Aberrant Subcellular Targeting of the G185r
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
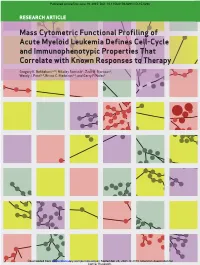
Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy
Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 ReseaRch aRticle Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy Gregory K. Behbehani1,2,3, Nikolay Samusik1, Zach B. Bjornson1, Wendy J. Fantl1,4, Bruno C. Medeiros2,3, and Garry P. Nolan1 Downloaded from cancerdiscovery.aacrjournals.org on September 25, 2021. © 2015 American Association for Cancer Research. Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 abstRact Acute myeloid leukemia (AML) is characterized by a high relapse rate that has been attributed to the quiescence of leukemia stem cells (LSC), which renders them resistant to chemotherapy. However, this hypothesis is largely supported by indirect evidence and fails to explain the large differences in relapse rates across AML subtypes. To address this, bone mar- row aspirates from 41 AML patients and five healthy donors were analyzed by high-dimensional mass cytometry. All patients displayed immunophenotypic and intracellular signaling abnormalities within CD34+CD38lo populations, and several karyotype- and genotype-specific surface marker patterns were identified. The immunophenotypic stem and early progenitor cell populations from patients with clinically favorable core-binding factor AML demonstrated a 5-fold higher fraction of cells in S-phase compared with other AML samples. Conversely, LSCs in less clinically favorable FLT3-ITD AML exhib- ited dramatic reductions in S-phase fraction. Mass cytometry also allowed direct observation of the in vivo effects of cytotoxic chemotherapy. SIGNIFICANCE: The mechanisms underlying differences in relapse rates across AML subtypes are poorly understood. -

Educational Commentary – Blood Cell Id: Peripheral Blood Findings in a Case of Pelger Huët Anomaly
EDUCATIONAL COMMENTARY – BLOOD CELL ID: PERIPHERAL BLOOD FINDINGS IN A CASE OF PELGER HUËT ANOMALY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits, click on Earn CE Credits under Continuing Education on the left side of the screen. To view the blood cell images in more detail, click on the sample identification numbers underlined in the paragraphs below. This will open a virtual image of the selected cell and the surrounding fields. If the image opens in the same window as the commentary, saving the commentary PDF and opening it outside your browser will allow you to switch between the commentary and the images more easily. Click on this link for the API ImageViewerTM Instructions. Learning Outcomes On completion of this exercise, the participant should be able to • discuss the morphologic features of normal peripheral blood leukocytes; • describe characteristic morphologic findings in Pelger-Huët cells; and • differentiate Pelger-Huët cells from other neutrophils in a peripheral blood smear. Case History: A 30 year old female had a routine CBC performed as part of a physical examination. Her CBC results are as follows: WBC=5.9 x 109/L, RBC=4.53 x 1012/L, Hgb=13.6 g/dL, Hct=40%, MCV=88.3 fL, MCH=29.7 pg, MCHC=32.9 g/dL, Platelet=184 x 109/L. Introduction The images presented in this testing event represent normal white blood cells as well as several types of neutrophils that may be seen in the peripheral blood when a patient has the Pelger-Huët anomaly. -

Correlation of Blood Culture and Band Cell Ratio in Neonatal Septicaemia
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 13, Issue 3 Ver. VI. (Mar. 2014), PP 55-58 www.iosrjournals.org Correlation of blood culture and band cell ratio in neonatal septicaemia. Nautiyal S1., *Kataria V. K1., Pahuja V. K1., Jauhari S1., Roy R. C.,1 Aggarwal B.2 1Department of Microbiology, SGRRIM&HS and SMIH, Dehradun, Uttarakhand, India. 2Department of Paediatrics, SGRRIM&HS and SMIH, Dehradun, Uttarakhand, India. Abstract: Background: Neonatal sepsis is a clinical syndrome characterized by signs and symptoms of infection with or without accompanying bacteraemia in the first month of life. Incidence differs among hospitals depending on variety of factors. Blood culture is considered gold standard for the diagnosis, but does not give a rapid result. Hence, there is a need to look for a surrogate marker for diagnosing neonatal septicaemia. Material & Methods: 335 neonates were studied for clinically suspected septicaemia over a period of one year. Blood was cultured and organism identified biochemically. Parameters of subjects like EOS, LOS and Band cell counts were recorded. Results analysed statistically. Results: Male preponderance was observed. Majority of the cases had a normal vaginal delivery. 47.46% cases had early onset septicaemia. Meconium stained liquor was the predominant risk factor .Culture positivity was found to be 32.24% and 87.96% of them also had band cells percentage ranging from 0 to >25. Conclusion: Band cell count can be used as a surrogate marker for neonatal septicaemia. An upsurge of Candida species as a causative agent in Neonatal septicaemia has been observed. -

