The Digestive System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

6 Physiology of the Colon : Motility
#6 Physiology of the colon : motility Objectives : ● Parts of the Colon ● Functions of the Colon ● The physiology of Different Colon Regions ● Secretion in the Colon ● Nutrient Digestion in the Colon ● Absorption in the Colon ● Bacterial Action in the Colon ● Motility in the Colon ● Defecation Reflex Doctors’ notes Extra Important Resources: 435 Boys’ & Girls’ slides | Guyton and Hall 12th & 13th edition Editing file [email protected] 1 ﺗﻛرار ﻣن اﻟﮭﺳﺗوﻟوﺟﻲ واﻷﻧﺎﺗوﻣﻲ The large intestine ● This is the final digestive structure. ● It does not contain villi. ● By the time the digested food (chyme) reaches the large intestine, most of the nutrients have been absorbed. ● The primary role of the large intestine is to convert chyme into feces for excretion. Parts of the colon ● The colon has a length of about 150 cm. ( 1.5 meters) (one-fifth of the whole length of GIT). ● It consists of the ascending & descending colon, transverse colon, sigmoid colon, rectum and anal canal. 3 ● The transit of radiolabeled chyme through 4 the large intestine occurs in 36-48 hrs. 2 They know this how? By inserting radioactive chyme. 1 6 5 ❖ Mucous membrane of the colon ● Lacks villi and has many crypts of lieberkuhn. ● They consists of simple short glands lined by mucous-secreting goblet cells. Main colonic secretion is mucous, as the colon lacks digestive enzymes. ● The outer longitudinal muscle layer is modified to form three longitudinal bands called taenia coli visible on the outer surface.(Taenia coli: Three thickened bands of muscles.) ● Since the muscle bands are shorter than the length of the colon, the colonic wall is sacculated and forms haustra.(Haustra: Sacculation of the colon between the taenia.) Guyton corner : mucus in the large intestine protects the intestinal wall against excoriation, but in addition, it provides an adherent medium for holding fecal matter together. -

Short Bowel Syndrome with Intestinal Failure Were Randomized to Teduglutide (0.05 Mg/Kg/Day) Or Placebo for 24 Weeks
Short Bowel (Gut) Syndrome LaTasha Henry February 25th, 2016 Learning Objectives • Define SBS • Normal function of small bowel • Clinical Manifestation and Diagnosis • Management • Updates Basic Definition • A malabsorption disorder caused by the surgical removal of the small intestine, or rarely it is due to the complete dysfunction of a large segment of bowel. • Most cases are acquired, although some children are born with a congenital short bowel. Intestinal Failure • SBS is the most common cause of intestinal failure, the state in which an individual’s GI function is inadequate to maintain his/her nutrient and hydration status w/o intravenous or enteral supplementation. • In addition to SBS, diseases or congenital defects that cause severe malabsorption, bowel obstruction, and dysmotility (eg, pseudo- obstruction) are causes of intestinal failure. Causes of SBS • surgical resection for Crohn’s disease • Malignancy • Radiation • vascular insufficiency • necrotizing enterocolitis (pediatric) • congenital intestinal anomalies such as atresias or gastroschisis (pediatric) Length as a Determinant of Intestinal Function • The length of the small intestine is an important determinant of intestinal function • Infant normal length is approximately 125 cm at the start of the third trimester of gestation and 250 cm at term • <75 cm are at risk for SBS • Adult normal length is approximately 400 cm • Adults with residual small intestine of less than 180 cm are at risk for developing SBS; those with less than 60 cm of small intestine (but with a -

