Feed the Future Tajikistan Health and Nutrition Activity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pdf | 336.56 Kb
RAPID EMERGENCY ASSESSMENT AND COORDINATION TEAM (REACT) Floods in Khatlon: 7 – 13 May 2021 Situation Report # 1 (as of 14 May 2021) Highlights - Over 12 mudflows and landslides have been reported during the period of 7 – 13 May 2021. - Mudflows caused the death of 9 people. - Over 70 households are left homeless. - Large number of cattle has been lost and agricultural crops destroyed. - Mudflows caused disruptions to the livelihoods of around 22,000 people Situation Overview The torrential rains of 7 – 12 May 2021 triggered floods, landslides and mudflows in many of the country’s districts. The largest number of losses and destructions are faced by districts and cities of Khatlon province. Disasters affected following cities and districts: Kulob city and districts of Shamsiddini Shohin, Qushoniyon, Dangara, Yovon, Khuroson, Dusti, Vaksh, Muminobod and Jomi (please refer to Map below). CoES reports that disasters caused the death 9 people. Very preliminary estimates indicate that 74 households were left homeless and houses of another 270 households were damaged to different extent. Very modest estimations indicate damages caused by disasters to private and social infrastructure caused disruptions to the livelihoods of around 22,000 people. Government of Tajikistan activated an Inter-Agency Commission on Emergency Situations (Commission) in each disaster affected district, which fully facilitates the response operations. Furthermore, Emergency Operations Centers (Shtab) have been set up in each disaster affected district, which collects and analyzes relevant information and coordinates the response activities. Up to date, general response actions in every district include: search and rescue, evacuation of population from risk zones, constant disinfection of the affected territories, debris removal, assessment of damages and needs, registration of affected population, restoration of communal services, collection and distribution of immediate relief assistance, as well as recovery planning. -

Application of Space Based Technologies for Disaster Risk Assessment at the Level of Communities A. Shomahmadov
Asian Conference on Disaster Risk Reduction January 23 rd 2013 , Kobe, Japan Application of space based technologies for Disaster Risk Assessment at the level of communities A. Shomahmadov Head of the Information Management and Analytical Center (IMAC) of the Committee of ES and CD, Tajikistan SSpacepace Based Technologies Application GIS mapping and application of geospatial information systems, which have become widespread and recognized in Tajikistan, allow to use innovative and effective approaches for the analysis of the information about disasters and solve tasks on their prevention and risk reduction. They play an especially important role for decision-making in socio- economic, economic, political and ecological spheres of development, disaster and natural resources management. A lot of agencies and departments are getting more and more concerned with the lack of qualified specialists who can effectively use GIS technologies and geospatial information systems for scientific research and decision-making. 1 SSpacepace Based Technologies Application Recent important achievements of the GIS technologies and remote sensing: 1. Monitoring and Early Warning System was installed in 2004 at the lake Sarez and it conducts the following kinds of measurements: Surface displacements on the body of the Usoi Landslide Dam; Registration of strong movements during earthquakes; Water level of the lake and maximal wave height; The water discharge of the Murghab river; Turbidity of the drain flow from the lake; Meteorological data. Components of the Monitoring System are used for the activation of the warning system and they are integrated into EarlyWarning System. The transmission of all data, warning signals and remote supervision over the system is carried out through the satellite system INMARSAT, or locally, through cables on short distances. -
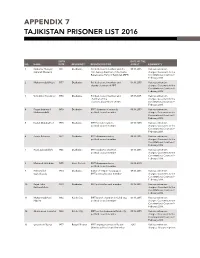
Appendix 7 Tajikistan Prisoner List 2016
APPENDIX 7 TAJIKISTAN PRISONER LIST 2016 BIRTH DATE OF THE NO. NAME DATE RESIDENCY RESPONSIBILITIES ARREST COMMENTS 1 Saidumar Huseyini 1961 Dushanbe Political council member and the 09.16.2015 Various extremism (Umarali Khusaini) first deputy chairman of the Islamic charges. Case went to the Renaissance Party of Tajikistan (IRPT) Constitutional Court on 9 February 2016. 2 Muhammadalii Hayit 1957 Dushanbe Political council member and 09.16.2015 Various extremism deputy chairman of IRPT charges. Case went to the Constitutional Court on 9 February 2016. 3 Vohidkhon Kosidinov 1956 Dushanbe Political council member and 09.17.2015 Various extremism chairman of the charges. Case went to the elections department of IRPT Constitutional Court on 9 February 2016. 4 Fayzmuhammad 1959 Dushanbe IRPT chairman of research, 09.16.2015 Various extremism Muhammadalii political council member charges. Case went to the Constitutional Court on 9 February 2016. 5 Davlat Abdukahhori 1975 Dushanbe IRPT foreign relations, 09.16.2015 Various extremism political council member charges. Case went to the Constitutional Court on 9 February 2016. 6 Zarafo Rahmoni 1972 Dushanbe IRPT chairman advisor, 09.16.2015 Various extremism political council member charges. Case went to the Constitutional Court on 9 February 2016. 7 Rozik Zubaydullohi 1946 Dushanbe IRPT academic chairman, 09.16.2015 Various extremism political council member charges. Case went to the Constitutional Court on 9 February 2016. 8 Mahmud Jaloliddini 1955 Hisor District IRPT chairman advisor, 02.10.2015 political council member 9 Hikmatulloh 1950 Dushanbe Editor of “Najot” newspaper, 09.16.2015 Various extremism Sayfullozoda IRPT political council member charges. -

