CUDAHY-DISSERTATION-2015.Pdf (1.179Mb)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

John G. Diefenbaker: the Political Apprenticeship Of
JOHN G. DIEFENBAKER: THE POLITICAL APPRENTICESHIP OF A SASKATCHEWAN POLITICIAN, 1925-1940 A Thesis Submitted to the Faculty of Graduate Studies and Research in Partial Fulfilment of the Requirements for the Degree of Master of Arts in the Department of History University of Saskatchewan Saskatoon by Methodius R. Diakow March, 1995 @Copyright Methodius R. Diakow, 1995. All rights reserved. In presenting this thesis in partial fulfilment of the requirements for a Postgraduate degree from the University of Saskatchewan, I agree that the Libraries of this University may make it freely available for inspection. I further agree that permission for copying of this thesis in any manner, in whole or in part, for scholarly purposes may be granted by the professor or professors who supervised my thesis work or, in their absence, by the Head of the Department for the Dean of the College in which my thesis work was done. It is understood that any copying or pUblication or use of this thesis or parts thereof for financial gain shall not be allowed without my written permission. It is also understood that due recognition shall be given to me and to the University of Saskatchewan in any scholarly use which may be made of any material in my thesis. Requests for permission to copy or to make other use of material in this thesis in whole or part should be addressed to: Head of the Department of History University of Saskatchewan 9 Campus Drive Saskatoon, Saskatchewan S7N 5A5 ii ABSTRACT John G. Diefenbaker is most often described by historians and biographers as a successful and popular politician. -
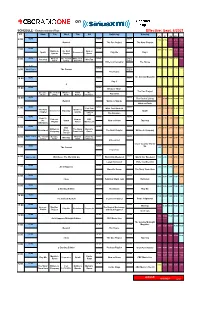
Siriusxm-Schedule.Pdf
on SCHEDULE - Eastern Standard Time - Effective: Sept. 6/2021 ET Mon Tue Wed Thu Fri Saturday Sunday ATL ET CEN MTN PAC NEWS NEWS NEWS 6:00 7:00 6:00 5:00 4:00 3:00 Rewind The Doc Project The Next Chapter NEWS NEWS NEWS 7:00 8:00 7:00 6:00 5:00 4:00 Quirks & The Next Now or Spark Unreserved Play Me Day 6 Quarks Chapter Never NEWS What on The Cost of White Coat NEWS World 9:00 8:00 7:00 6:00 5:00 8:00 Pop Chat WireTap Earth Living Black Art Report Writers & Company The House 8:37 NEWS World 10:00 9:00 8:00 7:00 6:00 9:00 World Report The Current Report The House The Sunday Magazine 10:00 NEWS NEWS NEWS 11:00 10:00 9:00 8:00 7:00 Day 6 q NEWS NEWS NEWS 12:00 11:00 10:00 9:00 8:00 11:00 Because News The Doc Project Because The Cost of What on Front The Pop Chat News Living Earth Burner Debaters NEWS NEWS NEWS 1:00 12:00 The Cost of Living 12:00 11:00 10:00 9:00 Rewind Quirks & Quarks What on Earth NEWS NEWS NEWS 1:00 Pop Chat White Coat Black Art 2:00 1:00 12:00 11:00 10:00 The Next Quirks & Unreserved Tapestry Spark Chapter Quarks Laugh Out Loud The Debaters NEWS NEWS NEWS 2:00 Ideas in 3:00 2:00 1:00 12:00 11:00 Podcast Now or CBC the Spark Now or Never Tapestry Playlist Never Music Live Afternoon NEWS NEWS NEWS 3:00 CBC 4:00 3:00 2:00 1:00 12:00 Writers & The Story Marvin's Reclaimed Music The Next Chapter Writers & Company Company From Here Room Top 20 World This Hr The Cost of Because What on Under the NEWS NEWS 4:00 WireTap 5:00 4:00 3:00 2:00 1:00 Living News Earth Influence Unreserved Cross Country Check- NEWS NEWS Up 5:00 The Current -
The Requisites of Leadership in the Modern House of Commons 1
Number 4 November 2001 CANADIAN STUDY OF PARLIAMENT GROUP HE EQUISITES OF EADERSHIP THE REQUISITES OF LEADERSHIP IN THE MODERN HOUSE OF COMMONS Paper by: Cristine de Clercy Department of Political Studies University of Saskatchewan Canadian Members of the Study of Parliament Executive Committee Group 2000-2001 The Canadian Study of President Parliament Group (CSPG) was created Leo Doyle with the object of bringing together all those with an interest in parliamentary Vice-President institutions and the legislative F. Leslie Seidle process, to promote understanding and to contribute to their reform and Past President improvement. Judy Cedar-Wilson The constitution of the Canadian Treasurer Study of Parliament Group makes Antonine Campbell provision for various activities, including the organization of conferences and Secretary seminars in Ottawa and elsewhere in James R. Robertson Canada, the preparation of articles and various publications, the Counsellors establishment