Town St Peters N.S. Bth 5 Castle Park 207 182 12 Arklow Arklow Town Templerainey N.S., Booth 1 247 135 13 Arklow Arklow Town Templerainey N.S., Booth 2 242 107 14 Arklow Arklow Town Templerainey N.S., Booth 3 240 115 15 Arklow Aughavanagh Askanagap Community Hall, Booth 1 42 54 16 Arklow Aughrim Aughrim N.S.,Booth 1 230 141 17 Arklow Aughrim Aughrim N.S.,Booth 2 221 146 18 Arklow Avoca St Patricks N.S., Booth 1, Avoca 172 110 19 Arklow Avoca St Patricks N.S., Booth 2, Avoca 236 111 20 Arklow Ballinaclash Ballinaclash Community Centre 255 128 21 Arklow Ballycoogue Ballycoogue N.S. 97 83 22 Arklow Barnacleagh St Patricks N.S., Barnacleagh 149 111 23 Arklow Barndarrig South Barndarrig N.S. -

Under 7 & 9 Hurling & Football Fixtures Give Respect, Get Respect
The Garden County Go Games Little Buds Programme A Place where all Children Bloom Under 7 & 9 Hurling & Football Fixtures Give Respect, Get Respect Recommendations for Age Groups 2017 Under 7 Under 9 Players born in 2010 & 2011 Players born in 2008 & 2009 Football Friday Night Clubs/18 Clubs Saturday Morning Clubs/18 Clubs Avoca Kilbride/Lacken AGB Blessington Barndarrig Valleymount St Patricks Hollywood Rathnew Dunlavin Ashford Donard/Glen Avondale Stratford/Grangecon Laragh Baltinglass Ballinacor Kiltegan An Tochar Knockananna Kilmacanogue Ballymanus Enniskerry Tinahely Bray Emmets Shillelagh Fergal Ogs Coolkenno Eire Og Greystones Carnew Kilcoole Coolboy Newtown Annacurra Newcastle Aughrim Hurling Friday Night Clubs / 16 Clubs Barndarrig Kilmacanogue Kiltegan St Patricks Kilcoole Tinahely Avondale Bray Emmets Kilcoole Carnew Fergal Ogs Glenealy Aughrim Eire Og Greystones ARP Stratford/Grangecon/Hollywood/Dunlavin The Full “Garden County Go Games Little Buds Programme” for 2017 will be sponsored by the Wicklow People Wicklow People are going to give us a lot of coverage but we need photos taken with the advertising board that will be supplied to each club. Club Go Games PR person to be appointed to send in photos for Twitter, Facebook and Wicklow People To the following Email Address shall be used immediately after each home blitz when returning photographs. We need all clubs corporation on this to ensure we have a good quality section in the Wicklow People each week. The onus is on the Home club to take the photographs of all teams -

Draft Wicklow County Development Plan 2021-2027
30th August 2021 Forward Planning, Wicklow County Council, Station Road, Wicklow Town, A67 FW96. Re: Draft Wicklow County Development Plan 2021-2027 A chara, Thank you for your authority’s work in preparing the draft Wicklow County Development Plan 2021-2027 (the draft Plan). The Office of the Planning Regulator (the Office) wishes to acknowledge the considerable work your authority has undertaken in the preparation of the draft Plan against the backdrop of an evolving national and regional planning policy and regulatory context. In particular, the inclusion of Strategic County Outcomes in the draft Plan which are informed by the NPF, the RSES and key issues arising in submissions from members of the public is commended and this approach assists in demonstrating consistency with the national and regional policy frameworks in a clear manner. Subsequent to the publication of the draft Plan you will also have been notified of the publication for consultation of the draft Development Plans Guidelines for Planning Authorities by the Department of Housing, Local Government and Planning (August 2021) which will also provide clarity and assistance to planning authorities in the completion of development plans, notwithstanding that the Guidelines are in draft form. 4ú hUrlár, Teach na Páirce, 191-193A An Cuarbhóthar Thuaidh, Baile Átha Cliath 7, D07 EWV4. 4th Floor, Park House, 191-193A North Circular Road, Dublin 7, D07 EWV4. T +353 (0)1 553 0270 | E [email protected] | W www.opr.ie As your authority is aware, a key function of the Office is the assessment of statutory plans to ensure consistency with legislative and policy requirements relating to planning. -
Accommodation (Use This 2021)
Ballybeg can accommodate up to 44 of your nearest and dearest so that more of your guests can relax and savour the atmosphere with you throughout the three days of wedding celebrations. Please see below for recommended off-site guest accommodation that is in close proximity to Ballybeg. Recommended Hotel Accommodation From the elegance of the Brooklodge Hotel & Spa to the convenience of Murphy’s Hotel in Tinahely or comfort of Lawless’ in Aughrim - your guests have options aplenty as all are within a 15-minute drive of Ballybeg. Our local hackney service will ensure safe passage of guests to and from their accommodation at any hour of the day or night! The Brooklodge Hotel Macreddin, Aughrim, Co Wicklow. Map: A. Website: www.brooklodge.com Tel: +353 (0)402 26444. The Meath Arms Aughrim, Co. Wicklow. Map: C. Located in the middle of one of Ireland's tidiest villages, Aughrim is also known as the granite village. Owned and managed by the Phelan family, this exceptional, cozy, friendly and licensed premises is the essence of both comfort and charm, a truly lovely place to stay, and only 3-4 miles from Ballybeg. Contact: Gerry or Paul. Tel: +353 (0)402 36460 or +353 (0)87 293 5987. The Woodenbridge Hotel Woodenbridge, Arklow, Co.Wicklow. Map: D. Website: www.woodenbridgehotel.com Tel: +353 (0)402 35146. Murphy's Hotel 10 new beautiful rooms added to this well known spot. Main Street, Tinahely, Co. Wicklow. Map: E. Website: www.murphys-hotel.ie Tel: +353 (0)402 38109. Please Note: All listings are in alphabetical order Recommended Bed & Breakfast Accommodation Within 5 to 15 minutes drive from Ballybeg there is ample choice of B&Bs, which all come highly recommended by us and our guests. -

