Use of the Biceps Femoris Following Failed Inferior Gluteal Flap Transfer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Intramuscular Injection Is an Injection Given Directly Into The
Depo Lupron and Testosterone are both given by intramuscular injection. The following is a guideline on their administration. Eileen Durham, RN, NP Version 12 Jan 2010 Description Intramuscular (IM) injections are given directly into the central area of selected muscles. There are a number of sites that are suitable for IM injections; there are three sites that are most commonly used in this procedure described below. The volume of viscosity of the medication to be injected determines the site that should be used. IM injections cause stretching of the muscle fiber so the larger the muscle used the less discomfort. Intramuscular Injection Sites Depo Lupron Depo Lupron 3 month preparation should only be injected into the Gluteus medius due to the viscosity and volume of the medication approx. 1.5 – 2 cc. Depo Lupron 1 month preparation can be injection into the vastus lateralis or the gluteus medius. Testosterone Testosterone administered to adolescents and adults can be injected into any of the sites listed below, as long as the volume is 1 cc or less. For a volume of 1.5 use the vastus lateralis or Gluteus medius, if the volume is 2 cc you must you the largest muscle the Gluteus medius. If the volume is greater then 2 cc you must divide the dose and give 2 injections as the maximum volume in the Gluteal muscle is 2 cc. Testosterone administered to infants and toddlers use only the anteriolateral aspect of the thigh. Deltoid muscle The deltoid muscle located laterally on the upper arm can be used for intramuscular injections. -
Bacterial Meningitis and Multiple Abscess Formation in the Iliopsoas
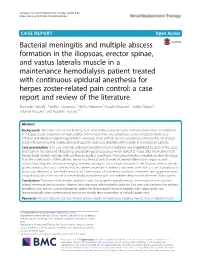
Yamada et al. Renal Replacement Therapy (2018) 4:22 https://doi.org/10.1186/s41100-018-0163-x CASEREPORT Open Access Bacterial meningitis and multiple abscess formation in the iliopsoas, erector spinae, and vastus lateralis muscle in a maintenance hemodialysis patient treated with continuous epidural anesthesia for herpes zoster-related pain control: a case report and review of the literature Shunsuke Yamada1, Narihito Tatsumoto1, Noriko Nakamura1, Kosuke Masutani1, Toshiro Maeda2, Takanari Kitazono1 and Kazuhiko Tsuruya1,3* Abstract Background: Infection is the second leading cause of mortality in patients who undergo maintenance hemodialysis. In this population, impairment in both cellular and humoral immunity contributes to the increased incidence of infection and infection-related hospitalization. However, these artificial devices occasionally enhance the risk of deep organ infection including muscle abscess, frequently leading to disability and mortality in hemodialysis patients. Case presentation: A 54-year-old male undergoing maintenance hemodialysis was hospitalized because of the acute onset pain in the back and bilateral legs and declining consciousness which started at 7 days after the treatment of herpes zoster-related neuralgia with continuous epidural anesthesia. Physical examination revealed purulent discharge from the insertion site of the catheter. Serum biochemical tests showed increased inflammatory response and malnutrition. Magnetic resonance imaging revealed meningitis and multiple abscesses in the iliopsoas, erector spinae, gluteus medius, and vastus lateralis muscles, where conventional antibiotic treatment often fails to cure. Staphylococcus aureus was detected in the cerebrospinal fluid. Combination of intravenous antibiotics treatment and aggressive open surgical drainage of the muscle abscesses finally cured meningitis and multiple deep muscle abscesses in this patient. -

The Anatomy of the Posterolateral Aspect of the Rabbit Knee
