Neurocranium + Splanchnocranium
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD This section aims to cover the non-traumatic pathologies affecting the temporal bone including external auditory canal, middle ear and inner ear which usually need emergent clinical attention. Many of the conditions in this section are secondary to infections in differ- ent clinical settings with resultant complications which may leave temporary or permanent sequelae if not suspected, timely diagnosed or treated. Semin Ultrasound CT MRI 40:116-124 © 2018 Elsevier Inc. All rights reserved. External Auditory Canal There is abnormal soft tissue thickening and enhancement along the margins of the EAC, auricle, and periauricular soft Malignant Otitis Externa tissue. There is effacement of the fat planes around the stylo- his is a more aggressive form of acute otitis externa mastoid foramen and infratemporal fossa5. The involvement T which affects the elderly, diabetic, and immunocompro- of the stylomastoid foramen may result in facial nerve mised patients.1 The term “Malignant” is a misnomer used to involvement. Opacification of middle ear cavity and mastoid describe the aggressive clinical nature and high mortality in air cells are frequently seen (Fig. 1). this condition. It is also referred to as necrotizing otitis If the disease extends inferiorly to involve the subtemporal externa (NOE). In most cases, the causative pathogen is Pseu- soft tissues, parotid, masticator, and parapharyngeal spaces, domonas aeruginosa2 which is not normally found in the imaging will demonstrate abnormal soft tissue enhancement, external acoustic meatus (EAC) but Aspergillus fumigatus is diffuse enlargement of the surrounding muscles, parotid also implicated in immunocompromised patients.3 enlargement, and effacement of the fat planes with or with- The infection begins as an area of granulation at the junc- out abscess. -

Direct Sagittal CT in the Evaluation of Temporal Bone Disease
371 Direct Sagittal CT in the Evaluation of Temporal Bone Disease 1 Mahmood F. Mafee The human temporal bone is an extremely complex structure. Direct axial and coronal Arvind Kumar2 CT sections are quite satisfactory for imaging the anatomy of the temporal bone; Christina N. Tahmoressi1 however, many relationships of the normal and pathologic anatomic detail of the Barry C. Levin2 temporal bone are better seen with direct sagittal CT sections. The sagittal projection Charles F. James1 is of interest to surgeons, as it has the advantage of following the plane of surgical approach. This article describes the advantages of using direct sagittal sections for Robert Kriz 1 1 studying various diseases of the temporal bone. The CT sections were obtained with Vlastimil Capek the aid of a new headholder added to our GE CT 9800 scanner. The direct sagittal projection was found to be extremely useful for evaluating diseases involving the vertical segment of the facial nerve canal, vestibular aqueduct, tegmen tympani, sigmoid sinus plate, sinodural angle, carotid canal, jugular fossa, external auditory canal, middle ear cavity, infra- and supra labyrinthine air cells, and temporo mandibular joint. CT has contributed greatly to an understanding of the complex anatomy and spatial relationship of the minute structures of the hearing and balance organs, which are packed into a small pyramid-shaped petrous temporal bone [1 , 2]. In the past 6 years, high-resolution CT scanning has been rapidly replacing standard tomography and has proved to be the diagnostic imaging method of choice for studying the normal and pathologic details of the temporal bone [3-14]. -

A Morphological Study of Jugular Foramen
Vikas. C. Desai et al /J. Pharm. Sci. & Res. Vol. 9(4), 2017, 456-458 A Morphological Study of Jugular Foramen Vikas. C. Desai1, Pavan P Havaldar2 1. Asst. Prof, Department of Dentistry, BLDE University’s,Shri. B. M. Patil Medical College Hospital and Research Centre,Bijapur – 586103, Karnataka State. 2. Assistant Professor of Anatomy, Gadag Institute of Medical Sciences, Mallasamudra, Mulgund Road, Gadag, Karnataka, India. Abstract Jugular foramen is a large aperture in the base of the skull. It is located behind the carotid canal and is formed by the petrous part of the temporal bone and behind by the occipital bone. The jugular foramen is the main route of venous outflow from the skull and is characterised by laterality based on the predominance of one of the sides. Sigmoid sinus continues as internal jugular vein in posterior part of jugular foramen. Ligation of the internal jugular is sometimes performed during radical neck dissection with the risk of venous infarction, which some adduce to be due to ligation of the dominant internal jugular vein. It is generally said that although the Jugular foramen is larger on the right side compared to the left, its size as well as its height and volume vary in different racial groups and sexes. The foramen’s complex shape, its formation by two bones, and the numerous nerves and venous channels that pass through it further compound its anatomy. The present study was undertaken in 263(526 sides) different medical and dental institutions in Karnataka, India. Out of 263 skulls in 61.21% of cases the right foramina were larger than the left, in 13.68% of cases the left foramina were larger than the right and in 25.09% cases were equal on both sides. -

