Study Protocol
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Combining a Glucagon-Like Peptide-1 Receptor Agonist with Basal Insulin: the Why and How
Combining a Glucagon-like Peptide-1 Receptor Agonist with Basal Insulin: The Why and How Case Study Mary is a 61 year-old female diagnosed with type 2 diabetes mellitus (T2DM) 8 years ago. She was initially managed with the combination of lifestyle modification and metformin. Since that time she was treated with a sulfonylurea, but it was discontinued due to symptomatic hypoglycemia. She was also treated with pioglitazone, but significant fluid retention led to it discontinuation. A year-and-a- half ago, basal insulin was added to her lifestyle and metformin management. She now administers 52 units (0.62 units/kg) once daily at bedtime. Since starting basal insulin, she has experienced 3 episodes of mild hypoglycemia. Since her diagnosis, Mary’s HbA1c has never been <7.0%; her current HbA1c is 7.9%. Over the past month, her fasting plasma glucose (FPG) has ranged from 103 mg/dL to 136 mg/dL and her postprandial glucose (PPG) from 164 mg/dL to 213 mg/dL. She has gained 2.6 kg since starting basal insulin and her body mass index is now 31 kg/m2. Her blood pressure is 134/82 mmHg. She experiences occasional tingling in her feet. Eye examination reveals grade 1 retinopathy. Current medications are: metformin 1000mg twice daily, basal insulin 52 units once daily at bedtime, and hydrochlorothiazide 25 mg once daily. Her family physician notes that Mary’s FPG is reasonably well-controlled, yet her HbA1c and PPG remain elevated. He is also concerned about her episodes of hypoglycemia and weight gain and the evidence indicating microvascular damage. -

Performance of the Insulin-Only Ilet Bionic Pancreas and The
e118 Diabetes Care Volume 44, June 2021 Performance of the Insulin-Only Luz E. Castellanos,1 Courtney A. Balliro,1 Jordan S. Sherwood,1 Rabab Jafri,1 iLet Bionic Pancreas and the Mallory A. Hillard,1 Evelyn Greaux,1 Rajendranath Selagamsetty,2 Hui Zheng,3 Bihormonal iLet Using Firas H. El-Khatib,2 Edward R. Damiano,2,4 and Dasiglucagon in Adults With Type Steven J. Russell1 1 Diabetes in a Home-Use Setting Diabetes Care 2021;44:e118–e120 | https://doi.org/10.2337/dc20-1086 Reductions in blood glucose levels in with insulin lispro (Eli Lilly) or aspart (Table 1). The mean CGM glucose and people with diabetes are often achieved (Novo Nordisk), the bihormonal iLet for time in range (70–180 mg/dL) were 149 at the expense of increased hypoglyce- 7dayswithdasiglucagon(4mg/mL) ±13mg/dLand72±8%,respectively,in mia. A novel approach is to automati- and insulin lispro or aspart, or both, us- the insulin-only period, and 139 ± 11 cally deliver microdose glucagon when ing the same glucose target (110 mg/ mg/dL and 79 ± 9%, respectively, in the automation of insulin delivery alone is dL), in random order. There were no re- bihormonal period. The mean daily car- not sufficient to prevent hypoglycemia. strictions on diet or exercise. The prima- bohydrates consumed to prevent or The approach requires a bihormonal de- ry outcomes were prespecified iLet treat hypoglycemia were 16 ± 13 g and vice and a stable form of glucagon or operational thresholds. The key second- 18 ± 21 g in the insulin-only and bihor- glucagon analog. -