Anatomy of the Digestive System
The Digestive System Anatomy of the Digestive System We need food for cellular utilization: organs of digestive system form essentially a long !nutrients as building blocks for synthesis continuous tube open at both ends !sugars, etc to break down for energy ! alimentary canal (gastrointestinal tract) most food that we eat cannot be directly used by the mouth!pharynx!esophagus!stomach! body small intestine!large intestine !too large and complex to be absorbed attached to this tube are assorted accessory organs and structures that aid in the digestive processes !chemical composition must be modified to be useable by cells salivary glands teeth digestive system functions to altered the chemical and liver physical composition of food so that it can be gall bladder absorbed and used by the body; ie pancreas mesenteries Functions of Digestive System: The GI tract (digestive system) is located mainly in 1. physical and chemical digestion abdominopelvic cavity 2. absorption surrounded by serous membrane = visceral peritoneum 3. collect & eliminate nonuseable components of food this serous membrane is continuous with parietal peritoneum and extends between digestive organs as mesenteries ! hold organs in place, prevent tangling Human Anatomy & Physiology: Digestive System; Ziser Lecture Notes, 2014.4 1 Human Anatomy & Physiology: Digestive System; Ziser Lecture Notes, 2014.4 2 is suspended from rear of soft palate The wall of the alimentary canal consists of 4 layers: blocks nasal passages when swallowing outer serosa: tongue visceral peritoneum, -
The Gastrointestinal System & Digestion Visual Worksheet
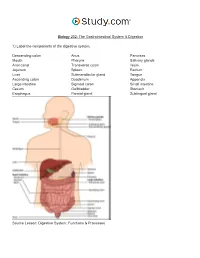
Biology 202: The Gastrointestinal System & Digestion 1) Label the components of the digestive system. Descending colon Anus Pancreas Mouth Pharynx Salivary glands Anal canal Transverse colon Ileum Jejunum Spleen Rectum Liver Submandibular gland Tongue Ascending colon Duodenum Appendix Large intestine Sigmoid colon Small intestine Cecum Gallbladder Stomach Esophagus Parotid gland Sublingual gland Source Lesson: Digestive System: Functions & Processes 2) Label the image below. Serosa Submucous plexus Muscularis externa Submucosa Myenteric plexus Muscular interna Source Lesson: Role of the Enteric Nervous System in Digestion 3) Label the structures of the alimentary canal. Some terms may be used more than once. Vein Mesentery Mucosa Submucosal plexus Epithelium Gland in mucosa Nerve Muscularis Serosa Lymphatic tissue Muscularis mucosae Glands in submucosa Lamina propria Submucosa Duct of gland outside tract Gland in mucosa Lumen Artery Longitudinal muscle Musculararis Areolar connective tissue Circular muscle Myenteric plexus Source Lesson: The Upper Alimentary Canal: Key Structures, Digestive Processes & Food Propulsion 4) Label the image below. Stomach Trachea Lower esophageal sphincter Esophagus Upper esophageal sphincter Source Lesson: The Upper Alimentary Canal: Key Structures, Digestive Processes & Food Propulsion 5) Label the anatomy of the oral cavity. Upper lip Tonsil Inferior labial frenulum Floor of mouth Tongue Superior labial frenulum Lower lip Teeth Retromolar trigone Palatine arch Hard palate Uvula Glossopalatine arch Soft palate Gingiva Source Lesson: The Oral Cavity: Structures & Functions 6) Label the structures of the oral cavity. Some terms may be used more than once. Hard palate Oropharynx Soft palate Pharyngeal tonsil Oral cavity Lingual tonsil Superior lip Teeth Palatine tonsil Tongue Inferior lip Source Lesson: The Oral Cavity: Structures & Functions 7) Label the image below. -

Internal Anal Sphincter
Arch Dis Child: first published as 10.1136/adc.43.231.569 on 1 October 1968. Downloaded from Arch. Dis. Childh., 1968, 43, 569. Internal Anal Sphincter Observations on Development and Mechanism of Inhibitory Responses in Premature Infants and Children with Hirschsprung's Disease E. R. HOWARD and H. H. NIXON From The Hospitalfor Sick Children, Great Ormond Street, London W.C.1 The relative importance of the internal and obstruction to constipation alone. During this external sphincters to the maintenance of tone in study physiological abnormalities were observed in the anal canal has been shown in previous studies of the reflexes of premature infants, which showed anal physiology (Gaston, 1948; Schuster et al., 1965; similarities to those seen in patients with Hirsch- Duthie and Watts, 1965). sprung's disease. On repeated examinations over The external sphincter is a striated muscle, but several days, however, the physiological responses shows continuous activity on electromyography. were found to change until normal reflexes were Inhibition and stimulation is mediated by spinal eventually established. cord reflexes, through the pudendal nerves and In order to help determine the nervous pathway sacral segments of the spinal cord (Floyd and Walls, through which the reflexes of the internal sphincter copyright. 1953; Porter, 1961). Voluntary control is possible are mediated, we have examined normal bowel over this part ofthe anal sphincter. and aganglionic bowel from cases of Hirschsprung's The internal sphincter is made up of smooth disease by pharmacological and histochemical muscle fibres, continuous with the muscle layers of methods. the rectal wall, and under resting conditions pro- vides most of the tone of the anal canal (Duthie and Physiological Study Watts, 1965). -