Anatomic Variations of the Nose and Paranasal Sinuses in Saudi Population
234 Original article Anatomic variations of the nose and paranasal sinuses in saudi population: computed tomography scan analysis Nada Alshaikha, Amirah Aldhuraisb aDepartment of Otolaryngology Head & Neck Background Surgery, Rhinology Unit, Dammam Medical Knowledge of the anatomy constitutes an integral part in the total management of Complex (DMC), bDepartment of ENT, King Fahad Specialist Hospital (KFSH), Dammam, patients with sinonasal diseases. The aim of this study was to obtain the prevalence Saudi Arabia of sinonasal anatomic variations in Saudi population and to understand their importance and impact on the disease process, as well as their influence on Correspondence to Nada Alshaikh, MD, Department of Otorhinolaryngology Head and surgical management and outcome. Neck Surgery, Dammam Medical Complex, Materials and methods Dammam - 31414, Saudi Arabia This study is prospective review of retrospectively performed normal computed e-mail: [email protected] tomography (CT) scans of the nose and paranasal sinuses in adult Saudi Received 13 November 2016 population at Dammam Medical Complex. The scans were reviewed by two Accepted 23 December 2016 independent observers. The Egyptian Journal of Otolaryngology Results 2018, 34:234–241 Of all CT scans that were reviewed, 48.4% were of female patients and 51.6% were of male patients. The mean age of the study sample was 38.5±26.5 years. The most common anatomic variation after excluding agger nasi cell was pneumatized crista galli, which was seen in 73% of the scans. However, the least common variation seen in this series was hypoplasia of the maxillary sinus, which was encountered in 5% of the cases. We did not detect a single pneumatized inferior turbinate among the studied scans. -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -

Neurocranial Histomorphometrics
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Doctoral Dissertations Graduate School 5-2012 Neurocranial Histomorphometrics Lindsay Hines Trammell University of Tennessee-Knoxville, [email protected] Follow this and additional works at: https://trace.tennessee.edu/utk_graddiss Part of the Biological and Physical Anthropology Commons Recommended Citation Trammell, Lindsay Hines, "Neurocranial Histomorphometrics. " PhD diss., University of Tennessee, 2012. https://trace.tennessee.edu/utk_graddiss/1359 This Dissertation is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Doctoral Dissertations by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a dissertation written by Lindsay Hines Trammell entitled "Neurocranial Histomorphometrics." I have examined the final electronic copy of this dissertation for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Doctor of Philosophy, with a major in Anthropology. Murray K. Marks, Major Professor We have read this dissertation and recommend its acceptance: Joanne L. Devlin, David A. Gerard, Walter E. Klippel, David G. Anderson (courtesy member) Accepted for the Council: Carolyn R. Hodges Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) University of Tennessee, Knoxville Trace: Tennessee Research and Creative Exchange Doctoral Dissertations Graduate School 5-2012 Neurocranial Histomorphometrics Lindsay Hines Trammell University of Tennessee-Knoxville, [email protected] This Dissertation is brought to you for free and open access by the Graduate School at Trace: Tennessee Research and Creative Exchange. -

