Peroneal Nerve Compression Secondary to an Anomalous Biceps Femoris Muscle in an Adolescent Athlete Kevin M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Anatomy of the Posterolateral Aspect of the Rabbit Knee
Journal of Orthopaedic Research ELSEVIER Journal of Orthopaedic Research 2 I (2003) 723-729 www.elsevier.com/locate/orthres The anatomy of the posterolateral aspect of the rabbit knee Joshua A. Crum, Robert F. LaPrade *, Fred A. Wentorf Dc~~ur/niiviiof Orthopuer/ic Surgery. Unicrrsity o/ Minnesotu. MMC 492, 420 Dcluwur-c Si. S. E., Minnwpoli,s, MN 55455, tiSA Accepted 14 November 2002 Abstract The purpose of this study was to determine the anatomy of the posterolateral aspect of the rabbit knee to serve as a basis for future in vitro and in vivo posterolateral knee biomechanical and injury studies. Twelve nonpaired fresh-frozen New Zealand white rabbit knees were dissected to determine the anatomy of the posterolateral corner. The following main structures were consistently identified in the rabbit posterolateral knee: the gastrocnemius muscles, biceps femoris muscle, popliteus muscle and tendon, fibular collateral ligament, posterior capsule, ligament of Wrisberg, and posterior meniscotibial ligament. The fibular collateral ligament was within the joint capsule and attached to the femur at the lateral epi- condyle and to the fibula at the midportion of the fibular head. The popliteus muscle attached to the medial edge of the posterior tibia and ascended proximally to give rise to the popliteus tendon, which inserted on the proximal aspect of the popliteal sulcus just anterior to the fibular collateral ligament. The biceps femoris had no attachment to the fibula and attached to the anterior com- partment fascia of the leg. This study increased our understanding of these structures and their relationships to comparative anatomy in the human knee. -

Peroneus Longus Tendon Regeneration After Anterior Cruciate Ligament Reconstruction with Magnetic Resonance Imaging Evaluation
Scientific Foundation SPIROSKI, Skopje, Republic of Macedonia Open Access Macedonian Journal of Medical Sciences. 2020 Nov 14; 8(A):916-920. https://doi.org/10.3889/oamjms.2020.5487 eISSN: 1857-9655 Category: A - Basic Sciences Section: Sports Medicine Peroneus Longus Tendon Regeneration after Anterior Cruciate Ligament Reconstruction with Magnetic Resonance Imaging Evaluation Sholahuddin Rhatomy1,2*, Bambang Kisworo3, Bunarwan Prihargono4, Faiz Alam Rashid1, Nolli Kressoni5 1Department of Orthopaedics and Traumatology, Dr. Soeradji Tirtonegoro General Hospital, Klaten, Indonesia; 2Department of Orthopaedics and Traumatology, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 3Department of Orthopaedics and Traumatology, Panti Rapih Hospital, Yogyakarta, Indonesia; 4Department of Orthopaedics and Traumatology, Karanganyar General Hospital, Karanganyar, Indonesia; 5Department of Radiology, Indriati Hospital, Sukoharjo, Indonesia Abstract Edited by: Slavica Hristomanova-Mitkovska BACKGROUND: Peroneus longus graft can be recommended as a superior graft over hamstring in anterior cruciate Citation: Rhatomy S, Kisworo B, Prihargono B, Rashid FA, Kressoni N. Peroneus Longus Tendon ligament (ACL) reconstruction. There are many studies concerning hamstring tendon regeneration, but there are few Regeneration after Anterior Cruciate Ligament studies on the regeneration of the peroneus longus tendon after ACL reconstruction. Reconstruction with Magnetic Resonance Imaging Evaluation. Open Access Maced J -