Mountain View AUTUMN 07 BC
THE NEWSLETTER OF WICKLOW UPLANDS COUNCIL AUTUMN 2007 LETTER FROM THE CHAIR Difficult though it is for some of us to comprehend, Wicklow Mountain Views 2007 marks the 10th anniversary of our foundation. Issue number 17: Autumn 2007 When one recalls how things were before we formed our network of those who live in, work in Published by: Our 2007 Annual General and use the Wicklow/Dublin landscape for Wicklow Uplands Council Ltd Meeting was a lively and well- recreation, we get some sense of what the Council Editor: Lenka Mulligan attended event. It also marked has achieved. Today, for example, we are in a the departure from the Board of strong position to reflect on Minister John Gormley’s David Rowe and Richard More- recent call for consultation around the development O’Ferrall, both of whom decided of a national landscape strategy. Our diverse that it was time to make room for some ‘new membership will enable us to respond to this issue blood’. I am grateful to both of them for their with some sort of rational debate. Of course, given outstanding contribution to our Executive and to the the widely divergent views that are ‘out there’, it will Board of Wicklow Uplands Council. not be easy to achieve consensus. David is a founding father and our first honorary Nevertheless, open discussion and a fair hearing member. His balanced and wise counsel informed for all points of view are very important and can our early days and continued unabated over the only help to facilitate mutual understanding and years. -

Tinahely Draft Town Plan
TTIINNAAHHEELLYY DDRRAAFFTT TTOOWWNN PPLLAANN Wicklow County Council October 2008 - 0 - TINAHELY DRAFT TOWN PLAN This document is in two sections: A Consists of a description of the process involved in the preparation and making of the Plan, including the statutory basis, details and reports of the consultation process, as well as the basis of and calculations for zoning. This part of the document is to enable an understanding of the basis of the assumptions and recommendations made in the Plan. This section will not form part of the final published Plan. While Part A will not be published once the Plan has been adopted, it will be available on the Wicklow County Council website, or at the Planning Office, for those who wish to further understand the process behind the Plan. B The development plan itself, include all relevant policies and objectives, and one or more maps - 1 - TINAHELY DRAFT TOWN PLAN PART A CONTENTS 1. Purpose of the plan…………………………………………………………….3 2. Local Area Plan status and process……………………………………………3 3. Public consultation……………………………………………………………4 4. Development management……………………………………………………6 5. Strategic Environmental Assessment…………………………………………6 6. Strategic context………………………………………………………………9 7. Population……………………………………………………………………10 8. Quantity of zoned land………………………………………………………10 Housing………………………………………………………………………11 Social & community infrastructure………………………………………….13 Employment & enterprise……………………………………………………15 Retail…………………………………………………………………………16 9. Infrastructure…………………………………………………………………17 - 2 - 1. PURPOSE OF THE PLAN It is the purpose of this Plan to establish a framework for the planned, co-ordinated and sustainable development of Tinahely. The aim of the Plan is to enhance and facilitate the balancing of economic, social and environmental infrastructure in order to maintain and develop a high quality of life without compromising the protection of the environment and the needs of future generations.