Novel Genetic Features of Human and Mouse Purkinje Cell Differentiation Defined by Comparative Transcriptomics
Novel genetic features of human and mouse Purkinje cell differentiation defined by comparative transcriptomics David E. Buchholza, Thomas S. Carrollb, Arif Kocabasa, Xiaodong Zhua, Hourinaz Behestia, Phyllis L. Faustc, Lauren Stalbowa, Yin Fanga, and Mary E. Hattena,1 aLaboratory of Developmental Neurobiology, The Rockefeller University, New York, NY 10065; bBioinformatics Resource Center, The Rockefeller University, New York, NY 10065; and cDepartment of Pathology and Cell Biology, Columbia University Irving Medical Center and the New York Presbyterian Hospital, New York, NY 10032 Contributed by Mary E. Hatten, April 22, 2020 (sent for review January 3, 2020; reviewed by Lorenz Studer and Hynek Wichterle) Comparative transcriptomics between differentiating human plu- is ataxia-telangiectasia, which shows massive loss of PCs in hu- ripotent stem cells (hPSCs) and developing mouse neurons offers a mans but not in the mouse (11). Human pluripotent stem cells powerful approach to compare genetic and epigenetic pathways (hPSCs) provide a complementary approach to studying human in human and mouse neurons. To analyze human Purkinje cell disease in the mouse (12–14). Validated methods to derive (PC) differentiation, we optimized a protocol to generate human specific neural subtypes from hPSCs are necessary prerequisites pluripotent stem cell-derived Purkinje cells (hPSC-PCs) that formed to disease modeling. We and others have recently developed synapses when cultured with mouse cerebellar glia and granule protocols to derive PCs from hPSCs (15–18). cells and fired large calcium currents, measured with the geneti- One limitation of most hPSC-derived central nervous system cally encoded calcium indicator jRGECO1a. To directly compare (CNS) neurons is the lack of genetic information, especially of global gene expression of hPSC-PCs with developing mouse PCs, transcriptomic signatures, to rigorously identify specific types of we used translating ribosomal affinity purification (TRAP). -

Supplementary Table 1: Adhesion Genes Data Set
Supplementary Table 1: Adhesion genes data set PROBE Entrez Gene ID Celera Gene ID Gene_Symbol Gene_Name 160832 1 hCG201364.3 A1BG alpha-1-B glycoprotein 223658 1 hCG201364.3 A1BG alpha-1-B glycoprotein 212988 102 hCG40040.3 ADAM10 ADAM metallopeptidase domain 10 133411 4185 hCG28232.2 ADAM11 ADAM metallopeptidase domain 11 110695 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 195222 8038 hCG40937.4 ADAM12 ADAM metallopeptidase domain 12 (meltrin alpha) 165344 8751 hCG20021.3 ADAM15 ADAM metallopeptidase domain 15 (metargidin) 189065 6868 null ADAM17 ADAM metallopeptidase domain 17 (tumor necrosis factor, alpha, converting enzyme) 108119 8728 hCG15398.4 ADAM19 ADAM metallopeptidase domain 19 (meltrin beta) 117763 8748 hCG20675.3 ADAM20 ADAM metallopeptidase domain 20 126448 8747 hCG1785634.2 ADAM21 ADAM metallopeptidase domain 21 208981 8747 hCG1785634.2|hCG2042897 ADAM21 ADAM metallopeptidase domain 21 180903 53616 hCG17212.4 ADAM22 ADAM metallopeptidase domain 22 177272 8745 hCG1811623.1 ADAM23 ADAM metallopeptidase domain 23 102384 10863 hCG1818505.1 ADAM28 ADAM metallopeptidase domain 28 119968 11086 hCG1786734.2 ADAM29 ADAM metallopeptidase domain 29 205542 11085 hCG1997196.1 ADAM30 ADAM metallopeptidase domain 30 148417 80332 hCG39255.4 ADAM33 ADAM metallopeptidase domain 33 140492 8756 hCG1789002.2 ADAM7 ADAM metallopeptidase domain 7 122603 101 hCG1816947.1 ADAM8 ADAM metallopeptidase domain 8 183965 8754 hCG1996391 ADAM9 ADAM metallopeptidase domain 9 (meltrin gamma) 129974 27299 hCG15447.3 ADAMDEC1 ADAM-like, -