Journal of Orthopaedic Research ELSEVIER Journal of Orthopaedic Research 2 I (2003) 723-729 www.elsevier.com/locate/orthres The anatomy of the posterolateral aspect of the rabbit knee Joshua A. Crum, Robert F. LaPrade *, Fred A. Wentorf Dc~~ur/niiviiof Orthopuer/ic Surgery. Unicrrsity o/ Minnesotu. MMC 492, 420 Dcluwur-c Si. S. E., Minnwpoli,s, MN 55455, tiSA Accepted 14 November 2002 Abstract The purpose of this study was to determine the anatomy of the posterolateral aspect of the rabbit knee to serve as a basis for future in vitro and in vivo posterolateral knee biomechanical and injury studies. Twelve nonpaired fresh-frozen New Zealand white rabbit knees were dissected to determine the anatomy of the posterolateral corner. The following main structures were consistently identified in the rabbit posterolateral knee: the gastrocnemius muscles, biceps femoris muscle, popliteus muscle and tendon, fibular collateral ligament, posterior capsule, ligament of Wrisberg, and posterior meniscotibial ligament. The fibular collateral ligament was within the joint capsule and attached to the femur at the lateral epi- condyle and to the fibula at the midportion of the fibular head. The popliteus muscle attached to the medial edge of the posterior tibia and ascended proximally to give rise to the popliteus tendon, which inserted on the proximal aspect of the popliteal sulcus just anterior to the fibular collateral ligament. The biceps femoris had no attachment to the fibula and attached to the anterior com- partment fascia of the leg. This study increased our understanding of these structures and their relationships to comparative anatomy in the human knee. -

Thieme: an Illustrated Handbook of Flap-Raising Techniques
4 Part 1 Flaps of the Upper Extremity Chapter 1 dyle are palpated and marked. A straight line is The Deltoid Fasciocutaneous Flap marked to connect these two landmarks. The groove between the posterior border of the del- toid muscle and the long head of triceps is pal- pated and marked. The intersection of these two lines denotes approximately the location of the vascular pedicle, as it emerges from under- The deltoid free flap is a neurovascular fascio- neath the deltoid muscle. This point may be cutaneous tissue, providing relatively thin sen- studied with a hand-held Doppler and marked sate tissue for use in soft-tissue reconstruction. if required. The deltoid fasciocutaneous flap was first de- Depending on the recipient area, the patient scribed anatomically and applied clinically by is positioned either supine, with the donor Franklin.1 Since then, the deltoid flap has been shoulder sufficiently padded with a stack of widely studied and applied.2–5 This flap is sup- towels, or in the lateral decubitus position. Myo- plied by a perforating branch of the posterior relaxants are required in muscular individuals, circumflex humeral artery and receives sensa- so as to ease retraction of the posterior border tion by means of the lateral brachial cutaneous of the deltoid muscle, especially if a long vascu- nerve and an inferior branch of the axillary lar pedicle is required for reconstruction. nerve. This anatomy is a constant feature, thus making the flap reliable. The ideal free deltoid Neurovascular Anatomy flap will be thin, hairless, of an adequate size, and capable of sensory reinnervation. -

Strain Assessment of Deep Fascia of the Thigh During Leg Movement
Strain Assessment of Deep Fascia of the Thigh During Leg Movement: An in situ Study Yulila Sednieva, Anthony Viste, Alexandre Naaim, Karine Bruyere-Garnier, Laure-Lise Gras To cite this version: Yulila Sednieva, Anthony Viste, Alexandre Naaim, Karine Bruyere-Garnier, Laure-Lise Gras. Strain Assessment of Deep Fascia of the Thigh During Leg Movement: An in situ Study. Frontiers in Bioengineering and Biotechnology, Frontiers, 2020, 8, 15p. 10.3389/fbioe.2020.00750. hal-02912992 HAL Id: hal-02912992 https://hal.archives-ouvertes.fr/hal-02912992 Submitted on 7 Aug 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. fbioe-08-00750 July 27, 2020 Time: 18:28 # 1 ORIGINAL RESEARCH published: 29 July 2020 doi: 10.3389/fbioe.2020.00750 Strain Assessment of Deep Fascia of the Thigh During Leg Movement: An in situ Study Yuliia Sednieva1, Anthony Viste1,2, Alexandre Naaim1, Karine Bruyère-Garnier1 and Laure-Lise Gras1* 1 Univ Lyon, Université Claude Bernard Lyon 1, Univ Gustave Eiffel, IFSTTAR, LBMC UMR_T9406, Lyon, France, 2 Hospices Civils de Lyon, Hôpital Lyon Sud, Chirurgie Orthopédique, 165, Chemin du Grand-Revoyet, Pierre-Bénite, France Fascia is a fibrous connective tissue present all over the body. -