of workshops, the Dianne Brydon promotion and organization of public William Cross discussions on parliamentary affairs, David Docherty participation in public affairs programs Jeff Heynen on radio and television, and the Tranquillo Marrocco sponsorship of other educational Louis Massicotte activities. Charles Robert Jennifer Smith Membership is open to all those interested in Canadian legislative institutions. Applications for membership and additional information concerning the Group should be addressed to the Secretariat, Canadian Study of Parliament Group, Box 660, West Block, Ottawa, Ontario, K1A 0A6. Tel: (613) 943-1228, Fax: (613) 995- 5357. INTRODUCTION This is the fourth paper in the Canadian Study of Parliament Groups Parliamentary Perspectives. First launched in 1998, the perspective series is intended as a vehicle for distributing both studies prepared by academics and the reflections of others who have a particular interest in these themes. -
![[If Non Viewer Skip to Next Section]](https://docslib.b-cdn.net/cover/2188/if-non-viewer-skip-to-next-section-292188.webp)
[If Non Viewer Skip to Next Section]
HNIC Year in Review November 2015 T 1. Thinking about Canadian culture and identity, how important is the game of hockey? Hockey defines Canadian culture Hockey is an important part of Canadian culture – and so are other things Hockey isn’t really a big factor in Canadian culture Hockey is just a game and has nothing to do with Canadian culture T 2. How important is NHL hockey to you? I’m a diehard fan I’m a fan A lot of other interests come before hockey I don’t care about hockey at all T 3. Since the 2015 season began last month, how many NHL games have you watched on TV? More than four 2 or 3 One None [IF NON VIEWER SKIP TO NEXT SECTION] 4. Which statement best describes how you feel about this season of Hockey Night in Canada compared to last year? I like it more than last season I like it less than last season I don’t have a preference either way I haven’t noticed a difference 5. Thinking about the personalities you see on the Hockey Night in Canada broadcasts, tell us how you feel about the overall chemistry of the broadcast team? Would you say: They are clicking together really well The chemistry is okay They have no chemistry T 6. Now, tell us how you feel about how much you’re seeing each of these personalities during the broadcast: Don Cherry George Stroumboulopoulos Ron MacLean Elliot Friedman Nick Kypreos I would like to see more of him I would like to see less of him He’s on for the right amount of time Not sure who that is Don’t know N 7. -

Allan Blakeney: Deftly Navigating Thunderstorms
ALLAN BLAKENEY: DEFTLY NAVIGATING THUNDERSTORMS Brian Topp Saskatchewan Premier Allan Blakeney was one of Canada’s greatest premiers, and there is much for us to learn from his approach to issues ranging from managing a resource dependent economy and the Charter, to how to run a fiscally responsible, economically literate and socially progressive social democratic government. Premier ministre de la Saskatchewan, Allan Blakeney a été l’un des meilleurs chefs provinciaux du pays et aurait beaucoup à nous apprendre aujourd’hui sur la gestion d’une économie tributaire des ressources naturelles, sur la Charte des droits et libertés tout comme le fonctionnement d’un gouvernement social-démocrate qui est à la fois financièrement responsable, économiquement compétent et socialement progressiste. first met Allan Blakeney, one of Canada’s greatest pre- CEOs; constitutional issues; national unity; trade issues. It is miers, during a high-risk aeronautics experiment. not the easy problems that make it onto a premier’s desk. It I Specifically, in the 1990s the Government of is the toughest problems — and it was the very toughest Saskatchewan wanted to see what would happen when a ones that Romanow discussed with Blakeney. couple of Cessna airplanes purchased in the 1960s contin- ued to be flown as the government’s “executive air” fleet to lakeney approached each issue like a fascinating little ferry ministers and officials around the sprawling province. B chess puzzle. What if we did this? What if we did that? Would the planes stay in the air? Or would one of them Did you think of this? What would it mean if that were so? finally break up after decades of loyal service, tumbling with All with a cheerful, wry humour and the slightest undertone some of the province’s most senior people into a wheat field of skepticism about the high principles invoked by princi- 10,000 feet below? The planes spent more time being serv- pals making their cases, usually at high decibels, before the iced than they did flying — they were the last planes of their premier. -