(Pram) and Insulin A21G Improves Post-Prandial Glucose Vs Novolog
ADO09, A Co-Formulation Of Pramlintide (Pram) and Insulin A21G improves Post-Prandial Glucose Vs Novolog® in Type 1 Diabetes (T1DM) G.Meiffren¹, G.Andersen², R.Eloy¹, C.Seroussi¹, C.Mégret¹, S.Famulla², Y.-P Chan¹, M.Gaudier¹, O.Soula¹, J.H. DeVries²,T.Heise² (1 Adocia, Lyon, France ; 2 Profil, Neuss, Germany) Introduction & Background Overall safety Outpatient period results - CGM metrics o ADO09 (M1Pram) is a co-formulation of pramlintide and insulin A21G o Both treatments were well tolerated without any treatment-related serious adverse events o Most of the CGM metrics (TiR [70-180], TiR [80-140], mean blood glucose per day), were significantly improved developed to leverage the beneficial effects of pramlintide on post-prandial (Table 2). As expected M1Pram had numerically more, mostly gastrointestinal adverse events with M1Pram (Table 4). Postprandial and mean 24-hour glucose profiles were improved with M1Pram (Fig. 3) glucose without additional injections than insulin aspart Table 4: CGM metrics, all days. Significant differences are marked in bold Objective and design o No severe hypoglycemia were seen, slightly more hypoglycemic events occurred with M1Pram Ratio of LSMean* o To compare the effect of M1Pram and insulin aspart (Novolog®, Novo than with aspart (Table 3) Difference Parameter Treatment LS Mean M1Pram / Aspart P-value Nordisk) on post-prandial glucose control, glycemic control assessed by Table 2: Incidence of adverse events throughout the trial (M1Pram-Aspart) (95% CI) CGM and safety/tolerability M1Pram Aspart M1Pram -

Soliqua – Criteria
Criteria Based Consultation Prescribing Program CRITERIA FOR DRUG COVERAGE Insulin glargine; lixisenatide (Soliqua) subcutaneous injection Initiation (new start) criteria: Non-formulary lixisenatide/glargine (Soliqua) will be covered on the prescription drug benefit when the following criteria are met: Must meet criteria for both individual agents lixisenatide and insulin glargine. Criteria for lixisenatide: • Diagnosis of Type 2 Diabetes Mellitus • Intolerance to preferred GLP-1 agonists liraglutide (Victoza) AND injectable semaglutide (Ozempic) • No personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2) • No personal history of gastroparesis • On maximally tolerated metformin dose (dose appropriate per renal function) or allergy or intolerance* to metformin (includes both metformin IR and XR) • And meets one of the following criteria: o Inadequate glycemic response on both basal and bolus insulin despite high dose requirements (total daily insulin dose of 1.5 units per kilogram of body weight or more OR greater than 200 units) OR o Has experienced recurrent nocturnal hypoglycemia with basal insulin defined as: 3 or more episodes of nocturnal hypoglycemia (BG less than 70 mg/dL) over the preceding 30 days that persists despite basal insulin dose reduction (including decrease in NPH dose and subsequent switch to and dose adjustment of insulin glargine) Criteria for insulin glargine • Use in patients with type 1 diabetes mellitus as basal insulin -OR- • Use in patients with -

KFHC DRUG FORMULARY Iii Preface FORMULARY
Drug Formulary prescribe generic first TM TM 9700 Stockdale Highway Bakersfield, California 93311-3617 1-800-391-2000 kernfamilyhealthcare.com L NK Drug Formulary February 2020 February 2020 The Kern Family Health Care Drug Formulary includes information boxes prior to some of the major therapeutic categories. Please use these tools to assist with your care of our members. TM This symbol indicates some or all of the dosage forms are available generically. Prescribing generic brands of medication is key to keeping the escalating medication costs down to a minimum. Kern Health Systems PMPM medication cost is approaching $35. 65 This symbol indicates a drug identified by National Committee for Quality Assurance (NCQA) as a high risk medication for the elderly and should generally be avoided for this population. Please consider a formulary alternative. Q This symbol indicates the drug should be billed to Medicare Part B as primary and Kern Family Health Care as a secondary payer. 1 This symbol indicates a tier. It will designate the tier only in regards to cost share. It does not reflect any step-therapy status. KFHC DRUG FORMULARY iii Preface FORMULARY The member identification number will be the CIN number. This is a number assigned by the state and is not the social security number. Kern Family Health Care (KHS Medi-Cal) BIN 600428 PCN 04970000 Pt. Number is CIN Number Formulary OTC’s Covered Formulary Prenatal Vitamins Covered (OTC included) Formulary Contraceptives Covered No copayments TAR’s allowed for OTC and legend PHARMACY AND THERAPEUTICS COMMITTEE The Pharmacy and Therapeutics Committee is composed of Physician and Pharmacist community providers as well as staff from Kern Health Systems. -