Aandp2ch25lecture.Pdf
Chapter 25 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction • Most nutrients we eat cannot be used in existing form – Must be broken down into smaller components before body can make use of them • Digestive system—acts as a disassembly line – To break down nutrients into forms that can be used by the body – To absorb them so they can be distributed to the tissues • Gastroenterology—the study of the digestive tract and the diagnosis and treatment of its disorders 25-2 General Anatomy and Digestive Processes • Expected Learning Outcomes – List the functions and major physiological processes of the digestive system. – Distinguish between mechanical and chemical digestion. – Describe the basic chemical process underlying all chemical digestion, and name the major substrates and products of this process. 25-3 General Anatomy and Digestive Processes (Continued) – List the regions of the digestive tract and the accessory organs of the digestive system. – Identify the layers of the digestive tract and describe its relationship to the peritoneum. – Describe the general neural and chemical controls over digestive function. 25-4 Digestive Function • Digestive system—organ system that processes food, extracts nutrients, and eliminates residue • Five stages of digestion – Ingestion: selective intake of food – Digestion: mechanical and chemical breakdown of food into a form usable by -

Electrophysiological Studies the Antrum Muscle Fibers of the Guinea
Electrophysiological Studies of the Antrum Muscle Fibers of the Guinea Pig Stomach H. KURIYAMA, T. OSA, and H. TASAKI Downloaded from http://rupress.org/jgp/article-pdf/55/1/48/1244765/48.pdf by guest on 29 September 2021 From the Department of PhysiologT,Faculty of Medicine and Dentistry, Kyushu University, Fukuoka,Japan AB STRAC T The membrane potentials of single smooth muscle fibers of various regions of the stomach were measured, and do not differ from those measured in intestinal muscle. Spontaneous slow waves with superimposed spikes could be recorded from the longitudinal and circular muscle of the antrum. The develop- ment of tension was preceded by spikes but often tension appeared only when the slow waves were generated. Contracture in high K solution developed at a critical membrane potential of --42 my. MnCI~ blocked the spike generation, then lowered the amplitude of the slow wave. On the other hand, withdrawal of Na +, or addition of atropine and tetrodotoxin inhibited the generation of most of the slow waves but a spike could still be elicited by electrical stimula- tion. Prostigmine enhanced and prolonged the slow wave; acetylcholine de- polarized the membrane without change in the frequency of the slow waves. Chronaxie for the spike generation in the longitudinal muscle of the antrum was 30 msec and conduction velocity was 1.2 cm/sec. The time constant of the foot of the propagated spike was 28 reset. The space constants measured from the longitudinal and circular muscles of the antrum were 1.1 mm and 1.4 into, respectively. INTRODUCTION The early investigations of mammalian stomach muscle suggested that mem- brane activity consisted of spike and slow wave components (Alvarez and Mahoney, 1922; Richter, 1923; Bozler, 1938, 1942; and Ichikawa and Bozler, 1955; Daniel, 1965). -
Bacteria Slides
BACTERIA SLIDES Cocci Bacillus BACTERIA SLIDES _______________ __ BACTERIA SLIDES Spirilla BACTERIA SLIDES ___________________ _____ BACTERIA SLIDES Bacillus BACTERIA SLIDES ________________ _ LUNG SLIDE Bronchiole Lumen Alveolar Sac Alveoli Alveolar Duct LUNG SLIDE SAGITTAL SECTION OF HUMAN HEAD MODEL Superior Concha Auditory Tube Middle Concha Opening Inferior Concha Nasal Cavity Internal Nare External Nare Hard Palate Pharyngeal Oral Cavity Tonsils Tongue Nasopharynx Soft Palate Oropharynx Uvula Laryngopharynx Palatine Tonsils Lingual Tonsils Epiglottis False Vocal Cords True Vocal Cords Esophagus Thyroid Cartilage Trachea Cricoid Cartilage SAGITTAL SECTION OF HUMAN HEAD MODEL LARYNX MODEL Side View Anterior View Hyoid Bone Superior Horn Thyroid Cartilage Inferior Horn Thyroid Gland Cricoid Cartilage Trachea Tracheal Rings LARYNX MODEL Posterior View Epiglottis Hyoid Bone Vocal Cords Epiglottis Corniculate Cartilage Arytenoid Cartilage Cricoid Cartilage Thyroid Gland Parathyroid Glands LARYNX MODEL Side View Anterior View ____________ _ ____________ _______ ______________ _____ _____________ ____________________ _____ ______________ _____ _________ _________ ____________ _______ LARYNX MODEL Posterior View HUMAN HEART & LUNGS MODEL Larynx Tracheal Rings Found on the Trachea Left Superior Lobe Left Inferior Lobe Heart Right Superior Lobe Right Middle Lobe Right Inferior Lobe Diaphragm HUMAN HEART & LUNGS MODEL Hilum (curvature where blood vessels enter lungs) Carina Pulmonary Arteries (Blue) Pulmonary Veins (Red) Bronchioles Apex (points -