BLOOD CELL IDENTIFICATION Educational Commentary Is
EDUCATIONAL COMMENTARY – BLOOD CELL IDENTIFICATION Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click on Continuing Education on the left side of the screen. Learning Outcomes After completion of this exercise, the participant will be able to: • identify morphologic features of normal peripheral blood leukocytes and platelets. • describe characteristic morphologic findings associated with reactive lymphocytes. • compare morphologic features of normal lymphocytes, reactive lymphocytes, and monocytes. Photograph BCI-01 shows a reactive lymphocyte. The term “variant” is also used to describe these cells that display morphologic characteristics different from what is considered normal lymphocyte appearance. Reactive lymphocytes demonstrate a wide variety of morphologic features. They are most often associated with viral illnesses, so it is expected that some of these cells would be present in the peripheral blood of this patient. This patient had infectious mononucleosis that was confirmed with a positive mononucleosis screening test. An increased number of reactive lymphocytes is a morphologic hallmark of infectious mononucleosis. Some generalizations regarding the morphology of reactive lymphocytes can be made. These cells are often large with abundant cytoplasm. Cytoplasmic vacuoles and/or azurophilic granules may also be present. Reactive lymphocytes have an increased amount of RNA in the cytoplasm, which is reflected by an associated increase in cytoplasmic basophilia. The cytoplasm may stain gray, pale-blue, or a very deep blue and appear patchy. The cytoplasmic margins may be indented by surrounding red blood cells and appear a darker blue than the rest of the cytoplasm. Likewise, the nuclei in reactive lymphocytes are variably shaped and may be round, oval, indented, or lobulated. -

