CDI Report for Major Problems in Africa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Discussion Piece Reflecting on the Recent Implementation of Programmes and Policies Supported by the World Bank in Benin, Camero
COMMUNITY-BASED RESULTS-BASED FINANCING IN HEALTH IN PRACTICE. A discussion piece reflecting on the recent implementation of programmes and policies supported by the World Bank in Benin, Cameroon, the Republic of Congo, the Democratic Republic of the Congo, The Gambia, and Rwanda Jean-Benoît Falisse, Petra Vergeer, Maud Juquois, Alphonse Akpamoli, Jacob Paul Robyn, Walters Shu, Michel Zabiti, Rifat Hasan, Bakary Jallow, Musa Loum, Cédric Ndizeye, Michel Muvudi, Baudouin Makuma Booto Joy Gebre Medhin Executive summary This report discusses Community Results-Based Financing (cRBF), a 'close to client' approach whereby community actors are paid based on the activities they undertake. The focus is on six developing cRBF experiences that have started in Cameroon, The Gambia, Benin, the Democratic Republic of the Congo (DR Congo), Rwanda, and the Republic of Congo. The report's main aim is to cast light on the success and difficulties encountered in the implementation of such a programme. The report is based on a participative process that included a short review of the existing literature on cRBF, a review of the manuals of procedures and reports produced in each country case, in-depth interviews with a focal point in five countries, and two workshops with practitioners. Do cRBF schemes work? It is too early to say: most schemes are still in their infancy. An impact evaluation of the Rwandan scheme found mixed effects. The Cameroon, Congo, and the Gambia schemes integrate rigorous impact evaluation mechanisms and the first results should be available in two to five years. At this stage, the main discussion is on the implementation of cRBF. -

Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields
Masks on the Move Defying Genres, Styles, and Traditions in the Cameroonian Grassfields Silvia Forni n the realm of African art, masks are some of the most This article investigates the longstanding history of commer- exemplary and iconic artworks. Whether displayed cial practices and stylistic experimentation that characterize to be admired for their shape, form, and volumes, or the production of masks and other artworks in the Grassfields presented in dialogue with ethnographic information of Western Cameroon. While I acknowledge the importance of and contextual images, masks are omnipresent in col- long-distance and international trade as an important stimulus lections and displays of African art. As aesthetic and for creativity and artistic production, my intention is to high- ethnographic objects, masks are used as gateways to the under- light the significance of contemporary artistic inventions in Istanding and appreciation of “cultural styles” as well as the for- shaping local understanding of aesthetics and material displays. mal and creative solutions adopted by artists and workshops. Yet Collections, museums, eco-museological itineraries and, more the appeal of masks also relies on their perceived irreducible dif- recently, experimentations and artistic interventions by contem- ference and mysterious spiritual aura. Even when isolated and porary artists Hervé Youmbi and Hervé Yamguen (Fig. 1) have stripped of their fiber costumes and attachments, there is always produced a complex and intriguing regional and national artistic a reference to the body of an absent wearer, thus evoking a sit- scene. Here the taxonomies distinguishing commercial produc- uated and embodied history of production, performance, and tions from “authentic artworks” have been blurred and subverted social meaning that often does not accompany the mask into the in local practices, where masks are now moving between spheres museum. -

