How to Cite Complete Issue More Information About This Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cologno Monzese Alla Ricerca Del Territorio Perduto
Storia locale - Studi storici Elisabetta Ferrario Mezzadri Cologno Monzese alla ricerca del territorio perduto Biblioteca Civica Presentazione Il venti dicembre del 1990, con delibera dirigenziale n° 1736, l’Amministrazione comunale di Cologno Monzese conferì all’Arch. Elisabetta Ferrario Mezzadri il compito di condurre una ricognizione del patrimonio architettonico storico presente sul territorio comunale e di darne conto in un elaborato che descrivesse i siti censiti, ricostruendone per quanto possibile la genesi e la storia delle modifiche intervenute nel corso del tempo. Rese eloquenti nelle loro stratificazioni storiche e nella ricchezza delle relazioni sistemiche che le legano al territorio, incontriamo ville, cioè residenze di campagna del ceto nobile, cascine, centri di produzione e trasformazione dei prodotti agricoli provenienti dai terreni collegati, borghi rurali, fontanili, boschi e luoghi di sosta per carrettieri; tutti elementi che hanno segnato per secoli, il territorio colognese, disegnandolo sia dal lato paesaggistico sia come nuclei originari di un ininterotto processo di antropizzazione e urbanizzazione. Frutto di una ampia e accurata ricerca documentale condotta sul campo come tra gli archivi storici, il lavoro è arricchito da un imprescindibile corredo iconografico, quasi sempre originale. La qualità scientifica di questo lavoro, che nulla ha perduto del suo interesse a vent’anni dalla sua redazione, mette dunque in luce i profondi legami urbanistici, come sociali ed economici, impliciti nella cartografia dei luoghi storici; noi sappiamo che sono questi legami che vanno a formare quel nucleo di specificità e identità che chiamiamo contesto culturale locale. Per questo la biblioteca civica ha ritenuto utile pubblicare l’opera nella speranza che possa nutrire, con la sua passione per il nostro passato, un maggior rispetto per le vestigia di un mondo sì scomparso ma non morto, un passato capace di potenti suggestioni che attendono solo di essere evocate. -

Per 6 Grandi Progetti
PAGINA PAGINA Provincia di Monza e Brianza Anpi, eletto il nuovo presidente «Taglio ai costi»: stop È Cesare Brambilla www.bcccarugate.it 3 al Provveditorato agli studi 6 «Puntiamo sui giovani» Differente per forza Aprile mese decisivo per i piani urbanistici - L’opposizione: «Aspettiamo le elezioni» CORSA FINALE per 6 grandi progetti orsa finale dell’amministra- LA COMMISSIONE DICE «NO» AL LA TORRE DELLA BINDELLERA zione Cifronti per condurre in porto numerosi progetti urbanistici. In ballo ci sono al- Cmeno sei interventi. Entro fine aprile una parte di questi potrebbe passare dal consigio comu- nale per la fase di Attesi adozione, primo Anno VII - N. 12 in aula gradino dell’iter Sabato 28 marzo 2009 anche che porterà all’ap- Settimanale edito provazione defini- dall’associazione culturale Kairós i ritocchi agli oneri tiva solo con l’arri- LA PAROLA DELLA SETTIMANA vo della nuova am- per costruire ministrazione. Dal- Dando si riceve l’aula di Villa Fiori- ta dovrà passare anche l’adeguamen- amando si è amati to degli oneri di urbanizzazione e l’ok al Parco delle cave. Intanto, giovedì di Angelo Sceppacerca sera, la commissione urbanistica ha bocciato l’ipotesi di un grattacielo nel quaranta giorni della Quaresima piano della Bindellera. Le stesse vo- corrono veloci. Domenica prossima lumetrie dovranno essere suddivise I sarà quella delle Palme e quella suc- in palazzine più basse. cessiva, infine, Pasqua. Di questo avvici- A PAGINA 3 narsi dei grandi giorni santi è prova il Vangelo di oggi nel quale Gesù stesso di- pagina 11 pagina 15 chiara che "è venuta l'ora". -