Type 2 Diabetes Adult Outpatient Insulin Guidelines
Diabetes Coalition of California TYPE 2 DIABETES ADULT OUTPATIENT INSULIN GUIDELINES GENERAL RECOMMENDATIONS Start insulin if A1C and glucose levels are above goal despite optimal use of other diabetes 6,7,8 medications. (Consider insulin as initial therapy if A1C very high, such as > 10.0%) 6,7,8 Start with BASAL INSULIN for most patients 1,6 Consider the following goals ADA A1C Goals: A1C < 7.0 for most patients A1C > 7.0 (consider 7.0-7.9) for higher risk patients 1. History of severe hypoglycemia 2. Multiple co-morbid conditions 3. Long standing diabetes 4. Limited life expectancy 5. Advanced complications or 6. Difficult to control despite use of insulin ADA Glucose Goals*: Fasting and premeal glucose < 130 Peak post-meal glucose (1-2 hours after meal) < 180 Difference between premeal and post-meal glucose < 50 *for higher risk patients individualize glucose goals in order to avoid hypoglycemia BASAL INSULIN Intermediate-acting: NPH Note: NPH insulin has elevated risk of hypoglycemia so use with extra caution6,8,15,17,25,32 Long-acting: Glargine (Lantus®) Detemir (Levemir®) 6,7,8 Basal insulin is best starting insulin choice for most patients (if fasting glucose above goal). 6,7 8 Start one of the intermediate-acting or long-acting insulins listed above. Start insulin at night. When starting basal insulin: Continue secretagogues. Continue metformin. 7,8,20,29 Note: if NPH causes nocturnal hypoglycemia, consider switching NPH to long-acting insulin. 17,25,32 STARTING DOSE: Start dose: 10 units6,7,8,11,12,13,14,16,19,20,21,22,25 Consider using a lower starting dose (such as 0.1 units/kg/day32) especially if 17,19 patient is thin or has a fasting glucose only minimally above goal. -

Use of Inhaled Human Insulin in Patients with Diabetes Mellitus Meghan K
Volume X, No. I January/February 2007 Mandy C. Leonard, Pharm.D., BCPS Assistant Director, Drug Information Service Editor Use of Inhaled Human Insulin in Patients with Diabetes Mellitus Meghan K. Lehmann, Pharm.D., BCPS by Linda Ghobrial, Pharm.D. Drug Information Specialist Editor I ntroduction: Diabetes mellitus is a concentration >200 mg/dL in the pres- Dana L. Travis, R.Ph. Drug Information Pharmacist metabolic disease characterized by ence of symptoms, or a 2-hour OGTT 2 Editor hyperglycemia and abnormal carbo- value of >200 mg/dL. The diagnosis hydrate, fat, and protein metabolism. is then confirmed by measuring any David A. White, B.S., R.Ph. Diabetes has a very high prevalence one of the three criteria on a subse- Restricted Drug Pharmacist 2 Associate Editor worldwide. There are approximately quent day. 20.8 million (7%) people in the 1 Marcia J. Wyman, Pharm.D. United States who have diabetes. Classification: Most patients with D rug Information Pharmacist Diabetes results from defects in insu- diabetes mellitus are classified as hav- Associate Editor lin secretion, sensitivity, or both. Al- ing either type 1 or type 2. Type 1 Amy T. Sekel, Pharm.D. though the exact cause remains un- diabetes (previously known as juve- D rug Information Pharmacist clear, genetics and environmental fac- nile diabetes) accounts for about 10% IAnss otchiaiste IEsdsituoer tors such as obesity and lack of exer- of all diabetes cases and is usually cise appear to be involved. diagnosed in children and young David Kvancz, M.S., R.Ph., FASHP 2 Chief Pharmacy Officer adults. -