WHO in Cameroon
Summary : Pages List of abbreviations 3 Editorial 5 7 Highlights of 2016 6 Significant quotes in 2016 8 Figures , charts and tables 9 Introduction 10 1. Communicable Diseases 12 1.1. HIV / AIDS 1.2. TUBERCULOSIS 14 1.3. MALARIA 1.4. NEGLECTED TROPICAL DISEASES 15 1.5. VACCINE PREVENTABLE DISEASES 19 6 2. Noncommunicable Diseases 24 2.1. NONCOMMUNICABLE DISEASES 2.2. NUTRITION 25 3. Promoting health at all stages of life 25 3.1. REPRODUCTIVE, MATERNAL, NEWBORN, CHILD AND ADOLESCENT HEALTH. 4. Health Systems 31 4.1. NATIONAL HEALTH POLICIES, STRATEGIES AND PLANS 4.2. ACCESS TO DRUGS AND HEALTH TECHNOLOGIES, AND STRENGTHENING REGULATORY MEASURES 4.3. INFORMATION AND DATA ON HEALTH SYSTEMS 32 5. Preparedness, monitoring and response 33 5.1. ALERT AND INTERVENTION CAPACITIES 5.2. MANAGEMENT OF CRISES AND RISKS ASSOCIATED WITH EMERGENCIES 35 5.3. POLIOMYELITIS ERADICATION 36 6. Institutional and Support Services 42 6.1. PROGRAMME SUPPORT (COUNTRY SUPPORT UNIT) 6.2. HUMAN RESOURCES 43 6.3. FINANCIAL MANAGEMENT AND INTERNAL CONTROL 6.4. IMPROVEMENT OF THE WORKING ENVIRONMENT 45 6.5. INFORMATION AND COMMUNICATION TECHNOLOGIES 14 6.6. COMMUNICATION SUPPORT PROGRAMMES 46 >> The faces of the office 47 - 50 ANNEX 51 Acknowledgements Annex 1 : Obstacles and constraints 52 Throughout the year, we worked with the Lessons learned Ministry of Public Health, the Government Prospects for the year 2017 53 of Cameroon, numerous bilateral and Annex 2 : Support received from IST – AFRO - HQ 54 multilateral partners, governmental orga - nizations and the civil society. Annex 3 : Assistance Missions to the Country We therefore express to them our deepest Annex 4 : List of documents produced 55 appreciation. -

Modele-Mc2-Depliant.Pdf
Pourqoui les MC² • La pauvreté est essentiellement rurale (plus de 60% de la population) ; • Plus de 50% des pauvres (personnes vivant avec moins d’un dollar par jour) vivent en Afrique • Les populations rurales n’ont presque pas accès aux services financiers qui permettraient d’améliorer leurs conditions de vie et développer leur communauté. Le grenier de la communauté • Les zones rurales regorgent d’un grand potentiel en ressources naturelles, agropastorales, etc. encore très peu valorisées Le bien-être de la famille par la femme Listes des MC² opérationnelles au cameroun au 31 octobre 2018 1. MC² de Baham 25. MC² Fongo-Tongo 49. MC² de Baré 73. MC² de Fundong 97. MC² de Mindif 2. MC² de Manjo 26. MC² de Njombé 50. MC² de Bertoua 74. MC² de Tibati 98. MC² Bamenkombo 3. MC² de Melong 27. MC² de Mbankomo 51. MC² de Banyo 75. MC² de Mbang 99. MC² Kedjom Keku 4. MC² Penka-Michel 28. MC² Kribi- Campo 52. MC² de Mokolo 76. MC² de Belo 100. MC² de Ngong 5. MC² de Bandjoun 29. MC² de Loum 53. MC² de Makak 77. MC² de Okola 101. MC² de Bangoua Le modèle MC² 6. MC² de Badjouma 30. MC² Esse-Awae 2 54. MC² de Bangang 78. MC² Tongo Gandima 102. MC² de Tonga 7. MC² de Bafia 31. MC² de Ekondo Titi 55. MC² de Santa 79. MC² Abong-Mbang 103. MC² de Ngoro Une approche endogène 8. MC² de Bamendjou 32. MC² de Kekem 56. MC² de Bamena 80. MC² de Yabassi 104. MC² de Ndziih 9. -

Banking on Health: World Bank and African Development Bank Spending on Reproductive Health And
Banking on Health: World Bank and African Development Bank Spending on Reproductive Health and HIV/AIDS in Sub-Saharan Africa i Publication prepared by: Claire Lauterbach, Programs Associate, Gender Action With contributions from: Elaine Zuckerman, President, Gender Action Elizabeth Arend, former Programs Coordinator, Gender Action Patience Nyangoma, Executive Director, NAWAD Christian Tanyi, Chief Executive Officer, LUKMEF With support from: The William and Flora Hewlett Foundation The Tides Foundation Copyright © Gender Action 2012 About Gender Action Gender Action was established in 2002. It is the only organization dedicated to promoting gender justice and women’s rights in all International Financial Institution (IFI) investments such as those of the World Bank. Gender Action’s goal is to ensure that women and men equally participate in and benefit from all IFI investments. Gender Action 1875 Connecticut Avenue NW Suite 500 Washington DC 20009, USA Tel: 202 939 5463 Email: [email protected] http://www.genderaction.org ii Table of Contents List of Abbreviations .................................................................................................................................... iv Executive Summary....................................................................................................................................... v Introduction ..................................................................................................................................................1 Population and reproductive -