Elenco Mappe Per Sito
ELENCO MAPPE 1620 Ducato di Milano 1620 Ducato di Milano particolare primi 1700 Lambro a sud di Monza 1721 Brugherio sotto Monza 1721 Cascina Bastoni 1721 Cascina Increa 1721 San Damiano originale di campagna 1721 San Damiano BRUGHERIO 1722 Cascina Occhiate e Malnido originale TERRITORIO DI 1757 Cassina Baraggia MONZA 6 1757 Stato di Milano 1758 Raccolta editti del Censimento 1781 Ducato di Milano 1855 San Damiano 1871 Brugherio sotto Monza centro e Bindellera 1871 Brugherio sotto Monza particolare centro 1871 Ca' Secca 1871 Cascina Occhiate 1721 - Mappe di CASSINA BARAGGIA con porzione di Brugherio S. SAN DAMIANO 4 Carlo VI Ambrogio Pieve di Vimercate - composta da 9 fogli. BARAGGIA 1721 1721 - Mappe di Territorio di S. Damiano Corte di Monza - composta Carlo VI da 4 fogli. 1700 Fiume Lambro e le sue rogge Fiume Lambro primi 1700 Mappa privata Cascina Occhiate CASSINA BARAGGIA con porzione di Brugherio S. 1721 - Mappe di Ambrogio Pieve di Vimercate - Mappa copia tratta Carlo VI dall'originale mappa arrotolata in 9 fogli (unificati) Mappa originale DEL TERRITORIO DI SAN DAMIANO - 1721 Pieve di Vimercate 1721 Moncucco e Uniti (unione dei fogli) CARTE E MAPPE 16 E 1750 Moncucco e Uniti MANIFESTO 1757 Pieve di Vimercate 1757 Corte di Monza: foglio con Brugherio 1763 Topografia Monte di Brianza particolare 1763 Topografia Monte di Brianza Beni Monastero S Caterina alla Chiusa - Giovanni 1767 Antonio Veladini - ASM - Fondo di Religione Mappa del Comune censuario di Moncucco di 1855 Monza ed Uniti Mandamento II di Monza Provincia di Milano (unione dei fogli) MAPPE 1856 1880 Mappa del Comune Censuario di Brugherio con 1887 - MAPPE parte 1856 Cassina Baraggia, S Ambrogio e Cassina Increa - 1 e parte 2 composta da 11 fogli. -

Scheda Completa Sirbec
SIRBeC scheda ARL - MI100-01286 Oratorio di S. Lucio Papa Brugherio (MB) Link risorsa: https://www.lombardiabeniculturali.it/architetture/schede/MI100-01286/ Scheda SIRBeC: https://www.lombardiabeniculturali.it/architetture/schede-complete/MI100-01286/ SIRBeC scheda ARL - MI100-01286 CODICI Unità operativa: MI100 Numero scheda: 1286 Codice scheda: MI100-01286 Visibilità scheda: 3 Utilizzo scheda per diffusione: 03 NUMERO INTERNO Riferimento: Rilevazione dei beni architettonici e ambientali nei comuni della Provincia di Milano Numero interno: 150340033 Tipo scheda: A Livello ricerca: P CODICE UNIVOCO Codice regione: 03 Ente schedatore: Provincia di Milano Ente competente: S26 RELAZIONI STRUTTURA COMPLESSA Livello: 1 Codice IDK della scheda di livello superiore: MI100-01267 OGGETTO OGGETTO Ambito tipologico principale: architettura religiosa e rituale Definizione tipologica: chiesa Denominazione: Oratorio di S. Lucio Papa ALTRA DENOMINAZIONE [1 / 2] Genere denominazione: originaria Denominazione: Cappella di S. Antonio Fonte dell'altra denominazione: bibliografia Pagina 2/24 SIRBeC scheda ARL - MI100-01286 Specifica della fonte dell'altra denominazione 1994, Valli, L./ Cannella, C., Il Tempietto di Moncucco/ Restauro e considerazioni sull'ex Oratorio dei Conti Andreani-Sormani in Brugherio già Cappella di S. Antonio presso il Convento di San Francesco in Lugano ALTRA DENOMINAZIONE [2 / 2] Genere denominazione: idiomatica Denominazione: Tempietto di Moncucco Fonte dell'altra denominazione: bibliografia Specifica della fonte dell'altra denominazione -