Initial Environmental Examination
INITIAL ENVIRONMENTAL EXAMINATION ADB LOAN L3451 / GRANT 0509 / GRANT 0510 REPUBLIC OF TAJIKISTAN: CENTRAL ASIA REGIONAL ECONOMIC COOPERATION (CAREC): CORRIDORS 2, 5, AND 6 (DUSHANBE - KURGONTEPPA ROAD PROJECT) - PHASE 1 (KM 0+275-33+475) Preparation of Road Network Sustainability Project in the Republic of Tajikistan Bokhtar – Dangara Road Rehabilitation Section Prepared by the KOCKS Consult GmbH for Ministry of Transport of Tajikistan and Ministry of Transport. The IEE is a document of the Borrower. This initial environmental examination report is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. August 2020 CONTENTS EXECUTIVE SUMMARY ................................................................................................... 5 I. INTRODUCTION ................................................................................................... 12 A. PROJECT BACKGROUND AND PURPOSE OF THE REPORT ........................... 12 B. PURPOSE OF THE INITIAL ENVIRONMENTAL EXAMINATION ......................... 15 II. LEGAL, POLICY AND ADMINISTRATIVE FRAMEWORK .................................. 19 A. ENVIRONMENTAL CLEARANCE -

World Bank Document
FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: PAD3028 INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT APPRAISAL DOCUMENT ON A PROPOSED GRANT Public Disclosure Authorized IN THE AMOUNT OF SDR 41.80 MILLION (US$ 58 MILLION EQUIVALENT) TO THE REPUBLIC OF TAJIKISTAN FOR A Public Disclosure Authorized RURAL WATER SUPPLY AND SANITATION PROJECT February 4, 2019 Water Global Practice Europe And Central Asia Region Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective December 31, 2018) Currency Unit = SDR 0.719 = US$1 US$ 1.391 = SDR 1 FISCAL YEAR January 1 - December 31 Regional Vice President: Cyril E Muller Country Director: Lilia Burunciuc Senior Global Practice Director: Jennifer Sara Practice Manager: David Michaud Task Team Leader(s): Sana Kh.H. Agha Al Nimer, Farzona Mukhitdinova ABBREVIATIONS AND ACRONYMS ADB Asian Development Bank AF Additional Financing APA Alternate Procurement Arrangements CERC Contingent Emergency Response Component CPF Country Partnership Strategy CSC Community Scorecard DA Designated Account DFIL Disbursement and Financial Information Letter EBRD European Bank for Reconstruction and Development ESMF Environmental and Social Management Framework ESMPs Environmental and Social Management Plans FCV Fragility, Conflict and Violence FI Financial Intermediaries FM Financial Management -

