Fetal Membranes and Placenta
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

3 Embryology and Development
BIOL 6505 − INTRODUCTION TO FETAL MEDICINE 3. EMBRYOLOGY AND DEVELOPMENT Arlet G. Kurkchubasche, M.D. INTRODUCTION Embryology – the field of study that pertains to the developing organism/human Basic embryology –usually taught in the chronologic sequence of events. These events are the basis for understanding the congenital anomalies that we encounter in the fetus, and help explain the relationships to other organ system concerns. Below is a synopsis of some of the critical steps in embryogenesis from the anatomic rather than molecular basis. These concepts will be more intuitive and evident in conjunction with diagrams and animated sequences. This text is a synopsis of material provided in Langman’s Medical Embryology, 9th ed. First week – ovulation to fertilization to implantation Fertilization restores 1) the diploid number of chromosomes, 2) determines the chromosomal sex and 3) initiates cleavage. Cleavage of the fertilized ovum results in mitotic divisions generating blastomeres that form a 16-cell morula. The dense morula develops a central cavity and now forms the blastocyst, which restructures into 2 components. The inner cell mass forms the embryoblast and outer cell mass the trophoblast. Consequences for fetal management: Variances in cleavage, i.e. splitting of the zygote at various stages/locations - leads to monozygotic twinning with various relationships of the fetal membranes. Cleavage at later weeks will lead to conjoined twinning. Second week: the week of twos – marked by bilaminar germ disc formation. Commences with blastocyst partially embedded in endometrial stroma Trophoblast forms – 1) cytotrophoblast – mitotic cells that coalesce to form 2) syncytiotrophoblast – erodes into maternal tissues, forms lacunae which are critical to development of the uteroplacental circulation. -

Management of Patent Vitellointestinal Duct in Infants
Published online: 2021-02-17 94 OriginalPatent Vitellointestinal Article Duct Ghritlaharey Management of Patent Vitellointestinal Duct in Infants Rajendra K. Ghritlaharey1 1Department of Paediatric Surgery, Gandhi Medical College and Address for correspondence Rajendra K. Ghritlaharey, MS, MCh, Associated Kamla Nehru and Hamidia Hospital, Bhopal, Madhya FAIS, MAMS, DLitt, Department of Paediatric Surgery, Gandhi Medical Pradesh, India College and Associated Kamla Nehru and Hamidia Hospitals, Bhopal 462001, Madhya Pradesh, India (e-mail: [email protected]). Ann Natl Acad Med Sci (India) 2021;57:94–99. Abstract Objectives This study was undertaken to investigate and review the clinical presen- tation, surgical procedures executed, and the final outcome of infants managed for the patent vitellointestinal duct. Materials and Methods This is a single-institution, retrospective study and included infants who were operated for the patent vitellointestinal duct. This study was conducted at author’s Department of Paediatric Surgery during the last 20 years; from January 1, 2000 to December 31, 2019. Results A total of 24 infants were operated for the patent vitellointestinal duct during the study period and comprised 20 (83.3%) boys and 4 (16.6%) girls. The age of infants ranged from 7 days to 10 months, with a mean of 88.41 ± 64.9 days. Twenty-three (95.8%) infants were operated within 6 months of the age, 17 (70.8%) of them were operated within 3 months of the age. Only one (4.1%) infant was operated at the age of 10 months. Among 24 infants, 13 (54.1%) were presented with features suggestive of acute intestinal obstruction and remaining 11 (45.8%) were presented with fecal discharges through the umbilicus without intestinal obstruction. -