Il Fondo Meani Di Luciana Tribuzio Zo I I Documenti, Le Fotografie E Le
Il Fondo Meani di Luciana Tribuzio Zoi I documenti, le fotografie e le mappe della raccolta, meglio nota come Fondo Meani, hanno caraere locale e provengono dai vari fondi degli archivi milanesi (Archivio di Stato, Archivio Diocesano, Archivio Storico - Civico, Archivio ertarelli), dell"Archivio Storico Civico e dell"ECA di Mon$a, dell"Archivio Parrocchiale di San artolomeo e dell"Archivio Storico del Comune di rugherio. In larghissima parte si traa di fotocopie' solo in (ualche caso i documenti sono originali e provengono da Enti pubblici e privati ciadini. Il materiale cartaceo * conservato nella sala di Storia locale, in contenitori/bo,' i documenti, singoli o in fascicoli, sono protei dalle cosiddee -camicie. per evitare il logoramento del materiale cartaceo. Il Fondo Meani contiene documenti che vanno dal 701 al 1315. I documenti della raccolta, (uasi tui di caraere locale, sono suddivisi in 10 classi5 1. Ac(ue e Strade (3 cartelle) 2. Agricoltura (5) 3. Amministra$ione delle antiche Comunit8 ante 1703 e dei Comuni ante 1100 (3) 4. Catasto (10) 5. Censo (1) 0. Culto (7) 7. Famiglie (27) 1. Finan$e (1) 3. Giusti$ia e Poli$ia (3) 10. Igiene e Sanit8 (1) 11. Istru$ione 12. Militari - Risarcimenti danni di guerra e alloggiamento soldati (1) 13. Miscellanea (3) 14. Monastero di S. Ambrogio di Milano (1) 15. Monastero di S. Caterina alla Chiusa di Milano, e, S. Ambrogio (4) 10. Tranvia rugherio - Mon$a (1) Cartelle5 71 Unit8 archivistiche5 1405 Nell@inventaria$ione e nella schedatura analitica dei documenti presenti nell"inventario si * voluto esprimere, in maniera completa, la descri$ione dell@oggeo del documento singolo o del fascicolo. -

Inventario Del Fondo Meani in Formato
Biblioteca Civica di Brugherio Documenti e mappe dall’anno 768 al 1985 Raccolti principalmente in copia presso Archivi diversi dal signor GIUSEPPE MEANI A cura di Luciana Tribuzio Zotti con la collaborazione di Enrico Sangalli Comune di Brugherio Le tantissime iniziative che hanno coinvolto Brugherio a tutti i livelli in occasione del suo 150° continuano a lasciare le loro tracce in una città che ha riscoperto il valore di sentirsi comunità e che si è appassionata come mai prima d'ora alla ricerca sulla propria storia. In un contesto di così fervida ricerca, ai 50 nuovi cartelli turistici dotati di Qrcode, al Portale di storia locale e alle diverse pubblicazioni su vari aspetti della storia cittadina che hanno arricchito la nostra Biblioteca, si aggiunge ora l'occasione di poter attingere direttamente alle fonti rappresentate dal “Fondo Meani”, reso finalmente disponibile alla consultazione grazie a un lungo, paziente e competente lavoro di riordino, inventariazione e catalogazione realizzato dalla Prof.ssa Luciana Tribuzio, con la collaborazione di un volontario, Enrico Sangalli, e l'assistenza tecnica di Silvia Barzago, referente della Sezione di storia locale della Biblioteca Civica. Un lavoro preziosissimo, che mette finalmente a disposizione di tutti i brugheresi l'inesauribile fonte di informazioni archivistiche rappresentata dai documenti raccolti nell'arco di una vita da Giuseppe Meani, un concittadino appassionato delle sue radici. Ora l'inventario di questa importante raccolta potrà essere finalmente consultato anche sul Portale di Storia Locale, il centro di documentazione della storia e della realtà cittadina inaugurato in occasione del 150°, per offrire ai cittadini, agli studenti e agli appassionati la più ampia possibilità di accesso agli strumenti di ricerca, alle fonti e ai documenti sulla storia della nostra città. -