Skeeling 1.Pdf
Musicking Tradition in Place: Participation, Values, and Banks in Bamiléké Territory by Simon Robert Jo-Keeling A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Anthropology) in The University of Michigan 2011 Doctoral Committee: Professor Judith T. Irvine, Chair Emeritus Professor Judith O. Becker Professor Bruce Mannheim Associate Professor Kelly M. Askew © Simon Robert Jo-Keeling, 2011 acknowledgements Most of all, my thanks go to those residents of Cameroon who assisted with or parti- cipated in my research, especially Theophile Ematchoua, Theophile Issola Missé, Moise Kamndjo, Valerie Kamta, Majolie Kwamu Wandji, Josiane Mbakob, Georges Ngandjou, Antoine Ngoyou Tchouta, Francois Nkwilang, Epiphanie Nya, Basil, Brenda, Elizabeth, Julienne, Majolie, Moise, Pierre, Raisa, Rita, Tresor, Yonga, Le Comité d’Etudes et de la Production des Oeuvres Mèdûmbà and the real-life Association de Benskin and Associa- tion de Mangambeu. Most of all Cameroonians, I thank Emanuel Kamadjou, Alain Kamtchoua, Jules Tankeu and Elise, and Joseph Wansi Eyoumbi. I am grateful to the Wenner-Gren Foundation for Anthropological Research for fund- ing my field work. For support, guidance, inspiration, encouragement, and mentoring, I thank the mem- bers of my dissertation committee, Kelly Askew, Judith Becker, Judith Irvine, and Bruce Mannheim. The three members from the anthropology department supported me the whole way through my graduate training. I am especially grateful to my superb advisor, Judith Irvine, who worked very closely and skillfully with me, particularly during field work and writing up. Other people affiliated with the department of anthropology at the University of Michigan were especially helpful or supportive in a variety of ways. -

Forets Sacres Au Cameroun.Pdf
M.E.M Millennium Ecologic Museum Ministère des Forêts et de la Faune Inventaire, cartographie et étude diagnostic des forêts sacrées du Cameroun : contribution à l’élaboration d’une stratégie nationale de gestion durable RAPPORT FINAL D’EXECUTION Avec l’appui financier du Programme CARPE-IUCN Juin 2010 0 Millennium Ecologic Museum MEM BP : 8038 Yaoundé, Cameroun Tel : (237) 99 99 54 08 / 96 68 11 34 e-mail : [email protected] Site web: www.ecologicalmuseum.netsons.org 1 L’EQUIPE DU PROJET Conseiller Technique Principal Prof. Bernard-Aloys NKONGMENECK, Directeur du MEM Point Focal MINFOF M. NOBANZA Francis, MINFOF/SDIAF - Service Cartographie Conseillers Scientifiques Guy Merlin NGUENANG Vincent BELIGNE Coordination des activités terrain et rapportage Evariste FONGNZOSSIE Collecte des données Victor Aimé KEMEUZE et René Bernadin JIOFACK Assistés de : JOHNSON Madeleine MAKEMTEU Junelle KAMDEM Gyslène WONKAM Christelle TABI Paule Pamela TAJEUKEM Vice Clotex MVETUMBO Moise KENNE Florette Base de Données et GIS Victor KEMEUZE et Francis NOBANZA 2 SOMMAIRE DU RAPPORT LISTE DES ACRONYMES....................................................................................................................................... 6 LISTE DES FIGURES .............................................................................................................................................. 7 LISTE DES TABLEAUX ......................................................................................................................................... -
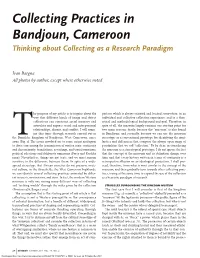
Collecting Practices in Bandjoun, Cameroon Thinking About Collecting As a Research Paradigm
Collecting Practices in Bandjoun, Cameroon Thinking about Collecting as a Research Paradigm Ivan Bargna All photos by author, except where otherwise noted he purpose of my article is to inquire about the parison which is always oriented and located somewhere, in an way that different kinds of image and object individual and collective collection experience, and in a theo- collections can construct social memory and retical and methodological background and goal. Therefore, in articulate and express social and interpersonal spite of all, the museum largely remains our starting point for relationships, dissent, and conflict. I will exam- two main reasons: firstly, because the “museum” is also found ine this topic through research carried out in in Bandjoun; and secondly, because we can use the museum the Bamileke kingdom of Bandjoun, West Cameroon, since stereotype as a conventional prototype for identifying the simi- T2002 (Fig. 1). The issues involved are to some extent analogous larities and differences that compose the always open range of to those concerning the transmission of written texts: continuity possibilities that we call “collection.” To be clear, in considering and discontinuity; translations, rewritings, and transformations; the museum as a stereotypical prototype, I do not ignore the fact political selections and deliberate omissions (Forty and Kuchler that the concept of the museum and its definition change over 1999). Nevertheless, things are not texts, and we must remain time and that every history written in terms of -