Download/Rozdzial05.Pdf (Accessed on 1 January 2007)
cancers Article Early Alcohol Use Initiation, Obesity, Not Breastfeeding, and Residence in a Rural Area as Risk Factors for Breast Cancer: A Case-Control Study Dorota Anna Dydjow-Bendek * and Paweł Zagozd˙ zon˙ Department of Hygiene and Epidemiology, Medical University of Gdansk, 80-211 Gdansk, Poland; [email protected] * Correspondence: [email protected] Simple Summary: Breast cancer became the most common cancer globally in 2021, according to the World Health Organization. The aim of the study was to evaluate risk factors for breast cancer, such as early alcohol use initiation, obesity, breastfeeding, and place of residence. The effect of alcohol consumption by girls has been assessed in only a few studies and is not fully understood. In this study, it has been found to be associated with a higher risk of breast cancer. Our study also shed light on the incidence disparity—women were more at risk in the countryside than in the city. The results of this study should be included in the preparation of breast cancer prevention programs and also aimed at women in adolescence and early adulthood because exposures during childhood and adolescence can affect a woman’s long-term risk of breast cancer. Every effort should also be made to ensure that access to knowledge is open to all, regardless of where they live, giving all women equal opportunities. Citation: Dydjow-Bendek, D.A.; Zagozd˙ zon,˙ P. Early Alcohol Use Abstract: Initiation, Obesity, Not Breastfeeding, The aim of this study was to determine the risk factors for breast cancer in the Polish and Residence in a Rural Area as Risk population. -
PRG2 and AQPEP Are Misexpressed in Fetal Membranes in Placenta Previa and Percreta Elisa T. Zhang1, Roberta L. Hannibal1,6, Keyl
bioRxiv preprint doi: https://doi.org/10.1101/2020.08.14.248807; this version posted August 14, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. 1 PRG2 and AQPEP are misexpressed in fetal membranes in placenta previa and percreta 2 3 Elisa T. Zhang1, Roberta L. Hannibal1,6, Keyla M. Badillo Rivera1,7, Janet H.T. Song1,8, Kelly 4 McGowan1, Xiaowei Zhu1,2, Gudrun Meinhardt3, Martin Knöfler3, Jürgen Pollheimer3, Alexander 5 E. Urban1,2, Ann K. Folkins4, Deirdre J. Lyell5, Julie C. Baker1,5* 6 7 1DepartMent of Genetics, Stanford University School of Medicine, Stanford, California, United 8 States of AMerica. 9 2DepartMent of Psychiatry and Behavioral Sciences, Stanford University School of 10 Medicine, Stanford, California, United States of AMerica. 11 3DepartMent of Obstetrics and Gynaecology, Reproductive Biology Unit, Medical University of 12 Vienna, Vienna, Austria. 13 4DepartMent of Pathology, Stanford University School of Medicine, Stanford, California, United 14 States of AMerica. 15 5DepartMent of Obstetrics and Gynecology, Stanford University School of Medicine, Stanford, 16 California, United States of AMerica. 17 6Present address: Second GenoMe, Inc., Brisbane, California, United States of AMerica. 18 7Present address: Eversana Consulting, South San Francisco, California, United States of 19 AMerica. 20 8Present address: Division of Genetics and GenoMics, Boston Children’s Hospital, Harvard 21 Medical School, Boston, Massachusetts, United States of AMerica. 22 23 *Correspondence: [email protected] 24 300 Pasteur Dr. -

Extremely Rare Presentation of an Omphalomesenteric Cyst in a 61-Year-Old Patient
Turk J Surg 2017; 33: 43-44 Case Report DOI: 10.5152/UCD.2014.2748 Extremely rare presentation of an omphalomesenteric cyst in a 61-year-old patient Recep Aktimur1, Uğur Yaşar2, Elif Çolak1, Nuraydın Özlem1 ABSTRACT The umbilicus is remaining scar tissue from the umbilical cord in the fetus. If the omphalomesenteric duct in the umbilicus is not properly closed, an ileal-umbilical fistula, sinus formation, cysts, or, most commonly, Meckel’s di- verticulum can develop. The others are very rare and mostly occur in the pediatric population. We describe herein a 61-year-old female with a giant omphalomesenteric cyst presented as an asymptomatic infraumbilical mass. To our knowledge, this is the oldest patient reported and the largest cyst described in the literature. The diagnosis of a painless abdominal mass frequently suggests malignancy in older patients. But, extremely rare conditions can be detected, such as an omphalomesenteric cyst. Keywords: Adult, anomaly, cyst, duct, omphalomesenteric INTRODUCTION The umbilicus is remaining scar tissue from the umbilical cord in the fetus. It contains the urachus, om- phalomesenteric duct, and the round ligament’s embryonic remnants, which can be a source of many clinical problems. Also, umbilical hernia can occur in cases of closure defects of the umbilical ring. If the omphalomesenteric duct is not properly closed, an ileal-umbilical fistula, sinus formation, cysts, or Meckel’s diverticulum can develop. Meckel’s diverticulum is the most common omphalomesenteric duct anomaly, and it is also the most common congenital abnormality of the gastrointestinal tract (2%). Other anomalies associated with the omphalomesenteric duct are very rare and mostly occur in the pediatric population. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