Insulin : Past, Present and Future
2016.5.13. 29th Spring Congress of Korean Diabetes Association Insulin : Past, Present and Future Seung-Hwan Lee, MD, PhD Seoul St.Mary’s Hospital The Catholic Univ. of Korea 본 발표와 관련된 이해관계 • 강의 및 자문료: Sanofi Aventis, Eli Lilly History of glucose-lowering drugs Kahn SE et al. Lancet, 2014 Groundwork for the discovery of insulin Josef Von Mering Oskar Minkowski Paul Langerhans (1849-1908) (1858-1931) (1847-88) pancreatectomy in dog displayed polyuria, small clusters of cells in thirst, hyperphagia pancreas separated from exocrine & ductal tissue demonstrated blood glucose lowering properties of pancreas “islets of Langerhans” Insulin in medical history: 4 Nobel prizes Frederick Sanger Chemistry 1958 Aminoacid sequence of insulin Dorothy Hodgkin Frederick Banting & John Macleod Chemistry 1964 Medicine 1923 X-ray crystallography Discovery of insulin Rosalyn Yalow Medicine 1977 RIA Charles Best James Collip Developments in insulin therapy: a journey not a destination Isolation Hagedorn protamine of insulin -retarded insulin Recombinant human Basal (Banting & Macleod) NPH insulin insulin analogues 1922 1946 1977 2000s Time The beginning 1923 1950s 1990s Animal insulin p Lente® insulin Rapid-acting reparations series insulin analogues NPH, neutral protamine Hagedorn Isolation of insulin • 1921: Banting and Best filter pancreatic tissue to produce ‘isletin’ in Professor Macleod’s laboratory at the University of Toronto • Purification of insulin by Bertram Collip First use of insulin in human January 1922: At Toronto General Hospital, 14-year-old Leonard Thompson was the first human to receive insulin • Banting and Best injected a 14-year-old “charity” patient who weighed 29 kg with 7.5 ml of a “thick brown muck” in each buttock. -

United States Experience of Insulin Degludec Alone Or in Combination for Type 1 and Type 2 Diabetes
Journal name: Drug Design, Development and Therapy Article Designation: Review Year: 2017 Volume: 11 Drug Design, Development and Therapy Dovepress Running head verso: Rendell Running head recto: Degludec insulin in the USA open access to scientific and medical research DOI: http://dx.doi.org/10.2147/DDDT.S132581 Open Access Full Text Article REVIEW United States experience of insulin degludec alone or in combination for type 1 and type 2 diabetes Marc Rendell1,2 Abstract: Insulin degludec has been the product of a sophisticated and systematic biochemical 1The Rose Salter Medical Research engineering program which began with the release of insulin detemir. The goal was to pro- Foundation, 2The Association of duce a long-lasting basal insulin with low individual variability. Certainly, this goal has been Diabetes Investigators, Newport achieved. Degludec has a duration of action approaching twice that of glargine. Another advan- Coast, CA, USA tage of degludec is in its lack of unpredictable copolymerization of added aspart. In several studies, degludec has shown lower rates of nocturnal hypoglycemia than glargine. Degludec can be administered flexibly with a very flat insulin concentration curve at any time of day. Initial US Food and Drug Administration concerns about a possible increase in cardiac events in degludec-treated patients have been allayed by the results of a study targeting individuals with high cardiac risk. Degludec is now marketed in the US competing with glargine. Despite the long duration of action of degludec, attempted administration three times weekly resulted For personal use only. in less effective lowering of glycated hemoglobin and an increased incidence of hypoglycemia compared to daily glargine. -
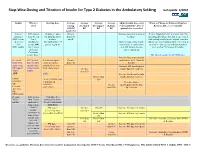
Step-Wise Dosing and Titration of Insulin for Type 2 Diabetes in the Ambulatory Setting Last Update 5/2010
Step -Wise Dosing and Titration of Insulin for Type 2 Diabetes in the Ambulatory Setting last update 5/2010 Insulin When to Starting dose Average Average Average Average Adjust Insulin dose every When to Change to Different Regimen start fasting Pre-lunch Pre-supper Bedtime 3 days until BG < 130, or Recheck A1C every 3 months AM BG BG BG BG optimal dose is reached Goal<130 Lantus A1C greater 10 units or up to Greater Increase dose by 2-4 units at If after 3 months if A1c is greater than 7% (glargine) than 8% on 0.2 units/kg SQ at than 130 bedtime. and optimal bedtime dose has been reached OR Levemir 2 or 3 bedtime mg/dL with fasting blood glucose at goal, consider (detemir) antidiabetic (DC sulfonylurea if Optimal long acting (basal) adding a pre-meal bolus insulin at the largest OR agents OR part of regimen) insulin dose keeps bedtime meal of the day, pre-meal bolus insulin at NPH insulin 1 or 2 agents and AM fasting glucose each meal or 70/30 premix insulin. if Serum values consistent. Creatinine greater than 2 DC all oral agents except Metformin. Increase long acting (basal) Pre-meal A1C greater 2-4 units of rapid Greater insulin dose by 2-4 units at bolus with than 7% with acting or regular than 130 bedtime rapid acting optimal long insulin SQ at each Increase AM rapid/regular OR regular acting (basal) meal (base dose) Greater insulin dose by 2-4 units. insulin insulin. than 130 AND with Increase lunch rapid/regular Greater than insulin dose by 2-4 units. -