A Cadaver Research
Journal of Arthroscopy and Joint Surgery 6 (2019) 114e116 Contents lists available at ScienceDirect Journal of Arthroscopy and Joint Surgery journal homepage: www.elsevier.com/locate/jajs Tensile strength comparison between hamstring tendon, patellar tendon, quadriceps tendon and peroneus longus tendon: A cadaver research * Krisna Y. Phatama a, , Mohamad Hidayat a, Edi Mustamsir a, Ananto Satya Pradana a, Brian Dhananjaya b, Surya Iman Muhammad b a Orthopaedic and Traumatology Department, Lower Extremity and Adult Reconstruction Division, Saiful Anwar Hospital, Jalan Jaksa Agung Suprapto No.2, Klojen, Kota Malang, Jawa Timur, 65112, Indonesia b Orthopaedic and Traumatology Department, Saiful Anwar Hospital, Jalan Jaksa Agung Suprapto No. 2, Klojen, Kota Malang, Jawa Timur, 65112, Indonesia article info abstract Article history: Knee ligament injury is a frequent occurrence. Ligament reconstruction using tendon graft is the best Received 6 December 2018 therapy recommendation in the case of severe knee ligament injury. Tendon graft that is oftenly used are Accepted 15 February 2019 hamstring tendon, patellar tendon (BPTB), quadriceps tendon and peroneus longus tendon have been Available online 19 February 2019 proposed as tendon graft donor. Biomechanically, tensile strength from tendon graft is the main factor that greatly contributes to the success of ligament reconstruction procedure. Numerous researches have Keywords: been done to calculate tensile strengths of hamstring and patellar tendon, but there has not been a Ligament reconstruction research done yet on the comparison of the tensile strengths of peroneus longus tendon, hamstring, Tendon graft Tensile strength patellar tendon and quadriceps tendon. This research will strive to record the tensile strengths of per- oneus longus tendon, hamstring, patellar tendon and quadriceps tendon as well as their comparison. -

A Study on Peroneus Longus Autograft for Anterior Cruciate Ligament Reconstruction
International Journal of Research in Medical Sciences Kumar VK et al. Int J Res Med Sci. 2020 Jan;8(1):183-188 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20195904 Original Research Article A study on peroneus longus autograft for anterior cruciate ligament reconstruction Kumar V. K.*, Narayanan S. K., Vishal R. B. Department of Orthopedics, Sree Gokulam Medical College and Research Foundation, Venjaramoodu, Trivandrum, Kerala, India Received: 20 October 2019 Revised: 20 November 2019 Accepted: 02 December 2019 *Correspondence: Dr. Kumar V. K., E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: To compare the clinical outcome and donor site morbidity of ACL reconstruction with Peroneus longus tendon autografts in patients with isolated ACL injury. Methods: This was a prospective study that included patients who underwent ACL reconstruction using Peroneus longus tendon autograft. Results were assessed via physical examination. Donor site morbidity of the foot and ankle after tendon harvesting was assessed using Medical Research Council (MRC) grading of ankle and foot movements. Post-operative knee function was evaluated by the International Knee Documentation Committee (IKDC) scoring. Results: In this study sample of 25 patients, the ankle functions at the donor site are grossly preserved in almost all the patients, which was elucidated by grading the power of foot eversion. -

Muscles of the Hip and Lower Limb Review Questions 1
Scoring Review questions /10 Name __________________________ coloring /40 Date ____________ Total /50 Pd. ______ Muscles of the Hip and Lower Limb Review questions 1. What is the longest muscle of the body? ______________________________________________________________ Where is it located? _________________________________________________________________________________ 2. How did the quadriceps femoris get its name? ________________________________________________________ 3. What are the two main functions of the anterior hip and thigh muscles? a. ___________________________________________ b. ____________________________________________ 4. What are the two main functions of the posterior hip and thigh muscles? a. ____________________________________________ b. ____________________________________________ 5. What is the function of the medial thigh muscles? _____________________________________________________ 6. Straining what muscles is termed a “pulled groin”? ___________________________________________________ 7. What is the sole extensor of the knee? _______________________________________________________________ 8. On what surface of the leg are the muscles located that plantarflex the foot? ___________________________ Dorsiflex? __________________________________________________________________________________________ 9. What is the only dorsal foot muscle? _________________________________________________________________ What does it do? ___________________________________________________________________________________ 10. How -