Applications of the Pedicled Vastus Lateralis Flap for Patients with Complicated Pressure Sores
Spinal Cord (1997) 35, 437 ± 442 1997 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/97 $12.00 Applications of the pedicled vastus lateralis ¯ap for patients with complicated pressure sores AB Schmidt1, G Fromberg1 and M-H Ruidisch2 1Abt. fuÈr Plastische-, Hand-, Kiefer- und rekonstruktive Mikrochirurgie, BG Unfallklinik Murnau; 2Abt. fuÈr RuÈckenmark- und WirbelsaÈulenverletztungen, BG Unfallklinik Murnau, Germany The vastus lateralis muscle- or musculocutaneous ¯ap is a well established tool in the surgery of pressure sores of the pelvic region. Its size, its constant large axial vascular pedicle originating from the lateral circum¯ex femoral artery, and its ability to carry quite a large skin island from the distal lateral region of the upper thigh makes this ¯ap a very versatile one in the management of dicult situations. The vastus lateralis ¯ap allows the simultaneous closure of defects in the trochanteric and sacral region, a technique which has not been described previously. A pedicled vastus lateralis ¯ap may be the only remaining local salvage procedure for defects due to obstruction of internal and external iliac arteries and aortobifemoral bypass surgery. This is another application which has not yet been described in the medical literature. The outcome of a series of 38 vastus lateralis ¯aps and the complications are shown. The follow-up period ranged from 3 months to 4 years. One ¯ap was lost. More complications were seen at the donor site than at the reconstructed defect. In patients who may be able to walk or stand at a later date, potential impairment of these functions has to be considered. -

The Role of and Relationship Between Hamstring and Quadriceps Muscle Myofascial Trigger Points in Patients with Patellofemoral Pain Syndrome
The role of and relationship between Hamstring and Quadriceps muscle myofascial trigger points in patients with patellofemoral pain syndrome. By Karen Louise Frandsen Smith A mini-dissertation submitted in partial compliance with the requirements for the Master’s Degree in Technology: Chiropractic at the Durban University of Technology I, Karen Louise Frandsen Smith, declare that this dissertation is representative of my own work in both conception and execution (except where acknowledgements indicate to the contrary). _______________________ ________________ Karen Louise Frandsen Smith Date Approved for Submission _______________________ ________________ Dr Brian Kruger (supervisor) Date M. Tech. Chiro., C.C.S.P. Dedication I dedicate this work to everyone who loves me and have supported me throughout these years of studying and all the difficult times. It is thanks to you that I have reached my dream. Dad, you would be so proud. i Acknowledgements Thank you to the DUT staff, patients, and supervisor, Dr Brian Kruger for making this happen. Thanks to my class mates for making the years fly by, and creating lifelong memories. This dissertation would not have been completed without supportive, generous and helpful people. Special thanks to you, Dr Danella Lubbe for motivating me and thank you so much Dr Charmaine Korporaal for “picking me up” and helping me finish. Endless gratitude goes to you Damon, Cherine, Mom and Viggo. You are / were all my anchors in the storm, and without your belief in me, I would be nowhere. ii Abstract Purpose: Patellofemoral Pain Syndrome is a common condition in all age groups, with a multi- factorial etiology. -

The Fascia Lata of the Thigh – More Than a “Stocking”: a Magnetic Resonance Imaging, Ultrasonography and Dissection Study