Siride a Brugherio: Grande Festival Degli Artisti Di Strada
Brugherio periodico spedito gratuitamente - anno XLI - numero 6 - SETTEMBRE 2011 sIride a Brugherio: grande festival degli artisti di strada > AMMINISTRAZIONE > SCUOLA > SPECIALE CORSI > FESTA DI BRUGHERIO Iniziative e progetti Un nuovo anno Una stagione Il programma per la nuova stagione ricco di novità piena di appuntamenti dei festeggiamenti www.comune.brugherio.mb.it Brugherio Brugherio periodico spedito gratuitamenament e - anno XLI - numernumeroo6 6 - SETTEMBRE 2011 Editoriale Tempus fugit, sIride a Brugherio: g ra n d e fe s t i va l ma almeno degli artisti di stra d a > AMMINISTRAZIONE > SCUOLA > SPECIALE CORSI > FESTA DI BRUGHERIO non aiutiamolo! Iniziative e progetti Un nuovo anno Una stagione Il programma per la nuova stagione ricco di novità piena di appuntamenti dei festeggiamenti www.comune.brugherio.mb.it B r u g h e r i o Siamo ormai a fine settembre e le vacanze estive, con i loro salutari e rilassanti effetti, sono già quasi un ricordo. Ci restano le fotografie da guardare, i flashback da godere Anno XLI - numero 6 - SETTEMBRE 2011 e qualche souvenir a testimoniare i luoghi visitati. In questa simbolica valigia di me- morie estive, permane con piacere la percezione di aver vissuto e goduto un tempo Direttore Responsabile: speso meglio. Un tempo che in vacanza mi è parso essere più a contatto con il mio Adolfo Gatti andamento fisico, psicologico e relazionale. Senza l’assillo del lavoro, dei ritmi quoti- diani e delle incombenze che tutti ben conosciamo, in vacanza si riesce a riassaporare Redazione: il tempo goduto in pieno, ben speso e a misura delle nostre necessità, emozioni e bi- Sara Anzalone Alessia Pignoli sogni. -

2 FG9A Nationale Patente Brevets Nationaux Brevetti
14.5.2004 +pat+ 9 B 2 FG9A I A61M039/20, A 61 M 039/02 00111/00 C A 693 941 20.01.2000 K Nationale Patente B 00901/99 Schablone zum Herstellen von C 11.05.1999 Briefumschlägen. O Brevets nationaux F 12.05.1998 US 09/076,442 Reinhard Gut-Widmeier K Entfernbare Plazierungsspitze. Rebrainstrasse 17b O 8624 Grüt (Gossau) (CH) Brevetti nazionali NOVARTIS NUTRITION AG N Monbijoustrasse 118 Reinhard Gut-Widmeier 3001 Bern (CH) Rebrainstrasse 17b N Michels, Lester D. 8624 Grüt (Gossau) (CH) 2.3 FG3A 9149 Fox Run Circle I B32B001/04, F 16 L 059/06, Eden Prairy, Minnesota 55347 (US) G10K011/00 Ohne Vorprüfung erteilte P Novartis AG Patent & Trademark A 693 946 Patente Department B 00120/00 4002 Basel (CH) C 21.01.2000 Brevets délivrés sans F examen préalable I B23H001/02 23.01.1999 DE 199 02 599.1 A K Isoliermatte. 693 942 O Brevetti rilasciati senza B 02569/95 Helmut W. Diedrichs esame preventivo C 11.09.1995 Greinstrasse 49 F 64291 Darmstadt (DE) 09.09.1994 JP A6-216245 N 05.09.1995 JP A7-228102 Helmut W. Diedrichs Greinstrasse 49 K Speiseeinheit für einen I A44C017/00 64291 Darmstadt (DE) Erosionsapparat. A 693 938 Ritter, Jürgen O Mitsubishi Denki Kabushiki Kaisha B 02370/99 Haaner Strasse 145 2-3, Marunouchi 2-chome C 23.12.1999 D-42719 Solingen (DE) Chiyoda-ku/Tokyo (JP) K Gemme taillée, en particulier P Isler & Pedrazzini AG Mitsubishi Electric Engineering Co., diamant taillé. 8023 Zürich (CH) Ltd O Montblanc Simplo GmbH 6-2, Otemachi 2-chome I B 32 B 007/12 Z B 32 B 021/04 100, Hellgrundweg, Chiyoda-ku/Tokyo 100 (JP) A 693 947 D-22525 Hamburg (DE) N Akamatsu, Koji N Eve Zimet I Nagoya-shi/Aichi 461 (JP) B32B021/04, B 32 B 007/12, Talstrasse 20 Suzuki, Satoshi C09K021/00, E 04 B 001/94 8027 Zürich (CH) A Nagoya-shi/Aichi 462 (JP) 693 947 Nadine Schmidt B Taneda, Atsushi 02214/99 Talstrasse 20 C Nagoya-shi/Aichi 461 (JP) 02.12.1999 8027 Zürich (CH) F Ogawa, Hajime 12.11.1999 DE 299 19 919.3 P K Micheli & Cie ingénieurs-conseils Nagoya-shi/Aichi 461 (JP) Feuerhemmende Sandwichplatte. -