Muscular Leg: Anterior
Muscular Leg: Anterior Go to: 1 11 Posterior view 2 Lateral view 3 Lower leg 10 Lower leg: Deep 9 4 Calf: Superficial Calf: Deep 5 8 Thigh: Anterior 6 7 Thigh: Deep Thigh: Posterior Foot: dorsal Foot: Lateral Answers:Foot: Plantar Muscular Leg: 1 11 Anterior 2 1. Sartorius 3 2. Adductor longus 10 3. Rectus femoris 4 9 4. Vastus medialis 5. Gastrocneumius & soleus 6. Tibia 5 8 7. Extensor digitorum longus 6 7 8. Tibialis anterior 9. Vastus lateralis 10. Iliotibial tract 11. Tensor fasciae latae Muscular Leg: Posterior 12 11 9 8 7 1 10 2 3 4 5 6 Muscular Leg: Posterior 12 11 9 8 7 1 10 2 3 4 5 6 1. Gluteus maximus 5. Peroneus longus 9. Gastrocnemius (medial head) 2. Iliotibial tract 6. Peroneus brevis 3. Biceps femoris (long 10. Semimembranosus 7. Calcaneus head) 11. Semitendinousus 4. Gastrocnemius (lateral 8. Calcaneal tendon head) 12. Adductor magnus Leg Lateral View 3 4 5 6 1 2 11 10 8 14 13 9 15 12 7 Leg Lateral View 3 4 5 6 1 2 11 10 8 14 13 9 15 12 7 1. Peroneus 6. Tensor fasciae latae 11. Gastrocnemeus (fibularis)brevis 7. Gluteus maximus (lateral head) 2. Extensor digitorum 12. Soleus longus 8. Biceps femoris (long head) 13. Peroneus (fibularis) 3. Vastus lateralis 9. Vastus lateralis longus 4. Rectus femoris 14. Calcaneal tendon 10. Semitendinosus 5. Iliotibial tract 15. Calcaneus 15 Lower Leg: 1 Superficial 2 3 14 4 13 5 12 11 6 10 7 9 8 Lower Leg: 15 1 Superficial 1. -

Tendon Variations of the Peroneal Musculature in Man David C
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine Spring 5-31-1973 Tendon Variations of the Peroneal Musculature in Man David C. Johnson Yale Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl Part of the Body Regions Commons Recommended Citation Johnson, David C., "Tendon Variations of the Peroneal Musculature in Man" (1973). Yale Medicine Thesis Digital Library. 2. http://elischolar.library.yale.edu/ymtdl/2 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. rn YALE MEDICAL LIBRARY TENDON VARIATIONS OF THE PERONEAL MUSCULATURE IN MAN David C. Johnson Augustus A. White, M, D,, Adviser CONTENTS Introduction Evolution Mechanism of Variation Normal Anatomy and Variations Peroneus Longus Peroneus Brevis leroneus Tertlus Accessory Peroneal Musculature Peroneus Digiti Minimi Peroneus Digiti Quart! Peroneus Quartus Peroneus Brevis II Anatomic Studies Specimens Dissections Results Peroneus Longus Peroneus Brevis Peroneus Tertius Peroneus Digiti Minimi Peroneus Digiti Quart! CONTENTS (cont. ) Peroneus Quartus page 35 Peroneus Accessorlus 36 Discussion 36 Tables #1 Composite Results of Study 44 #2 -
Bflh Is Usually Compromised During Sprinting, but Slowspeed
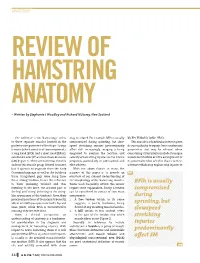
anatomY REVIEW OF HAMSTRING ANATOMY – Written by Stephanie J Woodley and Richard N Storey, New Zealand The collective term ‘hamstrings’ refers may be related. For example, BFlh is usually BICEPS FEMORIS LONG HEAD to three separate muscles located in the compromised during sprinting, but slow- This muscle is of particular interest given posterior compartment of the thigh - biceps speed stretching injuries predominantly its susceptibility to injury. Some anatomical femoris (which consists of two components, affect SM1. Increasingly, imaging is being parameters that may be relevant when a long head [BFlh] and a short head [BFsh]), employed to confirm the location and considering strain injuries include its unique semitendinosus (ST) and semimembranosus severity of hamstring injuries and to inform muscle architecture and the arrangement of (SM) (Figure 1). There are numerous theories prognosis, particularly in professional and its proximal tendon which it shares with ST, on how this muscle group derived its name, elite athletes. a feature which may explain why injuries to but it appears to originate from the early With the above factors in mind, the Germanic language as well as the butchery purpose of this paper is to provide an trade. Slaughtered pigs were hung from overview of our current understanding of these strong tendons, hence the reference the morphology of the hamstring muscles. to ‘ham’ (meaning ‘crooked’ and thus Terms used frequently within this review BFlh is usually referring to the knee, the crooked part of require some explanation. Firstly, a tendon compromised the leg) and ‘string’ (referring to the string- can be considered to consist of two main like appearance of the tendons). -