Tajikistan 2016 Human Rights Report
TAJIKISTAN 2016 HUMAN RIGHTS REPORT EXECUTIVE SUMMARY Tajikistan is an authoritarian state dominated politically by President Emomali Rahmon and his supporters. The constitution provides for a multiparty political system, but the government has historically obstructed political pluralism and continued to do so during the year. A constitutional amendment approved in a national referendum on May 22 outlawed non-secular political parties and removed any limitation on President Rahmon’s terms in office as the “Leader of the Nation,” allowing him to further solidify his rule. Civilian authorities only partially maintained effective control over security forces. Officials in the security services and elsewhere in the government acted with impunity. The most significant human rights problems included citizens’ inability to change their government through free and fair elections; torture and abuse of detainees and other persons by security forces; repression, increased harassment, and incarceration of civil society and political activists; and restrictions on freedoms of expression, media, and the free flow of information, including through the repeated blockage of several independent news and social networking websites. Other human rights problems included torture in the military; arbitrary arrest; denial of the right to a fair trial; harsh and life-threatening prison conditions; prohibition of international monitors’ access to prisons; poor religious freedom conditions; violence and discrimination against women; limitations on worker rights; and trafficking in persons, including sex and labor trafficking. There were very few prosecutions of government officials for human rights abuses. Section 1. Respect for the Integrity of the Person, Including Freedom from: a. Arbitrary Deprivation of Life and other Unlawful or Politically Motivated Killings While the law prohibits extrajudicial killings by government security forces, there were several reports that the government or its agents committed arbitrary or unlawful killings. -

Tajikistan Act Appeal for Extreme Winter 08
150 route de Ferney, P.O. Box 2100 1211 Geneva 2, Switzerland Tel: 41 22 791 6033 Fax: 41 22 791 6506 Appeal E-mail: [email protected] Coordinating Office Tajikistan Severe Weather - ASCE81 Appeal Target: US$ 169,540 Balance Requested: US$ 139,540 Geneva, 19 March 2008 Dear Colleagues, Tajikistan is experiencing its harshest winter in three decades with unusually low temperatures. T he cold weather over the last months and the ensuing shortage of electricity ha ve crippled the population, particularly in urban areas which depend on electricity for heating, cooking and water supply. Children and the elderly are among the most vulnerable people being hit by these conditions. As a result of heavy snowfalls, roads between several districts were blocked, which has also reduced local supplies of food and other basic commodities. According to media reports, 303 babies and 12 young women have died as a result of this situation over the last month (Source: Asia Plus). Many antiquated water lines had broken or become clogged. Meanwhile heating and electricity have been restored In Dushanbe, but in the higher altitudes, extreme cold and power outages prevail. There is a risk of flooding and mudslides and outbreak of typhoid as a result of precarious health conditions. The World Health Organization (WHO), together with other agencies, has identified critical food and non-food items are needed to mit igate against immediate, life threatening conditions. These items include wheat flour and vegetable oil in particular, warm clothes for children and the elderly, blankets and sleeping mats, jerry cans for carrying and storing water, flashlights, batteries, candles, matches, generators and fuel, and medicines. -