Gli Anni Della Guerra: Storie Di Vita E Di Morte Brugherio 1940 - 1945
Papaveri Rossi collettivo aperto di ricerca storica Gli anni della guerra: storie di vita e di morte Brugherio 1940 - 1945 Città di Brugherio Papaveri Rossi collettivo aperto di ricerca storica Gli anni della guerra: storie di vita e di morte Brugherio 1940 - 1945 Città di Brugherio Assessorato alle Politiche culturali Città di Brugherio Assessorato alle Politiche culturali Marco Troiano, sindaco di Brugherio Laura Valli, assessora alle Politiche culturali Enrica Meregalli, direttrice della Biblioteca civica Silvia Barzago, sezione di Storia locale - Biblioteca civica Ermanno Vercesi e Riccardo Rappa, progetto grafico e impaginazione Prima edizione, dicembre 2020 Foto di copertina: disegno di Erika Taussigovà, Ghetto di Terezín. 1943 – 1944 Ringraziamenti degli autori Un sentito ringraziamento a tutti coloro che singolarmente o come soggetti di riferimento hanno consentito la pubblicazione di questo lavoro. In primo luogo al Comune e alla Biblioteca Civica di Brugherio per averci sostenuto nella ricerca, mettendo a disposizione tempo e competenze. Un grazie particolare a Laura Muserra per i suoi preziosi consigli e per il lavoro di revisione dei testi, a Fulvio Bella per la disponibilità a scrivere la prefazione e a Ros Video per l'aiuto sulla parte fotografica. Ringraziamo anche alcuni famigliari dei caduti che, sapendo di questa ricerca, hanno messo a disposizione documenti e foto in loro possesso, così come la sezione di Brugherio dell'Associazione Alpini per averci permesso di consultare l'archivio dell'Associazione Combattenti e Reduci di Brugherio. Grazie infine ai nostri amici che durante la stesura di questo libro hanno avuto l'opportunità di leggere parti della ricerca e con i loro giudizi ci hanno sostenuto e incoraggiato nel portare a termine questo lavoro. -

Buon Compleanno
PAGINE PAGINA 160.000 euro per le luci Tante proposte stradali. Nuovi proiettori per l’Avvento di S. Paolo www.bcccarugate.it 5 e risparmio energetico 13 Il 17 oratorio in festa Differente per forza È stato Vittorio Emanuele II a riunire piccole municipalità in un unico Comune Allora il paese contava 3.686 abitanti, oggi vivono in città 33.000 persone BUON COMPLEANNO N. 124 - Sabato 9 dicembre 2006 Settimanale edito dall’associazione culturale Kairós LA PAROLA DELLA SETTIMANA La strada, la storia, il deserto Brugherio è nata il 9 dicembre 1866 di don Giovanni Meraviglia rugherio compie 140 anni. Il tuiscono i nuclei storici degli attuali "Brugherio" [...] Nel più breve tempo immagine che questa domenica di Comune fu infatti istituito quartieri come Increa, Baraggia, Il titolo di città possibile si procederà alla elezione dei L’ Avvento ci presenta è quella della con regio decreto di Vittorio Moncucco, Guzzina, Moia, Ca’ nuovi Consigli comunali». Già all’e- strada. La Parola di Dio che scende su Emanuele II il 9 dicembre Secca, Sant’Ambrogio. è stato invece poca della dominazione austriaca de- Giovanni il Battista nel deserto B1866, riunendo le piccolissime muni- «Vista la domanda sporta dalla mag- concesso gli Asburgo si era tentata una riunifi- (Vangelo), e prima ancora sui profeti cipalità indipendenti che facevano gioranza degli elettori della parroc- dal presidente cazione, ma si era dovuto desistere Isaia e Baruc (prima lettura), raccoman- parte della parrocchia di San chia di Brugherio - si leggeva nel do- per l’opposizione delle aristocrazie da di preparare una via, una strada al Bartolomeo. -