Morphometric Analysis of Peroneus Brevis Muscle in Adult Human Cadavers
Original Research Article Morphometric analysis of peroneus brevis muscle in adult human cadavers Poonam Verma1,*, Seema2 1,2Professor, Dept. of Anatomy, SGRDIMSAR *Corresponding Author: Poonam Verma Professor, Dept. of Anatomy, SGRDIMSAR Email: [email protected] Abstract Introduction: Keeping in view the frequency of variations in morphometry of musculature of the lower limb, Peroneus Brevis, the present work has been taken up. Under the research study of Peroneus brevis muscle in adult human cadavers of Punjab, the 2 dissection of sixty limbs was done. This muscle takes origin from distal /3 of the lateral surface of fibula anterior to the Peroneus Longus and anterior and posterior crural intermuscular septa and its insertion on the lateral aspect of base of fifth metatarsal. Aim: To converse surgical relevance of dissimilarities in the morphometry of this muscle. The present paper is for the curiosity for the disciples of orthopedics, radiology and sports medicine. Materials and Methods: Material consists of 60 lower limbs related to 30 embalmed adult human cadavers (20-70 years) of known sex got from Government Medical College, Amritsar. The muscle was exposed by dissection steps provided by Cunningham’s manual of practical anatomy from origin to insertion and length and width was taken. Results: Peroneus brevis muscle was detected in all the cases (60 limbs). Mean value of muscle belly length was 18 cm and width was 1.9 cm. While the mean length of the tendon with no muscle fibers up to insertion was 11 cm, and the mean width was found to be 0.5 cm. Conclusion: The clinical significance of this muscle is that the rebuilding of superior peroneal retinaculum can be done by using a portion of Peroneus brevis. -

Peroneal Tendon Disorders
Dr Todd Gothelf www.orthosports.com.au 47‐49 Burwood Road, Concord 29‐31 Dora Street, Hurstville 119‐121 Lethbridge Street, Penrith 160 Belmore Road, Randwick Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Peroneal Tendon Disorders Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Peroneal Tendon Disorders • Tenosynovitis •Tears • Snapping Peroneal Tendons Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Cause of injury •Occur during acute ankle sprain •Can occur as well by attrition over time. • Multiple ankle sprains/recurrent instability Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Lateral Ankle Sprain •“Complete Rupture of the ATFL Ligament” •Treated Non‐ operatively Dr Todd Gothelf Shoulder, Foot & Ankle Surgery ACL Rupture/ Rotator Cuff Tear •“Complete Rupture of the ACL ligament” •“Full Thickness tear of the Rotator Cuff • Usually require surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Lateral Ankle Sprains •Treat the complete ATFL rupture NON‐ operatively • Similar outcomes to surgical treatment with LESS RISK. •Can Always do surgery later on. Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Causes of Pain after Lateral Ankle Sprain‐ NOT ATFL •Talardome lesions •Intra‐articular scar tissue, impingement • Peroneal tendon tears • Peroneal tendon dislocations •Missed achilles •Missed Syndesmosis •Missed Lis Franc Dr Todd Gothelf Shoulder, Foot & Ankle Surgery Anatomy Peroneal Tendons •Acute Angle around fibula • Eversion/Flexion •SPR‐ -