Self-Organized Amniogenesis by Human Pluripotent Stem Cells in a Biomimetic Implantation-Like Niche
LETTERS PUBLISHED ONLINE: 12 DECEMBER 2016 | DOI: 10.1038/NMAT4829 Self-organized amniogenesis by human pluripotent stem cells in a biomimetic implantation-like niche Yue Shao1†, Kenichiro Taniguchi2†, Katherine Gurdziel3, Ryan F. Townshend2, Xufeng Xue1, Koh Meng Aw Yong1, Jianming Sang1, Jason R. Spence2, Deborah L. Gumucio2* and Jianping Fu1,2,4* Amniogenesis—the development of amnion—is a critical factors seen in the in vivo amniogenic niche: a three-dimensional developmental milestone for early human embryogenesis (3D) extracellular matrix (ECM) that is provided by the basement and successful pregnancy1,2. However, human amniogenesis membrane surrounding the epiblast during implantation11; and a is poorly understood due to limited accessibility to peri- soft tissue bed provided by the uterine wall and trophoblast to implantation embryos and a lack of in vitro models. Here support the developing amnion (Fig. 1a,b). Since amniogenesis ini- we report an ecient biomaterial system to generate human tiates from the expanding pluripotent epiblast, we utilized mTeSR1 amnion-like tissue in vitro through self-organized development medium and basement membrane matrix (Geltrex) to render the of human pluripotent stem cells (hPSCs) in a bioengineered culture permissive for pluripotency maintenance. niche mimicking the in vivo implantation environment. We In this culture system, H9 human embryonic stem cells (hESCs) show that biophysical niche factors act as a switch to toggle were plated as single cells at 30,000 cells cm−2 onto a thick, hPSC self-renewal versus amniogenesis under self-renewal- soft gel bed of Geltrex (with thickness ≥100 µm, bulk Young's permissive biochemical conditions. We identify a unique modulus ∼900 Pa, coated on a glass coverslip), in mTeSR1 medium molecular signature of hPSC-derived amnion-like cells and supplemented with the ROCK inhibitor Y27632 (Fig. -

BMP-Treated Human Embryonic Stem Cells Transcriptionally Resemble Amnion Cells in the Monkey Embryo
bioRxiv preprint doi: https://doi.org/10.1101/2021.01.21.427650; this version posted January 22, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. BMP-treated human embryonic stem cells transcriptionally resemble amnion cells in the monkey embryo Sapna Chhabra1,2,3, Aryeh Warmflash2,4* 1Systems Synthetic and Physical Biology graduate program, 2Department of Biosciences, 4Department of Bioengineering, Rice University, Houston, TX 77005 3Present address: Developmental Biology Unit, EMBL Heidelberg. *Correspondence to AW: [email protected] Abstract Human embryonic stem cells (hESCs) possess an immense potential to generate clinically relevant cell types and unveil mechanisms underlying early human development. However, using hESCs for discovery or translation requires accurately identifying differentiated cell types through comparison with their in vivo counterparts. Here, we set out to determine the identity of much debated BMP-treated hESCs by comparing their transcriptome to the recently published single cell transcriptomes of early human embryos in the study Xiang et al 2019. Our analyses reveal several discrepancies in the published human embryo dataset, including misclassification of putative amnion, intermediate and inner cell mass cells. These misclassifications primarily resulted from similarities in pseudogene expression, highlighting the need to carefully consider gene lists when making comparisons between cell types. In the absence of a relevant human dataset, we utilized the recently published single cell transcriptome of the early post implantation monkey embryo to discern the identity of BMP-treated hESCs. -

Folding of Embryo
❑There is progressive increase in the size of the embryonic disc due to rapid growth of cells of central part of embryonic disc and rapid growth of somites. ❑ This causes conversion of flat pear-shaped germ disc into a cylindrical embryo. ❑The head and tail ends of the disc remain relatively close together.The increased length of the disc causes it to bulge upward into the amniotic cavity. ❑With the formation of the head and tail folds, parts of the yolk sac become enclosed within the embryo. ❑ In this way, a tube lined by endoderm is formed in the embryo. This is the primitive gut, from which most of the gastrointestinal tract is derived. ❑ At first, the gut is in wide communication with the yolk sac. The part of the gut cranial to this communication is called the foregut; the part caudal to the communication is called the hindgut; while the intervening part is called the midgut . ❑The communication with the yolk sac becomes progressively narrower. As a result of these changes, the yolk sac becomes small and inconspicuous, and is now termed the definitive yolk sac (also called the umbilical vesicle). ❑The narrow channel connecting it to the gut is called the vitellointestinal duct (also called vitelline duct; yolk stalk or omphalomesenteric duct). This duct becomes elongated and eventually disappears. ❑With the formation of the cavity, the embryo (along with the amniotic cavity and yolk sac) remains attached to the trophoblast only by extraembryonic mesoderm into which the coelom does not exist. This extraembryonic mesoderm forms the connecting stalk. -