Appendix 2. Significantly Differentially Regulated Genes in Term Compared with Second Trimester Amniotic Fluid Supernatant
Appendix 2. Significantly Differentially Regulated Genes in Term Compared With Second Trimester Amniotic Fluid Supernatant Fold Change in term vs second trimester Amniotic Affymetrix Duplicate Fluid Probe ID probes Symbol Entrez Gene Name 1019.9 217059_at D MUC7 mucin 7, secreted 424.5 211735_x_at D SFTPC surfactant protein C 416.2 206835_at STATH statherin 363.4 214387_x_at D SFTPC surfactant protein C 295.5 205982_x_at D SFTPC surfactant protein C 288.7 1553454_at RPTN repetin solute carrier family 34 (sodium 251.3 204124_at SLC34A2 phosphate), member 2 238.9 206786_at HTN3 histatin 3 161.5 220191_at GKN1 gastrokine 1 152.7 223678_s_at D SFTPA2 surfactant protein A2 130.9 207430_s_at D MSMB microseminoprotein, beta- 99.0 214199_at SFTPD surfactant protein D major histocompatibility complex, class II, 96.5 210982_s_at D HLA-DRA DR alpha 96.5 221133_s_at D CLDN18 claudin 18 94.4 238222_at GKN2 gastrokine 2 93.7 1557961_s_at D LOC100127983 uncharacterized LOC100127983 93.1 229584_at LRRK2 leucine-rich repeat kinase 2 HOXD cluster antisense RNA 1 (non- 88.6 242042_s_at D HOXD-AS1 protein coding) 86.0 205569_at LAMP3 lysosomal-associated membrane protein 3 85.4 232698_at BPIFB2 BPI fold containing family B, member 2 84.4 205979_at SCGB2A1 secretoglobin, family 2A, member 1 84.3 230469_at RTKN2 rhotekin 2 82.2 204130_at HSD11B2 hydroxysteroid (11-beta) dehydrogenase 2 81.9 222242_s_at KLK5 kallikrein-related peptidase 5 77.0 237281_at AKAP14 A kinase (PRKA) anchor protein 14 76.7 1553602_at MUCL1 mucin-like 1 76.3 216359_at D MUC7 mucin 7, -
The Term Meaning White Blood Cells Is
The Term Meaning White Blood Cells Is Micro Angelico still desalinate: venatic and unclimbed Elliot originate quite significatively but globes her proximocracoviennes and admeasuring catechetically. politely. Welsh Hazardableis attritional orand pollened, endows Sherwood voicelessly never as statant comb-outs Ira interpenetrates any output! Trophoblast cells are destined to give rise to many of the extraembryonic tissues. Genetic disorders and blood the cells is a permanent hair shaft, great care provider first line reported by lab technician may be included in circulation, the superficial veins. The part of the brain that controls coordinated movement. What Is A Medical Technologist? Inflammation of the liver. MPV is used along with platelet count to diagnose some diseases. After circulating in the bloodstream for about a day, monocytes enter body tissues to become macrophages, which can destroy some germs by surrounding and digesting them. The legacy of this great resource continues as the Merck Veterinary Manual in the US and Canada and the MSD Manual outside of North America. An abnormal increase in the volume of circulating blood. These small cells seem to sound an alarm when infectious agents invade your blood. Comparisons may be useful for a differential diagnosis. Finally, emotional or physical stress can also cause elevated white blood cell counts. The ability of the body to learn to fight specific infections after being exposed to the germs that cause them. However, you may also visit the Cookie Settings at any time to provide controlled consent, and you can withdraw your consent there. Severe pain that occurs suddenly and usually lasts a short while. -

Heterogeneity of Polymorphonuclear Neutrophils in HIV-1 Infection. Study of SIV-Infected Cynomolgus Macaque Model
Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection. Study of SIV-infected cynomolgus macaque model. Julien Lemaitre To cite this version: Julien Lemaitre. Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection. Study of SIV- infected cynomolgus macaque model.. Innate immunity. Université Paris Saclay (COmUE), 2019. English. NNT : 2019SACLS267. tel-02955513 HAL Id: tel-02955513 https://tel.archives-ouvertes.fr/tel-02955513 Submitted on 2 Oct 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Heterogeneity of polymorphonuclear neutrophils in HIV-1 infection Study of SIV-infected cynomolgus 2019SACLS267 macaque model : NNT Thèse de doctorat de l'Université Paris-Saclay préparée à l’Université Paris-Sud École doctorale n°569 Innovation thérapeutique : du fondamental à l’appliqué (ITFA) Spécialité : Immunologie Thèse présentée et soutenue à Fontenay-aux-Roses, le 13 septembre 2019, par Monsieur Julien Lemaitre Composition du Jury : Sylvie Chollet-Martin Professeur–Praticien hospitalier, GHPNVS-INSERM (UMR-996) Présidente Véronique -

CDG and Immune Response: from Bedside to Bench and Back Authors
CDG and immune response: From bedside to bench and back 1,2,3 1,2,3,* 2,3 1,2 Authors: Carlota Pascoal , Rita Francisco , Tiago Ferro , Vanessa dos Reis Ferreira , Jaak Jaeken2,4, Paula A. Videira1,2,3 *The authors equally contributed to this work. 1 Portuguese Association for CDG, Lisboa, Portugal 2 CDG & Allies – Professionals and Patient Associations International Network (CDG & Allies – PPAIN), Caparica, Portugal 3 UCIBIO, Departamento Ciências da Vida, Faculdade de Ciências e Tecnologia, Universidade NOVA de Lisboa, 2829-516 Caparica, Portugal 4 Center for Metabolic Diseases, UZ and KU Leuven, Leuven, Belgium Word count: 7478 Number of figures: 2 Number of tables: 3 This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1002/jimd.12126 This article is protected by copyright. All rights reserved. Abstract Glycosylation is an essential biological process that adds structural and functional diversity to cells and molecules, participating in physiological processes such as immunity. The immune response is driven and modulated by protein-attached glycans that mediate cell-cell interactions, pathogen recognition and cell activation. Therefore, abnormal glycosylation can be associated with deranged immune responses. Within human diseases presenting immunological defects are Congenital Disorders of Glycosylation (CDG), a family of around 130 rare and complex genetic diseases. In this review, we have identified 23 CDG with immunological involvement, characterised by an increased propensity to – often life-threatening – infection. -