Congenital Entrapment of the Lateral Cutaneous Nerve of the Calf Presenting As a Peroneal Sensory Neuropathy
Congenital Entrapment of the Lateral Cutaneous Nerve of the Calf Presenting as a Peroneal Sensory Neuropathy Daniel G. Hackam and Thomas J. Zwimpfer ABSTRACT: Objective: Presentation of an unusual case of congenital entrapment of the lateral cutaneous nerve of the calf (LCNC) mimicking a peroneal sensory neuropathy. Methods: We report the case of a 16-year-old girl with a 3 year history of progressive tingling, numbness and pain in her right calf precipitated by athletic activities involving repeated flexion and extension of the knee. A Tinel's sign was present over the common peroneal nerve in the distal popliteal fossa but absent at the fibular neck. Motor and sensory examination of the common peroneal nerve was normal as were electrophysiological studies and MRI. Results: At surgery, the LCNC, a sensory branch of the common peroneal nerve, was entrapped at a point where it pierced the tendon of the biceps femoris muscle. Transection of the part of the tendon overlying the LCNC resulted in complete and permanent relief of symptoms. Significance and Conclusion: The proximal location of the Tinel's sign, absence of motor or sensory deficits and normal electrophysiology suggested, preoperatively, that this was not an entrapment of the common peroneal nerve at the fibular neck but rather a more proximal abnormality likely involving only a part of the peroneal nerve or one of its sensory branches. As a result, more proximal exposure of the peroneal nerve within the popliteal fossa revealed entrapment of the LCNC due to its anomalous course through the biceps femoris tendon. This case has two noteworthy features. -

Chapter 9 the Hip Joint and Pelvic Girdle
The Hip Joint and Pelvic Girdle • Hip joint (acetabular femoral) – relatively stable due to • bony architecture Chapter 9 • strong ligaments • large supportive muscles The Hip Joint and Pelvic Girdle – functions in weight bearing & locomotion • enhanced significantly by its wide range of Manual of Structural Kinesiology motion • ability to run, cross-over cut, side-step cut, R.T. Floyd, EdD, ATC, CSCS jump, & many other directional changes © 2007 McGraw-Hill Higher Education. All rights reserved. 9-1 © 2007 McGraw-Hill Higher Education. All rights reserved. 9-2 Bones Bones • Ball & socket joint – Sacrum – Head of femur connecting • extension of spinal column with acetabulum of pelvic with 5 fused vertebrae girdle • extending inferiorly is the coccyx – Pelvic girdle • Pelvic bone - divided into 3 • right & left pelvic bone areas joined together posteriorly by sacrum – Upper two fifths = ilium • pelvic bones are ilium, – Posterior & lower two fifths = ischium, & pubis ischium – Femur – Anterior & lower one fifth = pubis • longest bone in body © 2007 McGraw-Hill Higher Education. All rights reserved. 9-3 © 2007 McGraw-Hill Higher Education. All rights reserved. 9-4 Bones Bones • Bony landmarks • Bony landmarks – Anterior pelvis - origin – Lateral pelvis - for hip flexors origin for hip • tensor fasciae latae - abductors anterior iliac crest • gluteus medius & • sartorius - anterior minimus - just superior iliac spine below iliac crest • rectus femoris - anterior inferior iliac spine © 2007 McGraw-Hill Higher Education. All rights reserved. 9-5 © 2007 McGraw-Hill Higher Education. All rights reserved. 9-6 1 Bones Bones • Bony landmarks • Bony landmarks – Medially - origin for – Posteriorly – origin for hip hip adductors extensors • adductor magnus, • gluteus maximus - adductor longus, posterior iliac crest & adductor brevis, posterior sacrum & coccyx pectineus, & gracilis - – Posteroinferiorly - origin pubis & its inferior for hip extensors ramus • hamstrings - ischial tuberosity © 2007 McGraw-Hill Higher Education.