The Fascia Lata of the Thigh – More Than a “Stocking”: A Magnetic Resonance Imaging, Ultrasonography and Dissection Study. Willem Fourie. School of Anatomical Sciences, University of the Witwatersrand, 7 York Road, Parktown 2193, Johannesburg, South Africa. Phone: +27 (0)11 763 6990. Fax: +27 (0)866 180 179. E-mail: [email protected] BACKROUND: Regional descriptions of the thigh mostly exclude detailed descriptions of the fascia lata and its relationships to underlying muscles. It is cursorily described as “a strong, dense, broad single layer of deep fascia investing the thigh muscles like a stocking”. This “stocking” contributes to increased compartment pressure when the muscles contract, aiding venous return. With recent growing understanding of the role of deep fascia, it seems like the fascia lata may not solely be for compartmentalisation, containment and aiding venous return. OBSERVATIONS: During dissections of cadaver thighs, we observed that the fascial relations to underlying muscles differ from textbook descriptions, forming a separate fascia covering some muscles, while acting as an epimysial cover to others in the same region. Furthermore, in an ultrasonography (US) pilot study, some regions of the upper thigh appeared as a triple layer of fascia covering muscles. Both these observations contradicted the general descriptions in literature. AIMS: 1. To investigate the above observations further. 2. Comparing dissection observations and living subjects using magnetic resonance imaging (MRI) and ultrasonography (US). METHODS: Detailed dissection of eight cadaver thighs compared to observations from MRI and US of four living subjects’ thighs. Observations were done at the same four levels on all the thighs. RESULTS: While vastus lateralis observations corresponded to textbook descriptions, US showed the fascia lata as a triple layer in places. -

Chapter 10 the Knee Joint
The Knee Joint • Knee joint – largest joint in body Chapter 10 – very complex The Knee Joint – primarily a hinge joint Manual of Structural Kinesiology Modified for Prentice WE: Arnheim’s principles of athletic training , ed 12, New R.T. Floyd, EdD, ATC, CSCS York, 2006, McGraw-Hill; from Saladin, KS: Anatomy &physiology: the unity of forms and function , ed 2, New York, 2001, McGraw- Hill. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-1 © 2007 McGraw-Hill Higher Education. All rights reserved. 10-2 Bones Bones • Enlarged femoral condyles articulate on • Fibula - lateral enlarged tibial condyles – serves as the attachment for • Medial & lateral tibial condyles (medial & knee joint lateral tibial plateaus) - receptacles for structures femoral condyles – does not articulate • Tibia – medial with femur or patella – bears most of weight – not part of knee joint Modified from Anthony CP, Kolthoff NJ: Textbook of anatomy and physiology , ed 9, St. Louis, 1975, Mosby. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-3 © 2007 McGraw-Hill Higher Education. All rights reserved. 10-4 Bones Bones • Patella • Key bony landmarks – sesamoid (floating) bone – Superior & inferior patellar poles – imbedded in quadriceps – Tibial tuberosity & patellar tendon – Gerdy’s tubercle – serves similar to a pulley – Medial & lateral femoral in improving angle of condyles pull, resulting in greater – Upper anterior medial tibial mechanical advantage in surface – Head of fibula knee extension Modified from Anthony CP, Kolthoff NJ: Textbook of anatomy and physiology , ed 9, St. Louis, 1975, Mosby. © 2007 McGraw-Hill Higher Education. All rights reserved. 10-5 © 2007 McGraw-Hill Higher Education. All rights reserved. -
Structural Kinesiology Class 11
STRUCTURAL KINESIOLOGY CLASS 11 With John Maguire WHAT WE WILL COVER IN THIS CLASS Muscles of the Large Intestine: • Fascia Lata • Hamstrings • Lumborum The Emergency Mode 2 FASCIA LATA MUSCLE PAGE 224 Meridian Large Intestine Organ Large Intestine Action Flexes, medially rotates and abducts the hip. Origin Iliac crest posterior to the ASIS Insertion Iliotibial band Muscle Test The supine person holds the leg in a position of abduction, internal rotation, and hip flexion with the knee in hyperextension. Push the leg down and in towards the other ankle NL Top of the thigh to below the knee cap along the iliotibial band Back: a triangle from L2 – L4 on the soft tissue in the back NV #10 Parietal Eminence Indications • Intestinal problems of constipation, spastic colon, colitis and diarrhea, • Chest soreness and breast pain with menstruation. • Postural sign is the legs tend to bow 3 HAMSTRINGS PAGE 226 Meridian Large Intestine Organ Large Intestine – particularly the rectum Action Biceps Femoris (lateral hamstring) – Flexes the knee, laterally rotates the hip and the flexed knee and extends the hip. Semitendinosus and Semimembranosus (medial hamstrings) Flexes the knee, medially rotates the hip and extends the hip. Origin Ischial tuberosity and the back middle of the femur Insertion Biceps Femoris – Head of the fibula. Semitendinosus – top inside of the tibia Semimembranosus – back of the medial condyle of the tibia Muscle Test With the leg bent so the angle of the calf and the thigh is slightly more than 90 degrees, exert pressure in the middle of the hamstring to prevent cramping. Pressure is against the back of the achilles tendon to straighten the leg. -