Cross-Border Ties Among Protest Movements the Great Plains Connection
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln Great Plains Quarterly Great Plains Studies, Center for Spring 1997 Cross-Border Ties Among Protest Movements The Great Plains Connection Mildred A. Schwartz University of Illinois at Chicago Follow this and additional works at: https://digitalcommons.unl.edu/greatplainsquarterly Part of the Other International and Area Studies Commons Schwartz, Mildred A., "Cross-Border Ties Among Protest Movements The Great Plains Connection" (1997). Great Plains Quarterly. 1943. https://digitalcommons.unl.edu/greatplainsquarterly/1943 This Article is brought to you for free and open access by the Great Plains Studies, Center for at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in Great Plains Quarterly by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. CROSS .. BORDER TIES AMONG PROTEST MOVEMENTS THE GREAT PLAINS CONNECTION MILDRED A. SCHWARTZ This paper examines the connections among supporters willing to take risks. Thus I hypoth political protest movements in twentieth cen esize that protest movements, free from con tury western Canada and the United States. straints of institutionalization, can readily cross Protest movements are social movements and national boundaries. related organizations, including political pro Contacts between protest movements in test parties, with the objective of deliberately Canada and the United States also stem from changing government programs and policies. similarities between the two countries. Shared Those changes may also entail altering the geography, a British heritage, democratic prac composition of the government or even its tices, and a multi-ethnic population often give form. Social movements involve collective rise to similar problems. l Similarities in the efforts to bring about change in ways that avoid northern tier of the United States to the ad or reject established belief systems or organiza joining sections of Canada's western provinces tions. -

A PRESCRIPTION for HEALTH CARE Introduction
A PRESCRIPTION FOR HEALTH CARE Introduction On November 28, 2002, Roy Romanow tioned whether it would be able to find Focus presented his long-awaited report on the all the new funding Romanow had This News in Re- state of Canada’s health-care system recommended. Finance Minister John view story focuses on the Romanow and a list of 47 major recommendations Manley wondered if the anticipated Report on the state designed to reform it. Eighteen months federal budget surpluses over the next and future of before, Prime Minister Jean Chrétien few years would be large enough to Canada’s health- had named the former Saskatchewan cover the great increase in funding. care system. It premier to head a royal commission to Advocacy groups that had mounted a includes the re- investigate the problems confronting strong campaign in favour of preserving port’s major recom- mendations and the country’s health-care system, and to and strengthening the country’s medi- the political re- recommend improvements to it. care system were delighted with sponse to it, as well Romanow’s report, entitled “Building Romanow’s endorsement of it as one of as its implications on Values: The Future of Health Care in the core values of Canadian society. for the country’s Canada,” was unequivocal in its de- One spokesperson for Canadian Friends medicare system and Canadians’ fence of the country’s free, universal of Medicare, Shirley Douglas, the access to it in system of medical care. It rejected any daughter of T.C. “Tommy” Douglas, future years. suggestions that there should be a the Saskatchewan NDP premier whose greater role for a competing private, government had pioneered public health for-profit sector. -

Legislative Assembly of Alberta Prayers Head:Oral Question Period