Gastrointestinal Motility, Part 2: Small-Bowel and Colon Transit
CONTINUING EDUCATION Gastrointestinal Motility, Part 2: Small-Bowel and Colon Transit Alan H. Maurer Nuclear Medicine and Molecular Imaging, Temple University Hospital and School of Medicine, Philadelphia, Pennsylvania Learning Objectives: On successful completion of this activity, participants should be able to describe (1) the normal physiology and pathophysiology of small-bowel and colon transit; (2) methods for performing scintigraphic small-bowel and colon transit studies; and (3) pertinent image findings for interpreting scintigraphic small-bowel and colon transit studies. Financial Disclosure: The author of this article has indicated no relevant relationships that could be perceived as a real or apparent conflict of interest. CME Credit: SNMMI is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing education for physicians. SNMMI designates each JNM continuing education article for a maximum of 2.0 AMA PRA Category 1 Credits. Physicians should claim only credit commensurate with the extent of their participation in the activity. For CE credit, SAM, and other credit types, participants can access this activity through the SNMMI website (http://www.snmmilearningcenter.org) through September 2018. and indigestible solids. It is recommended that gastrointestinal Because of the difficulty often encountered in deciding whether transit studies be used to localize the potential site of disease a patient’s symptoms originate in the upper or lower gastrointesti- and guide therapy (2). A final diagnosis of a primary motility nal tract, gastrointestinal transit scintigraphy is a uniquely suited disorder by scintigraphy should not be made until an anatomic noninvasive, quantitative, and physiologic method of determining or structural cause (e.g., tumor, stricture, malrotation) for abnor- whether there is a motility disorder affecting the stomach, small mal transit has been excluded by imaging or endoscopy. -

Morphology of the Gastrointestinal Tract in Primates : Comparisons with Other Mammals in Relation to Diet David J Chivers, Claude Marcel Hladik
Morphology of the gastrointestinal tract in primates : Comparisons with other mammals in relation to diet David J Chivers, Claude Marcel Hladik To cite this version: David J Chivers, Claude Marcel Hladik. Morphology of the gastrointestinal tract in primates : Com- parisons with other mammals in relation to diet. Journal of Morphology, Wiley, 1980, 166, pp.337-386. hal-00561758 HAL Id: hal-00561758 https://hal.archives-ouvertes.fr/hal-00561758 Submitted on 16 Mar 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. CHIVERS D.J. & HLADIK C.M. (1980) — Morphology of the gastrointestinal tract in primates : Comparisons with other mammals in relation to diet. Journal of Morphology, 166 : 337-386. Flattened pieces of intestinal tract in a dissecting tray, for the actual measurement of mucosal area. 338 DAVID J. CliiVERS AND C. M. HLADIK G 'I' ~IOI!PIIOI.OGY Ai\llDIET I ~li\~ 1\ I AI.S 339 '67) showed interesting relationsh ips among available in limited qua ntity (fruit), to t hose reductions are clearly specializations, rather a "muscular tooth" compensating fo r the lack primates, but data on diet were st ill inade that are widely abundant bui relatively diffi than representing the prim it ive condition. -