Feed the Future Tajikistan Health and Nutrition Activity
FEED THE FUTURE TAJIKISTAN HEALTH AND NUTRITION ACTIVITY Annual Progress Report October 2017 to September 2018 Submitted October 30, 2018 Table of contents Acronyms and Abbreviations ................................................................................ 4 Activity Implementation Summary ....................................................................... 5 IR 1: IMPROVED QUALITY OF HEALTH CARE SERVICES FOR MNCH ...................... 7 Outcome 1.1: Improved quality of health care services being provided in the FTF ZOI ................ 7 Outcome 1.2: Improved patient access to health care services in the FTF ZOI due to improved quality .................................................................................................... 14 Outcome 1.3: Stronger facility and provider networks ................................................................ 18 1.3.1. Hospital-level activities .................................................................................................................. 18 1.3.2. Primary health care activities ......................................................................................................... 19 IR 2: INCREASED ACCESS TO A DIVERSE SET OF NUTRIENT-RICH FOODS ............ 20 Outcome 2.1: Diversified food consumption during the growing season and beyond ............... 20 Outcome 2.2: Nutrition integrated into agriculture-focused programs and linked to value chains supported through FTF activities ....................................................... 23 IR 3: INCREASED PRACTICE -
40046-013: Completion Report
Completion Report Project Number: 40046-013 Loan Number: 2356 April 2015 Tajikistan: Khatlon Province Flood Risk Management Project This document is being disclosed to the public in accordance with ADB’s Public Communications Policy 2011. CURRENCY EQUIVALENTS Currency Unit – somoni (TJS) At Project Design At Project Completion (31 August 2007) (6 April 2015) TJS1.00 = $0.29 $0.17 $1.00 = TJS3.44 TJS5.80 ABBREVIATIONS ADB – Asian Development Bank CES – Committee for Emergency Situations CIS – Chubek irrigation system CPS – country partnership strategy DMF – design and monitoring framework EIRR – economic internal rate of return ha – hectare Hydromet – Agency for Hydrometeorology ICB – international competitive bidding JFPR – Japan Fund for Poverty Reduction km – kilometer MLRWR – Ministry of Land Reclamation and Water Resources NCB – national competitive bidding NGO – nongovernment organization O&M – operation and maintenance PCR – project completion report PIO – project implementation office PMO – project management office PPTA – project preparatory technical assistance SDR – special drawing rights WRM – water resources management GLOSSARY jamoat – administrative unit below the district, comprising a group of villages; also the lowest level of local government administration NOTES (i) The fiscal year (FY) of the government and its agencies ends on 31 December. FY before a calendar year denotes the year in which the fiscal year ends, e.g., FY2009 ends on 31 December 2009. (ii) In this report, "$" refers to US dollars. Vice-President W. Zhang, Operations Group 1 Director General K. Gerhaeusser, Central and West Asia Department (CWRD) Director A. Siddiq, Environment, Natural Resources and Agriculture Division, CWRD Team leader R. Takaku, Senior Water Resources Specialist, CWRD Team members G. -

International Alert's Tajikistan Case Study, Climate Change, Complexity and Resilient Communities
CLIMATE CHANGE, COMPLEXITY AND RESILIENT COMMUNITIES Case study: Tajikistan Shreya Mitra and Janani Vivekananda, September 2013 CONTEXT Central Asia faces the double burden of fragility and climate change. Uneven distribution of resources across the various Central Asian countries poses significant risks to stability, with climate change adding an additional layer of insecurity. The collapse of the Soviet Union left some Central Asian countries with an abundance of water resources but limited fossil fuel energy and others with less water but more fossil fuel reserves. Transboundary sharing of water and energy resources has caused escalating tensions between the various neighbours in the region. Climate change will act as a threat multiplier by negatively impacting on the availability of these natural resources, with rising temperatures and frequent and more intensified drought already decreasing the water reserves available to upstream countries. Hydropower resources are concentrated in Kyrgyzstan and Tajikistan, the upstream countries of Central Asia’s Amu Darya and Syr Darya rivers. These countries however, have a negligible share of fossil fuels. Water is therefore the cheapest source of electricity for them. Downstream countries Uzbekistan, Turkmenistan and Kazakhstan, on the other hand, are dependent upon water flows, especially for irrigation from the upstream countries, but are better endowed with fossil fuels and are suppliers of gas and coal to their upstream neighbours. Hydropower is especially important for the upstream countries during winter months, when heating needs are highest. As flows during winter are limited, Kyrgyzstan and Tajikistan store water in large reservoirs during the summertime, when water flows are more abundant. The summer months however, are precisely the months when the irrigation needs of the downstream countries are most acute. -