June 26, 1990 Alberta Hansard 2211 Legislative Assembly of Alberta Alberta Liquor Control Board for the fiscal year ended January 2, 1990. Title: Tuesday, June 26, 1990 2:30 p.m. MR. GOGO: Mr. Speaker, I wish to table the 1988-89 annual Date: 90/06/26 report of Mount Royal College. [The House met at 2:30 p.m.] head: Introduction of Special Guests MR. GOGO: Mr. Speaker, I'm pleased to introduce today two [Mr. Speaker in the Chair] special guests from the thriving community of Lethbridge. The Prayers Minister of Health is having meetings today with hospital board chairmen and presidents, and seated in the members' gallery is the chairman of the Lethbridge Regional hospital, Mr. Shaun MR. SPEAKER: Let us pray. Ward, and the acting president, Mr. Doug Schindeler. I would We give thanks to God for the rich heritage of this province ask them to rise and be recognized by members of the House. as found in our people. We pray that native-born Albertans and those who have come MR. R. SPEAKER: Mr. Speaker, I would like to introduce to from other places may continue to work together to preserve my colleagues in this Legislature a special guest I met in the and enlarge the precious heritage called Alberta. hallway a few moments ago: Mr. Dmytro Pavlychko. He is a Amen. member of the Supreme Soviet of the Ukraine and also chair• head: Notices of Motions man of the international relations committee. He's accompanied REV. ROBERTS: Mr. Speaker, I'd like to give oral notice of by two persons, one the head of Ukrainian studies with the a motion under the provisions of Standing Order 40 for the University of Alberta, and also Peter Savaryn. -
Appendix 6 Board of Directors’ Response to the Recommendations Presented in the Ombudsmens’ Report
APPENDIX 6 BOARD OF DIRECTORS’ RESPONSE TO THE RECOMMENDATIONS PRESENTED IN THE OMBUDSMENS’ REPORT BOARD OF DIRECTORS of the CANADIAN BROADCASTING CORPORATION STANDING COMMITTEES ON ENGLISH AND FRENCH LANGUAGE BROADCASTING Minutes of the Meeting held on June 18, 2014 Ottawa, Ontario = by videoconference Members of the Committee present: Rémi Racine, Chairperson of the Committees Hubert T. Lacroix Edward Boyd Peter Charbonneau George Cooper Pierre Gingras Marni Larkin Terrence Leier Maureen McCaw Brian Mitchell Marlie Oden Members of the Committee absent: Cecil Hawkins In attendance: Maryse Bertrand, Vice-President, Real Estate, Legal Services and General Counsel Heather Conway, Executive Vice-President, English Services () Louis Lalande, Executive Vice-President, French Services () Michel Cormier, Executive Director, News and Current Affairs, French Services () Stéphanie Duquette, Chief of Staff to the President and CEO Esther Enkin, Ombudsman, English Services () Tranquillo Marrocco, Associate Corporate Secretary Jennifer McGuire, General Manage and Editor in Chief, CBC News and Centres, English Services () Pierre Tourangeau, Ombudsman, French Services () Opening of the Meeting At 1:10 p.m., the Chairperson called the meeting to order. 2014-06-18 Broadcasting Committees Page 1 of 2 1. 2013-2014 Annual Report of the English Services’ Ombudsman Esther Enkin provided an overview of the number of complaints received during the fiscal year and the key subject matters raised, which included the controversy about paid speaking engagements by CBC personalities, the reporting on results polls, the style of, and views expressed by, a commentator, questions relating to matters of taste, the coverage regarding the mayor of Toronto, and the website’s section for comments. She also addressed the manner in which non-news and current affairs complaints are being handled by the Corporation. -

Getting a on Transmedia
® A PUBLICATION OF BRUNICO COMMUNICATIONS LTD. SPRING 2014 Getting a STATE OF SYN MAKES THE LEAP GRIon transmediaP + NEW RIVALRIES AT THE CSAs MUCH TURNS 30 | EXIT INTERVIEW: TOM PERLMUTTER | ACCT’S BIG BIRTHDAY PB.24462.CMPA.Ad.indd 1 2014-02-05 1:17 PM SPRING 2014 table of contents Behind-the-scenes on-set of Global’s new drama series Remedy with Dillon Casey shooting on location in Hamilton, ON (Photo: Jan Thijs) 8 Upfront 26 Unconventional and on the rise 34 Cultivating cult Brilliant biz ideas, Fort McMoney, Blue Changing media trends drive new rivalries How superfans build buzz and drive Ant’s Vanessa Case, and an exit interview at the 2014 CSAs international appeal for TV series with the NFB’s Tom Perlmutter 28 Indie and Indigenous 36 (Still) intimate & interactive 20 Transmedia: Bloody good business? Aboriginal-created content’s big year at A look back at MuchMusic’s three Canadian producers and mediacos are the Canadian Screen Awards decades of innovation