Piano Territoriale Di Coordinamento Provinciale Ai Sensi Della LR 12/2005 ALLEGATO a DICEMBRE 2011
PTCP Piano Territoriale di Coordinamento Provinciale ai sensi della LR 12/2005 ALLEGATO A DICEMBRE 2011 PROVINCIA MONZA BRIANZA L’attività di collaborazione ed assistenza tecnico-scientifica alla redazione del PTCP – Piano Territoriale di Coordinamento Provinciale della Provincia di Monza e della Brianza [IST_20_10] è ricompresa nei Programmi di Collaborazione Centro Studi PIM – Provincia di Monza e della Brianza [Settore Pianificazione Territoriale e Parchi] per gli anni 2010 e 2011. dicembre 2011 PTCP // Piano Territoriale di Coordinamento Provinciale ai sensi della legge regionale n.12/2005 Adozione Adottato con deliberazione del Consiglio Provinciale n. XX del gg mese anno Approvazione Approvato con deliberazione del Consiglio Provinciale n. XX del gg mese anno. Pubblicazione Pubblicato sul Bollettino Ufficiale della Regione Lombardia, Serie Inserzioni n. XX del gg mese anno, ai sensi dell'art. 17 comma 10 della LR 12/2005 PROVINCIA DI MONZA E DELLA BRIANZA Settore Pianificazione Territoriale e Parchi Paolo Morazzoni, Direttore Laura Brioschi, ufficio di piano Bruno Grillini, sistemi verdi Marco Longoni, pianificazione territoriale Lisa Sacchi, difesa del suolo con la collaborazione dei Settori Ambiente ed Agricoltura Fabio Sabatino Lopez Nunes, Direttore Infrastrutture, Interventi strategici, Opere pubbliche e Trasporti Antonio Infosini, Direttore Turismo, Sport e Tempo Libero, Caccia e Pesca, Attività produttive, Politiche Giovanili Saverio D’Ambrosio, Direttore Viabilità e Strade Saverio Bourlà, Direttore COMITATO TECNICO SCIENTIFICO -
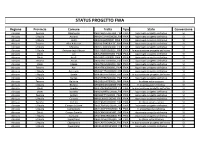
Status Progetto Fwa
STATUS PROGETTO FWA Regione Provincia Comune Tratta Tipo Stato Convenzione Abruzzo Pescara Abbateggio ABI3ABBATEGGIO00_FWA FWA Approvato progetto definitivo SI Abruzzo L'Aquila Acciano ABR2ACCIANO00000_FWAFWA Approvato progetto definitivo SI Abruzzo L'Aquila Aielli ABI3AIELLI000000_FWA FWA Approvato progetto definitivo SI Abruzzo Teramo Alba Adriatica ABR1ALBAADRIATIC_FWA FWA Approvato progetto definitivo SI Abruzzo L'Aquila Alfedena ABI3ALFEDENA0000_FWA FWA Approvato progetto definitivo SI Abruzzo L'Aquila Anversa degli Abruzzi ABI4ANVERSADEGLI_FWA FWA In approvazione progetto definitivo SI Abruzzo Chieti Ari ABI4ARI000000000_FWA FWA Approvato progetto definitivo SI Abruzzo Chieti Arielli ABI2ARIELLI00000_FWA FWA Approvato progetto definitivo SI Abruzzo Teramo Arsita ABR2ARSITA000000_FWA FWA Approvato progetto definitivo SI Abruzzo Chieti Atessa ABI3ATESSA000000_FWA FWA Approvato progetto definitivo SI Abruzzo Teramo Atri ABI4ATRI00000000_FWA FWA Approvato progetto definitivo SI Abruzzo L'Aquila Avezzano ABI3AVEZZANO0000_FWA FWA Approvato progetto definitivo SI Abruzzo L'Aquila Barete ABI4BARETE000000_FWA FWA In approvazione progetto definitivo SI Abruzzo L'Aquila Barrea ABI2BARREA000000_FWA FWA Approvato progetto definitivo SI Abruzzo Teramo Bellante ABI3BELLANTE0000_FWA FWA In attesa autorizzazioni SI Abruzzo L'Aquila Bisegna ABR2BISEGNA00000_FWA FWA In progettazione definitiva SI Abruzzo Chieti Bomba ABI4BOMBA0000000_FWAFWA In approvazione progetto definitivo SI Abruzzo Chieti Borrello ABR2BORRELLO0000_FWAFWA Approvato progetto definitivo