New Diabetes Medications: Where Do They Fit in the Paradigm?
NEW DIABETES MEDICATIONS: WHERE DO THEY FIT IN THE PARADIGM? Nabila Ahmed-Sarwar, Pharm.D., BCPS, CDE Elizabeth Sutton Burke, Pharm.D., BCACP, CDE Wegmans School of Pharmacy November 19 th , 2016 Disclosure Statement No relevant financial relationships to disclose Learning Objectives Upon completion of this educational session, participants will be able to: • Summarize current and new targets for drug action that influence glucose homeostasis • Explain the clinical impact of the new therapeutic agents and determine their place in therapy for the treatment of diabetes mellitus Current Treatment Options Location Medications Effect Secretagogues Increase serum insulin DPP-IV Inhibitors levels Insulin Metformin Decrease Thiazolidinediones gluconeogenesis Increase glucose uptake Alpha-glucosidase Decrease glucose Inhibitors absorption Pramlintide American Diabetes Association-Standards of Care. Diabetes Care 2016 Where do we go from here?? Improved Improved Safety Efficacy Alternative Desirable targets for Administration glucose Regimens homeostasis New Anti-hyperglycemic Agents New Treatment Options Location Medications Effect Increase serum insulin levels Basal Insulins GLP-1 Analogs Decrease glucagon release SGLT-2 Inhibitors Increase urinary glucose excretion Where do we go from here?? Improved Improved Safety Efficacy Alternative Desirable targets for Administration glucose Regimens homeostasis New Anti-hyperglycemic Agents Basal-Rapid Acting Regimen Provides continuous basal coverage Insulin 7 amnoon 7 pm 11 pm 7 am Basal Insulins Generic -

Combination Use of Insulin and Incretins in Type 2 Diabetes
Canadian Agency for Agence canadienne Drugs and Technologies des médicaments et des in Health technologies de la santé CADTH Optimal Use Report Volume 3, Issue 1C Combination Use of Insulin and July 2013 Incretins in Type 2 Diabetes Supporting Informed Decisions This report is prepared by the Canadian Agency for Drugs and Technologies in Health (CADTH). The report contains a comprehensive review of the existing public literature, studies, materials, and other information and documentation (collectively the “source documentation”) available to CADTH at the time of report preparation. The information in this report is intended to help Canadian health care decision-makers, health care professionals, health systems leaders, and policy-makers make well-informed decisions and thereby improve the quality of health care services. The information in this report should not be used as a substitute for the application of clinical judgment in respect of the care of a particular patient or other professional judgment in any decision-making process, nor is it intended to replace professional medical advice. While CADTH has taken care in the preparation of this document to ensure that its contents are accurate, complete, and up to date as of the date of publication, CADTH does not make any guarantee to that effect. CADTH is not responsible for the quality, currency, propriety, accuracy, or reasonableness of any statements, information, or conclusions contained in the source documentation. CADTH is not responsible for any errors or omissions or injury, loss, or damage arising from or relating to the use (or misuse) of any information, statements, or conclusions contained in or implied by the information in this document or in any of the source documentation.