African Development Bank Group
AFRICAN DEVELOPMENT BANK GROUP PROJECT : TRANSPORT SECTOR SUPPORT PROGRAMME PHASE 2 : REHABILITATION OF YAOUNDE-BAFOUSSAM- BAMENDA ROAD – DEVELOPMENT OF THE GRAND ZAMBI-KRIBI ROAD – DEVELOPMENT OF THE MAROUA-BOGO-POUSS ROAD COUNTRY : REPUBLIC OF CAMEROON SUMMARY FULL RESETTLEMENT PLAN (FRP) Team Leader J. K. NGUESSAN, Chief Transport Engineer OITC.1 P. MEGNE, Transport Economist OITC.1 P.H. SANON, Socio-Economist ONEC.3 M. KINANE, Environmentalist ONEC.3 S. MBA, Senior Transport Engineer OITC.1 T. DIALLO, Financial Management Expert ORPF.2 C. DJEUFO, Procurement Specialist ORPF.1 Appraisal Team O. Cheick SID, Consultant OITC.1 Sector Director A. OUMAROU OITC Regional Director M. KANGA ORCE Resident CMFO R. KANE Representative Sector Division OITC.1 J.K. KABANGUKA Manager 1 Project Name : Transport Sector Support Programme Phase 2 SAP Code: P-CM-DB0-015 Country : Cameroon Department : OITC Division : OITC-1 1. INTRODUCTION This document is a summary of the Abbreviated Resettlement Plan (ARP) of the Transport Sector Support Programme Phase 2. The ARP was prepared in accordance with AfDB requirements as the project will affect less than 200 people. It is an annex to the Yaounde- Bafoussam-Babadjou road section ESIA summary which was prepared in accordance with AfDB’s and Cameroon’s environmental and social assessment guidelines and procedures for Category 1 projects. 2. PROJECT DESCRIPTION, LOCATION AND IMPACT AREA 2.1.1 Location The Yaounde-Bafoussam-Bamenda road covers National Road 4 (RN4) and sections of National Road 1 (RN1) and National Road 6 (RN6) (Figure 1). The section to be rehabilitated is 238 kilometres long. Figure 1: Project Location Source: NCP (2015) 2 2.2 Project Description and Rationale The Yaounde-Bafoussam-Bamenda (RN1-RN4-RN6) road, which was commissioned in the 1980s, is in an advanced state of degradation (except for a few recently paved sections between Yaounde and Ebebda, Tonga and Banganté and Bafoussam-Mbouda-Babadjou). -

Divine Illumination: the Unity Of
Ilorin Journal of Religious Studies (IJOURELS) Vol. 2, No. 2 (2012) pp.61-72 THE RELIGIOUS DIVIDE IN THE YORUBA TERMINOLOGY FOR GOD: A LINGUISTIC PERSPECTIVE Michael A.O. Oyebola Department of Linguistics and Nigerian Languages, University of Ilorin, Ilorin. [email protected] [email protected] Abstract This paper has addressed the issue of the reflection of religious affiliation in the use of language. It specifically set out to ascertain whether the use any of the Ọlọ́ run/ Ọlọ́ hun variant, in reference to ‘God’ has any religious connotation. In addition it sought to find out which of the variants correctly serves as the underlying form of the reduced form ‘Ọlọ́ un’. The paper adopted a two-pronged methodological approach, first, through a phonological analysis of consonant deletion in Yoruba, and secondly, through a questionnaire based data collection. The phonological analysis focused specifically on the possibility of the deletion of [r] and [h] in Yoruba. The linguistic analysis showed that the reduced form could not have been derived from the variant with [r] but from that with [h]. The analysis from the results from the questionnaire showed that though the Ọlọ́ run variant is predominant in the language community, the Muslim origin of the Ọlọ́ hun variant is not in doubt. The study found that Christians and Muslims use the reduced variant without regard to its decidedly Muslim origin. The paper concluded by observing that linguistics and language use are veritable instruments of breaking down the barriers of religious divide. Introduction The Yoruba language community is, within the larger Nigerian context, remarkable for peaceful coexistence in religious pluralism. -