Morphometry of Parietal Foramen in Skulls of Telangana Population Dr
Scholars International Journal of Anatomy and Physiology Abbreviated Key Title: Sch Int J Anat Physiol ISSN 2616-8618 (Print) |ISSN 2617-345X (Online) Scholars Middle East Publishers, Dubai, United Arab Emirates Journal homepage: https://saudijournals.com/sijap Original Research Article Morphometry of Parietal Foramen in Skulls of Telangana Population Dr. T. Sumalatha1, Dr. V. Sailaja2*, Dr. S. Deepthi3, Dr. Mounica Katukuri4 1Associate professor, Department of Anatomy, Government Medical College, Mahabubnagar, Telangana, India 2Assistant Professor, Department of Anatomy, Gandhi Medical College, Secunderabad, Telangana, India 3Assistant Professor, Department of Anatomy, Government Medical College, Mahabubnagar, Telangana, India 4Post Graduate 2nd year, Gandhi Medical College, Secunderabad, Telangana, India DOI: 10.36348/sijap.2020.v03i10.001 | Received: 06.10.2020 | Accepted: 14.10.2020 | Published: 18.10.2020 *Corresponding author: Dr. V. Sailaja Abstract Aims & Objectives: To study the prevalence, number, location and variations of parietal foramen in human skulls and correlate with the clinical significance if any. Material and Methods: A total of 45 skulls with 90 parietal bones were studied in the Department of Anatomy Govt medical college Mahabubnagar from osteology specimens in the academic year 2018-2019.Various parameters like unilateral or bilateral occurance or total absence of the parietal foramen, their location in relation to sagittal suture and lambda, their shape have been observed using appropriate tools and the findings have been tabulate. Observation & Conclusions: Out of total 45 skulls there were 64 parietal foramina in 90 parietal bones, with foramina only on right side in 10 skulls, only on left side in 7 skulls, bilaterally present in 23 skulls, total absence in 4 skulls and 1 foramen located in the sagittal suture. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -
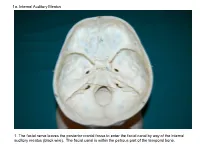
1A. Internal Auditory Meatus
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

The Skull O Neurocranium, Form and Function O Dermatocranium, Form
Lesson 15 ◊ Lesson Outline: ♦ The Skull o Neurocranium, Form and Function o Dermatocranium, Form and Function o Splanchnocranium, Form and Function • Evolution and Design of Jaws • Fate of the Splanchnocranium ♦ Trends ◊ Objectives: At the end of this lesson, you should be able to: ♦ Describe the structure and function of the neurocranium ♦ Describe the structure and function of the dermatocranium ♦ Describe the origin of the splanchnocranium and discuss the various structures that have evolved from it. ♦ Describe the structure and function of the various structures that have been derived from the splanchnocranium ♦ Discuss various types of jaw suspension and the significance of the differences in each type ◊ References: ♦ Chapter: 9: 162-198 ◊ Reading for Next Lesson: ♦ Chapter: 9: 162-198 The Skull: From an anatomical perspective, the skull is composed of three parts based on the origins of the various components that make up the final product. These are the: Neurocranium (Chondocranium) Dermatocranium Splanchnocranium Each part is distinguished by its ontogenetic and phylogenetic origins although all three work together to produce the skull. The first two are considered part of the Cranial Skeleton. The latter is considered as a separate Visceral Skeleton in our textbook. Many other morphologists include the visceral skeleton as part of the cranial skeleton. This is a complex group of elements that are derived from the ancestral skeleton of the branchial arches and that ultimately gives rise to the jaws and the skeleton of the gill -

Non Metric Traits of the Skull and Their Role in Anthropological Studies
Original article Non metric traits of the skull and their role in anthropological studies Kaur, J.1*, Choudhry, R.2, Raheja, S.3 and Dhissa, NC.4 1Doctor, Master of Science in Anatomy, Assistant Professor, Department of Anatomy, ESIC Dental College, Rohini, New Delhi 2Doctor, Master of Science in Anatomy, Ex Head of the Department of Anatomy, VMMC & Safdarjung Hospital, New Delhi 3Doctor, Master of Science in Anatomy, Professor, Department of Anatomy, Lady Hardinge Medical College, New Delhi 4Doctor, Master of Science in Anatomy, Associate Professor, Department of Anatomy, ESIC Dental College, New Delhi *E-mail: [email protected] Abstract Anthropological and paleoanthropological studies concerning the so called epigenetic cranial traits or non-metrical cranial traits have been increasing in frequency in last ten years. For this type of study, the trait should be genetically determined, vary in frequency between different populations and should not show age, sex and side dependency. The present study was conducted on hundred dry adult human skulls from Northern India. They were sexed and classified into groups of various non metrical traits. These traits were further studied for sexual and side dimorphism. None of the traits had shown statistically significant side dimorphism. Two of them (Parietal foramen and Exsutural mastoid foramen) however had shown statistically significant sexual dimorphism. Since the dimorphism is exhibited by very less number of traits, it can be postulated that these traits are predominantly under genetic control and can be effectively used for population studies. Keywords: double hypoglossal canal, epigenetic variants, non-metric cranial variants, supraorbital foramen, zygomaticofacial foramen. 1 Introduction 2 Material and methods Anthropological and paleoanthropological studies Hundred dry adult human skulls from Northern India, concerned with the epigenetic traits or non-metrical cranial having no deformity or fracture were examined.