Peroneal Nerve Compression Secondary to an Anomalous Biceps Femoris Muscle in an Adolescent Athlete Kevin M
(aspects of sports medicine • a case report) Peroneal Nerve Compression Secondary to an Anomalous Biceps Femoris Muscle in an Adolescent Athlete Kevin M. Kaplan, MD, Abhay Patel, MD, and Drew A. Stein, MD ABSTRACT compression can present a consid- 3/5, with all other muscle groups Common peroneal nerve compres- erable challenge. Other conditions 5/5. Sensation was significantly sion is a well-recognized entity must be excluded in order to make decreased at the first dorsal web that can cause severe debilitating the proper diagnosis.3 Symptoms space and the dorsal lateral foot. clinical manifestations. The cur- can occur after exercise, can develop Pulses were intact, and all reflexes rent literature describes numerous gradually after a period of training, were 2+ with negative clonus and locations and mechanisms of com- pression, including both structural or can have an insidious onset. Babinski reflexes bilaterally. The and systemic causes. Anatomical We present the case of a 14-year- patient had no lumbar tenderness variants should be considered old basketball player who developed and had a negative straight leg part of the differential diagnosis a compressive neuropathy of the raise bilaterally. in peroneal nerve impingement. common peroneal nerve secondary to On the basis of the clinical his- We present the case of a 14-year-old an accessory biceps femoris muscle. tory and physical examination, the basketball player with footdrop sec- ondary to compression of the com- mon peroneal nerve from an acces- sory biceps femoris muscle, which “...the diagnosis of an accessory biceps was treated by neurolysis. In addition, we review the systematic workup of femoris muscle should be part of the patients with nerve compression. -
Bflh Is Usually Compromised During Sprinting, but Slowspeed
anatomY REVIEW OF HAMSTRING ANATOMY – Written by Stephanie J Woodley and Richard N Storey, New Zealand The collective term ‘hamstrings’ refers may be related. For example, BFlh is usually BICEPS FEMORIS LONG HEAD to three separate muscles located in the compromised during sprinting, but slow- This muscle is of particular interest given posterior compartment of the thigh - biceps speed stretching injuries predominantly its susceptibility to injury. Some anatomical femoris (which consists of two components, affect SM1. Increasingly, imaging is being parameters that may be relevant when a long head [BFlh] and a short head [BFsh]), employed to confirm the location and considering strain injuries include its unique semitendinosus (ST) and semimembranosus severity of hamstring injuries and to inform muscle architecture and the arrangement of (SM) (Figure 1). There are numerous theories prognosis, particularly in professional and its proximal tendon which it shares with ST, on how this muscle group derived its name, elite athletes. a feature which may explain why injuries to but it appears to originate from the early With the above factors in mind, the Germanic language as well as the butchery purpose of this paper is to provide an trade. Slaughtered pigs were hung from overview of our current understanding of these strong tendons, hence the reference the morphology of the hamstring muscles. to ‘ham’ (meaning ‘crooked’ and thus Terms used frequently within this review BFlh is usually referring to the knee, the crooked part of require some explanation. Firstly, a tendon compromised the leg) and ‘string’ (referring to the string- can be considered to consist of two main like appearance of the tendons).