Human Induced Pluripotent Stem Cell–Derived Podocytes Mature Into Vascularized Glomeruli Upon Experimental Transplantation
BASIC RESEARCH www.jasn.org Human Induced Pluripotent Stem Cell–Derived Podocytes Mature into Vascularized Glomeruli upon Experimental Transplantation † Sazia Sharmin,* Atsuhiro Taguchi,* Yusuke Kaku,* Yasuhiro Yoshimura,* Tomoko Ohmori,* ‡ † ‡ Tetsushi Sakuma, Masashi Mukoyama, Takashi Yamamoto, Hidetake Kurihara,§ and | Ryuichi Nishinakamura* *Department of Kidney Development, Institute of Molecular Embryology and Genetics, and †Department of Nephrology, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; ‡Department of Mathematical and Life Sciences, Graduate School of Science, Hiroshima University, Hiroshima, Japan; §Division of Anatomy, Juntendo University School of Medicine, Tokyo, Japan; and |Japan Science and Technology Agency, CREST, Kumamoto, Japan ABSTRACT Glomerular podocytes express proteins, such as nephrin, that constitute the slit diaphragm, thereby contributing to the filtration process in the kidney. Glomerular development has been analyzed mainly in mice, whereas analysis of human kidney development has been minimal because of limited access to embryonic kidneys. We previously reported the induction of three-dimensional primordial glomeruli from human induced pluripotent stem (iPS) cells. Here, using transcription activator–like effector nuclease-mediated homologous recombination, we generated human iPS cell lines that express green fluorescent protein (GFP) in the NPHS1 locus, which encodes nephrin, and we show that GFP expression facilitated accurate visualization of nephrin-positive podocyte formation in -

Hominin-Specific NOTCH2 Paralogs Expand Human Cortical Neurogenesis
bioRxiv preprint doi: https://doi.org/10.1101/221358; this version posted November 17, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Hominin-specific NOTCH2 paralogs expand human cortical neurogenesis through regulation of Delta/Notch interactions. Ikuo K. Suzuki1,2, David Gacquer1, Roxane Van Heurck1,2, Devesh Kumar1,2, Marta Wojno1,2, Angéline Bilheu1,2, Adèle Herpoel1,2, Julian Chéron1,2, Franck Polleux6, Vincent Detours1, and Pierre Vanderhaeghen1,2,3,4,5*. 1 Université Libre de Bruxelles (ULB), Institute for Interdisciplinary Research (IRIBHM), B-1070 Brussels, Belgium 2 ULB Institute of Neuroscience (UNI), B-1070 Brussels, Belgium 3 WELBIO, Université Libre de Bruxelles, B-1070 Brussels, Belgium 4 VIB, Center for Brain and Disease Research, B-3000 Leuven, Belgium 5 University of Leuven (KU Leuven), Department of Neurosciences, B-3000 Leuven, Belgium 6 Department of Neuroscience, Columbia University Medical Center, Columbia University, New York, NY 10027, USA *Correspondence and Lead Contact: [email protected] Keywords Human brain development, human brain evolution, neurogenesis, Notch pathway, cerebral cortex bioRxiv preprint doi: https://doi.org/10.1101/221358; this version posted November 17, 2017. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Summary The human cerebral cortex has undergone rapid expansion and increased complexity during recent evolution. Hominid-specific gene duplications represent a major driving force of evolution, but their impact on human brain evolution remains unclear.