Republic of the Philippines
Chapter 3 Final Report Power Development Plan (1st Screening) CHAPTER 3 POWER DEVELOPMENT PLAN (1ST SCREENING) Data Collection Survey on the Installment of Small Hydropower Stations for the Communities of Khatlon Oblast, Tajikistan Chapter 3 Final Report Power Development Plan (1st Screening) CHAPTER 3 POWER DEVELOPMENT PLAN (1ST SCREENING) 3.1 CONSIDERATION OF POWER DISCHARGE 3.1.1 Collection on Hydrological Data Hydrological data of nine hydropower potential sites will be collected. Potential sites are classified into two types, sites using natural rivers (Yokunch and Baljuvon) and artificial canals (Nurbakhsh, Surhak-1, Sathad, Shibanai, Pakhtakor, Faizobod and Bohtar). Hydrological data are essential factor for power generation plan such as maximum power discharge, annual power generation, plant capacity factor and so on. Therefore it is important to ensure the reliability of the data by using various documents. Meanwhile, it is difficult to collect reliable hydrological data in Tajikistan due to lack of observation stations, aging facilities and inadequacy of operation record of intake weirs. As discharge data of artificial canals is particularly unavailable, discharge is estimated by means of site surveys, relevant data and interviews at the 1st screening stage. (1) Natural River River observation stations at Khatlon province are as shown in Table 3.1-1. Since hydrological data is not observed at Yokunch and Baljuvon rivers, the discharge data at these sites is estimated by hydrological data of Yaksu river and Kizilsu river Fig. 3.1-1 River Observation Stations at Khatlon Province Data Collection Survey on the Installment 3 - 1 of Small Hydropower Stations for the Communities of Khatlon Oblast, Tajikistan Chapter 3 Power Development Plan (1st Screening) Final Report Table 3.1-1 Hydrological Gauging Stations at Khatlon Province Station Observation Period (Data Availability) Period of Data Station Name River No. -

Activity in Tajikistan
LIVELIHOODS άͲ͜ͲG ͞΄ͫΕ͟ ACTIVITY IN TAJIKISTAN A SPECIAL REPORT BY THE FAMINE EARLY WARNING SYSTEMS NETWORK (FEWS NET) January 2011 LIVELIHOODS άͲ͜ͲG ͞΄ͫΕ͟ ACTIVITY IN TAJIKISTAN A SPECIAL REPORT BY THE FAMINE EARLY WARNING SYSTEMS NETWORK (FEWS NET) January 2011 Α·͋ ̯Ϣχ·Ϊιν͛ ϭΊ͋Ϯν ͋ϳζι͋νν͇͋ ΊΣ χ·Ίν ζϢ̼ΜΊ̯̽χΊΪΣ ͇Ϊ ΣΪχ Σ͋̽͋νν̯ιΊΜϴ ι͕͋Μ͋̽χ χ·͋ ϭΊ͋Ϯν Ϊ͕ χ·͋ United States Agency for International Development or the United States Government. 1 Contents Acknowledgments ......................................................................................................................................... 3 Methodology ................................................................................................................................................. 3 National Livelihood Zone Map and Seasonal Calendar ................................................................................ 4 Livelihood Zone 1: Eastern Pamir Plateau Livestock Zone ............................................................................ 1 Livelihood Zone 2: Western Pamir Valley Migratory Work Zone ................................................................. 3 Livelihood Zone 3: Western Pamir Irrigated Agriculture Zone .................................................................... 5 Livelihood Zone 4: Rasht Valley Irrigated Potato Zone ................................................................................. 7 Livelihood Zone 5: Khatlon Mountain Agro-Pastoral Zone ..........................................................................