Dekadal Climate Alerts and Probable Impacts for the Period 21St to 30Th October 2020
REPUBLIQUE DU CAMEROUN REPUBLIC OF CAMEROON Paix-Travail-Patrie Peace-Work-Fatherland ----------- ----------- OBSERVATOIRE NATIONAL SUR NATIONAL OBSERVATORY LES CHANGEMENTS CLIMATIQUES ON CLIMATE CHANGE ----------------- ----------------- DIRECTION GENERALE DIRECTORATE GENERAL ----------------- ----------------- ONACC www.onacc.cm; [email protected]; Tel : (+237) 693 370 504 / 654 392 529 BULLETIN N° 60 Dekadal climate alerts and probable impacts for the period 21st to 30th October 2020 st 21 October 2020 © NOCC October 2020, all rights reserved Supervision Prof. Dr. Eng. AMOUGOU Joseph Armathé, Director, National Observatory on Climate Change (NOCC) and Lecturer in the Department of Geography at the University of Yaounde I, Cameroon. Eng. FORGHAB Patrick MBOMBA, Deputy Director, National Observatory on Climate Change (NOCC). Production Team (NOCC) Prof. Dr. Eng. AMOUGOU Joseph Armathé, Director, National Observatory on Climate Change (NOCC) and Lecturer in the Department of Geography at the University of Yaounde I, Cameroon. Eng. FORGHAB Patrick MBOMBA, Deputy Director, National Observatory on Climate Change (NOCC). BATHA Romain Armand Soleil, PhD student and Technical staff, NOCC. ZOUH TEM Isabella, M.Sc. in GIS-Environment and Technical staff, NOCC. NDJELA MBEIH Gaston Evarice, M.Sc. in Economics and Environmental Management. MEYONG René Ramsès, M.Sc. in Physical Geography (Climatology/Biogeography). ANYE Victorine Ambo, Administrative staff, NOCC. ELONG Julien Aymar, M.Sc. in Business and Environmental law. I. Introduction This dekadal -
Topics on Yoruba Nominal Expressions
TOPICS ON YORUBA NOMINAL EXPRESSIONS by OLADIIPO JACOB AJIBOYE B.A (1983), P.G.D.E (1988), MA (1992), University of florin A THESIS SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY in THE FACULTY OF GRADUATE STUDIES (Linguistics) THE UNIVERISTY OF BRITISH COLUMBIA November 2005 © Oladiipo Jacob Ajiboye, 2005 ABSTRACT This thesis discusses four selected topics on Yoruba nominal expressions: the syntax of possessives, the construal of bare nouns, the marking of specificity and salience, and plural marking strategies. Regarding possessives, it is proposed that they have one base structure (a vP shell). The difference in surface linear order between verbal and nominal genitives is determined by which of the two arguments move. In nominal genitives, the possessum moves. In verbal genitives, it is the possessor that moves. Regarding the interpretation of Yoruba bare nouns, it is shown that they can be construed in one of three ways: as generics, as indefinites, or as definites. First, generics may be lexically conditioned (with permanent state predicates) or grammatically conditioned (with transitory predicates through the use of imperfective maa-n). Second, wherever a generic construal is illicit, an indefinite construal is licit. Third, definite construals are discourse-linked. Regarding specificity, it is shown that Yoruba overtly marks specificity on NPs with the element kan. Regarding salience, it is shown that definite DPs are morphologically marked as salient (by virtue of being unique, in an identity relation or additive) through the use of nda. Finally, regarding plural marking, it is shown that Yoruba uses three different strategies: contextually, semantically, or morphologically determined plurality.