building business strategies around multi- platform entertainment 30 Best picture, better box offi ce? 40 The ACCT celebrates its legacy Do the new CSA fi lm guidelines affect A tribute to the Academy of Canadian 24 Synful business marketing impact? Cinema and Television and 65 years of Going inside Smokebomb’s new Canadian screen achievements transmedia property State of Syn 32 The awards effect From books to music to TV and fi lm, 46 The Back Page a look at what cultural awards Got an idea for a transmedia project? mean for the business bottom line Arcana’s Sean Patrick O’Reilly charts a course for success Cover note: This issue’s cover features Smokebomb Entertainment’s State of Syn. -

George Stroumboulopoulos Is a Loner Who Loves Attention, an Anti-Authoritarian Mama's Boy and a Motorcycle-Riding H
By Olivia Stren PHOTOGRAPHY BY FINN O’HARA REBEL REBEL George Stroumboulopoulos is a loner who loves attention, an anti-authoritarian mama’s boy and a motorcycle-riding hedonist who doesn’t drink, smoke or sleep. His job? Save the CBC january 2007 | torontolife.com | ToronTo Life 65 banter about TomKat. Stroumboulopoulos has It’s beautiful.” been cast as the poster boy for a new and aggres- Stroumboulopoulos’s stamina and sively with-it CBC: billboards of the black-clad self-reliance comes from his mother. ex-VJ panel every corner of town. But his talent for Mary Ivanyshan is a petite Ukrainian television lies precisely in his anti-Corp personal- woman with a voice soft as a hankie ity. What he won’t do (he won’t change his wardrobe; and a gentle expression that she passed he won’t play the starchy anchor; he won’t take out on to her son. His father, Mark, a Greek his earrings) is winning him a meteoric career and a from Cairo, worked at a Ford factory in healthy fan base. The Hour now occupies the plum, Oakville. George’s parents were married post-Mansbridge time slot, aiming to compete with the when they were 19, and he was born in biggies: Letterman, Leno, Jon Stewart and CSI. Toronto in 1972. Before George was six, Stroumboulopoulos is the quintessential Torontonian: his family moved about five times in and he is what he does, and he strives, fanatically, for that around the Jane and Wilson area. One conflation. And though thoroughly at ease in front of morning, while seven-year-old George the camera, he seems to long less for the spotlight than was eating a bowl of cereal, he saw his what the spotlight affords: the romance of a ragged, dad, dressed in a suit, walk out the door. -

The Canadian Broadcasting Corporation's Annual Report For
ANNUAL REPORT 2001-2002 Valuable Canadian Innovative Complete Creative Invigorating Trusted Complete Distinctive Relevant News People Trust Arts Sports Innovative Efficient Canadian Complete Excellence People Creative Inv Sports Efficient Culture Complete Efficien Efficient Creative Relevant Canadian Arts Renewed Excellence Relevant Peopl Canadian Culture Complete Valuable Complete Trusted Arts Excellence Culture CBC/RADIO-CANADA ANNUAL REPORT 2001-2002 2001-2002 at a Glance CONNECTING CANADIANS DISTINCTIVELY CANADIAN CBC/Radio-Canada reflects Canada to CBC/Radio-Canada informs, enlightens Canadians by bringing diverse regional and entertains Canadians with unique, and cultural perspectives into their daily high-impact programming BY, FOR and lives, in English and French, on Television, ABOUT Canadians. Radio and the Internet. • Almost 90 per cent of prime time This past year, • CBC English Television has been programming on our English and French transformed to enhance distinctiveness Television networks was Canadian. Our CBC/Radio-Canada continued and reinforce regional presence and CBC Newsworld and RDI schedules were reflection. Our audience successes over 95 per cent Canadian. to set the standard for show we have re-connected with • The monumental Canada: A People’s Canadians – almost two-thirds watched broadcasting excellence History / Le Canada : Une histoire CBC English Television each week, populaire enthralled 15 million Canadian delivering 9.4 per cent of prime time in Canada, while innovating viewers, nearly half Canada’s population. and 7.6 per cent share of all-day viewing. and taking risks to deliver • The Last Chapter / Le Dernier chapitre • Through programming renewal, we have reached close to 5 million viewers for its even greater value to reinforced CBC French Television’s role first episode.