Digestive System A&P DHO 7.11 Digestive System
Digestive System A&P DHO 7.11 Digestive System AKA gastrointestinal system or GI system Function=responsible for the physical & chemical breakdown of food (digestion) so it can be taken into bloodstream & be used by body cells & tissues (absorption) Structures=divided into alimentary canal & accessory organs Alimentary Canal Long muscular tube Includes: 1. Mouth 2. Pharynx 3. Esophagus 4. Stomach 5. Small intestine 6. Large intestine 1. Mouth Mouth=buccal cavity Where food enters body, is tasted, broken down physically by teeth, lubricated & partially digested by saliva, & swallowed Teeth=structures that physically break down food by chewing & grinding in a process called mastication 1. Mouth Tongue=muscular organ, contains taste buds which allow for sweet, salty, sour, bitter, and umami (meaty or savory) sensations Tongue also aids in chewing & swallowing 1. Mouth Hard palate=bony structure, forms roof of mouth, separates mouth from nasal cavities Soft palate=behind hard palate; separates mouth from nasopharynx Uvula=cone-shaped muscular structure, hangs from middle of soft palate; prevents food from entering nasopharynx during swallowing 1. Mouth Salivary glands=3 pairs (parotid, sublingual, & submandibular); produce saliva Saliva=liquid that lubricates mouth during speech & chewing, moistens food so it can be swallowed Salivary amylase=saliva enzyme (substance that speeds up a chemical reaction) starts the chemical breakdown of carbohydrates (starches) into sugar 2. Pharynx Bolus=chewed food mixed with saliva Pharynx=throat; tube that carries air & food Air goes to trachea; food goes to esophagus When bolus is swallowed, epiglottis covers larynx which stops bolus from entering respiratory tract and makes it go into esophagus 3. -

Axis Scientific Human Digestive System (1/2 Size)
Axis Scientific Human Digestive System (1/2 Size) A-105865 48. Body of Pancreas 27. Transverse Colon 02. Hard Palate 47. Pancreatic Notch 07. Nasopharynx 05. Tooth 01. Lower Lip F. Large Intestine 06. Tongue 21. Jejunum A. Oral Cavity 09. Pharyngeal Tonsil 03. Soft Palate 08. Opening to Auditory Tube 28. E. Small Intestine 04. Uvula 11. Palatine Tonsil Descending Colon 40. Gallbladder 37. Round Ligament of Liver 22. Ileum 38. Quadrate Lobe 44. Proper Hepatic Artery 42. Common Hepatic Duct 45. Hepatic Portal Vein C. Esophagus 15. Fundus of Stomach 30. Rectum 29. Sigmoid Colon 13. Cardia 26. Ascending Colon 39. Caudate Lobe 24. Ileocecal Valve 35. Left Lobe of 16. Body of 34. Falciform Liver Stomach 41. Cystic Duct Ligament 36. Right Lobe of Liver G. Liver 31. Anal Canal 14. Pylorus D. Stomach 33. External 18. Duodenum Anal Sphincter Muscle 17. Pyloric Antrum 46. Head of Pancreas 23. Cecum 51. Accessory Pancreatic Duct 49. Tail of 50. Pancreatic 25. Vermiform 20. Minor Duodenal Papilla H. Pancreas Duct Pancreas Appendix 19. Major Duodenal Papilla 32. Internal Anal Sphincter Muscle 01. Lower Lip 20. Minor Duodenal Papilla 39. Caudate Lobe 02. Hard Palate 21. Jejunum 40. Gallbladder 03. Soft Palate 22. Ileum 41. Cystic Duct 42. Common Hepatic Duct 04. Uvula 23. Cecum 43. Common Bile Duct 05. Tooth 24. Ileocecal Valve 44. Proper Hepatic Artery 06. Tongue 25. Vermiform Appendix 45. Hepatic Portal Vein 07. Nasopharynx 26. Ascending Colon 46. Head of Pancreas 08. Opening to Auditory Tube 27. Transverse Colon 47. Pancreatic Notch 09. Pharyngeal Tonsil 28.