The Science of Amnioexcite™ Three Layer Placental Membrane Allograft
The Science of AmnioExcite™ Three Layer Placental Membrane Allograft REV. 10-2020 The Science of AmnioExcite™ Placental Membrane Allograft AmnioExcite™ is a full-thickness decellularized placental membrane. AmnioExcite™ is a lyophilized, full-thickness placental membrane allograft decellularized with LifeNet Health’s proprietary Matracell® process and patent pending technology and intended for homologous use as a barrier membrane.(1) Inclusion of the intact amniotic and chorionic membranes, as well as the trophoblast layer, makes it thicker than most available amniotic-only or amniotic-chorionic allografts, and provides a robust protective covering while also delivering superior handling. AmnioExcite™ retains the placental membrane’s naturally occurring growth factors, cytokines, protease inhibitors, and extracellular matrix components, such as proteoglycans, collagen and fibronectin(2) In vitro studies have shown that these endogenous factors are capable of inducing cellular proliferation and migration, mitigating inflammation, and inhibiting protein degradation(3-5) STRUCTURE OF THE THREE LAYER PLACENTAL MEMBRANE AMNIOTIC MEMBRANE CHORIONIC MEMBRANE TROPHOBLAST LAYER The placental membrane is comprised of the amnion and chorion (6). The amnion, also called amniotic membrane (AM) has five layers, including the epithelium, basement membrane, compact layer, fibroblast layer, and the spongy layer(6), which provide important extracellular membrane components, as well as a wide variety of growth factors, cytokines, and other proteins.(7) While these characteristics are important, the AM by itself lacks substantial structure for providing a protective covering and contains only a small portion of the biological factors found in the full-thickness placental membrane. AM-only grafts can also be difficult to apply and may migrate away from the intended site of application.(8) The chorion is comprised of four layers, including the cellular layer, reticular layer, the pseudobasement membrane and the trophoblast layer (TL) (6). -
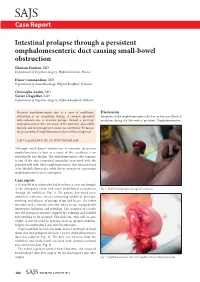
Intestinal Prolapse Through a Persistent Omphalomesenteric Duct
SAJS Case Report Intestinal prolapse through a persistent omphalomesenteric duct causing small-bowel obstruction Ghislain Pauleau, MD Department of Digestive Surgery, Hôpital Laveran, France Diane Commandeur, MD Department of Anaesthesiology, Hôpital Bouffard, Djibouti Christophe Andro, MD Xavier Chapellier, MD Department of Digestive Surgery, Hôpital Bouffard, Djibouti Persistent omphalomesenteric duct as a cause of small-bowel Discussion obstruction is an exceptional finding. A neonate presented Anomalies in the omphalomesenteric duct occur because of lack of with occlusion due to intestinal prolapse through a persistent involution during the 9th week of gestation. Omphalomesenteric omphalomesenteric duct. Remnants of the duct were successfully resected, and the postoperative course was uneventful. We discuss the presentation of omphalomesenteric duct and its management. S Afr J Surg 2012;50(3):102-103. DOI:7196/SAJS.1289 Although small-bowel obstruction is common, persistent omphalomesenteric duct as a cause of this condition is an exceptionally rare finding. The omphalomesenteric duct remnant is one of the rare congenital anomalies associated with the primitive yolk stalk. Most omphalomesenteric duct remnants tend to be Meckel’s diverticula, while the occurrence of a persistent omphalomesenteric duct is infrequent. Case report A 20-day-old male infant who had been born at term was brought to the emergency room with acute small-bowel evisceration Fig. 1. Small-bowel prolapse through the umbilicus. through the umbilicus (Fig. 1). His parents had noted peri- umbilical erythema, mucus-containing umbilical drainage, vomiting, and absence of passage of gas and faeces. The infant was taken to the intensive care unit, where he was managed with intravenous hydration and refeeding. -
Substance Use in Pregnancy
MAY 2017 SUBSTANCE USE IN PREGNANCY Prepared By: Aaron Fields, MD University of Rochester Medical Center, NYS Maternal & Infant Health Center of Excellence 265 Crittenden Blvd, Rochester, NY 14642 – Tel: 585-276-7893 – Fax: 585-461-4532 [email protected] – www.mihcoe.org Introduction ..............................................................................................................................................................2 What is Addiction? .....................................................................................................................................................3 Drugs of Abuse ..........................................................................................................................................................4 Opioids ................................................................................................................................................................................ 4 Stimulants ........................................................................................................................................................................... 4 Nicotine............................................................................................................................................................................... 5 Alcohol ................................................................................................................................................................................ 6 Marijuana ...........................................................................................................................................................................