RSI and Computer Keyboard Use April 4, 2006 Introduction Repetitive
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Summary Double Your Typing Speed
Summary Double Your Typing Speed.............................................................1 Stenography Benefits......................................................................1 Speed...........................................................................................................................................1 Fluency Of Thought....................................................................................................................2 Ergonomy....................................................................................................................................3 Mobile/Wearable Computing and Augmented Reality...............................................................3 Memorable Customizable Macros..............................................................................................4 Stenography Is Cool, But................................................................5 Open Source Stenography: Who Is Using It...................................5 Then I Saw The Light.....................................................................6 My Contributions............................................................................7 Stenography Is The Way.................................................................8 Machine stenography costs too much.........................................................................................8 Proprietary steno software might be better..................................................................................9 Learning takes too much -
Gesture Keyboard Using Arduino
www.ijcrt.org © 2021 IJCRT | Volume 9, Issue 5 May 2021 | ISSN: 2320-2882 GESTURE KEYBOARD USING ARDUINO P. R. Rodge1 Gawali Harshada2 Chaudhari Pooja3 More Mayur4 1Professor of Computer Engineering Department, SSJCOE, Maharashtra, India 2Student of Computer Engineering Department, SSJCOE, Maharashtra, India 3Student of Computer Engineering Department, SSJCOE. Maharashtra, India 4Student of Computer Engineering Department, SSJCOE, Maharashtra, India ABSTRACT Different keyboards are available in the market, with variations in size, layouts, programs, and functionalities. Recently, virtual keyboards are also in use but for every single keyboard, the user should remember the arrangement of keys in order to enter different characters. Remote-based gesture keyboard is a system that serves on the Internet of Things [IoT] architecture and embedded with Arduino as well as the accelerometer and machine learning process that enforces the system to perform in the desired direction. The remote-based gesture keyboard is the model, where the user can enter text and number in a text editor by moving a hand to the specific motion of characters in the air using Arduino. Arduino operates as a remote where gestures relocate into the air, translating into letters, and exposing them on a computer screen. Keywords— gesture, Arduino, remote, keyboard. I.INTRODUCTION The keyboard plays a vibrant role in the computer system for the entry of data by pressing the number of keys. In today’s generation screen touch keyboards are mostly used and gesture keyboards also used only for physically disabled people and for special use. There is plenty of variation in layouts of the physical keyboard such as AZERTY, QWERTY, Dvorak Colemak, Maltron, and JCUKEN. -

Speech-To-Text Interpreting in Finland, Sweden and Austria Norberg
https://helda.helsinki.fi Speech-to-text interpreting in Finland, Sweden and Austria Norberg, Ulf 2015 Norberg , U , Stachl-Peier , U & Tiittula , L 2015 , ' Speech-to-text interpreting in Finland, Sweden and Austria ' , Translation & Interpreting , vol. 7 , no. 3 , pp. 36-49 . https://doi.org/10.12807/ti.107203.2015.a03 http://hdl.handle.net/10138/162021 https://doi.org/10.12807/ti.107203.2015.a03 Downloaded from Helda, University of Helsinki institutional repository. This is an electronic reprint of the original article. This reprint may differ from the original in pagination and typographic detail. Please cite the original version. Speech-to-text interpreting in Finland, Sweden and Austria The International Journal for Translation & Interpreting Research Ulf Norberg trans-int.org Stockholm University, Sweden [email protected] Ursula Stachl-Peier University of Graz, Austria [email protected] Liisa Tiittula University of Helsinki, Finland [email protected] DOI: 10.12807/ti.107203.2015.a03 Abstract: Speech-to-text (STT) interpreting is a type of intralingual interpreting mostly used by late deafened and hearing impaired persons who have a spoken language as their first language. In Finland, Sweden and Austria the speech-to-text transfer is performed in real-time by interpreters using a (specially adapted or standard) keyboard that is connected to a screen. As a result of different legislative frameworks governing services for the disabled, STT interpreting has developed differently in different countries and so far there has been little international cooperation. STT interpreting has also been largely ignored by Translation and Interpreting Studies. This paper examines the situation in Finland and Sweden, where STT interpreting training programmes have been available since the 1980s, and Austria, where the first training programme started in 2010, and investigates the norms, values and expectations that guide STT interpreters’ practice in the three countries. -

Interaction Techniques for Finger Sensing Input Devices
PreSense: Interaction Techniques for Finger Sensing Input Devices ££ £ £ Jun Rekimoto £ Takaaki Ishizawa Carsten Schwesig Haruo Oba £ Interaction Laboratory ££ Graduate School of Media and Governance Sony Computer Science Laboratories, Inc. Keio University 3-14-13 Higashigotanda Shonan Fujisawa Campus Shinagawa-ku, Tokyo 141-0022 Japan 5322 Endo, Fujisawa 252-8520 Japan Phone: +81 3 5448 4380, Fax +81 3 5448 4273 [email protected] rekimoto,oba @csl.sony.co.jp http://www.csl.sony.co.jp/person/rekimoto.html ABSTRACT Although graphical user interfaces started as imitations of the physical world, many interaction techniques have since been invented that are not available in the real world. This paper focuses on one of these “previewing”, and how a sen- sory enhanced input device called “PreSense Keypad” can provide a preview for users before they actually execute the commands. Preview important in the real world because it is often not possible to undo an action. This previewable fea- Figure 1: PreSense Keypad senses finger contact ture helps users to see what will occur next. It is also helpful (proximity) and position before the key press. when the command assignment of the keypad dynamically changes, such as for universal commanders. We present sev- eral interaction techniques based on this input device, includ- touch sensor, finger motions on the keypad are recognized ing menu and map browsing systems and a text input system. by integrating each keytop’s information. We also discuss finger gesture recognition for the PreSense This sensor and keytop combination makes it possible to rec- Keypad. ognize “which button is about to be pressed”, and the system KEYWORDS: input devices, previewable user interfaces, can provide appropriate information to users. -

Using Action-Level Metrics to Report the Performance of Multi-Step Keyboards
Using Action-Level Metrics to Report the Performance of Multi-Step Keyboards Gulnar Rakhmetulla* Ahmed Sabbir Arif† Steven J. Castellucci‡ Human-Computer Interaction Group Human-Computer Interaction Group Independent Researcher University of California, Merced University of California, Merced Toronto I. Scott MacKenzie§ Caitlyn E. Seim¶ Electrical Engineering and Computer Science Mechanical Engineering York University Stanford University Table 1: Conventional error rate (ER) and action-level unit error rate ABSTRACT (UnitER) for a constructive method (Morse code). This table illustrates Computer users commonly use multi-step text entry methods on the phenomenon of using Morse code to enter “quickly” with one handheld devices and as alternative input methods for accessibility. character error (“l”) in each attempt. ER is 14.28% for each attempt. These methods are also commonly used to enter text in languages One of our proposed action-level metrics, UnitER, gives a deeper with large alphabets or complex writing systems. These methods insight by accounting for the entered input sequence. It yields an error require performing multiple actions simultaneously (chorded) or rate of 7.14% for the first attempt (with two erroneous dashes), and in a specific sequence (constructive) to produce input. However, an improved error rate of 3.57% for the second attempt (with only evaluating these methods is difficult since traditional performance one erroneous dash). The action-level metric shows that learning has metrics were designed explicitly for non-ambiguous, uni-step meth- occurred with a minor improvement in error rate, but this phenomenon ods (e.g., QWERTY). They fail to capture the actual performance of is omitted in the ER metric, which is the same for both attempts. -
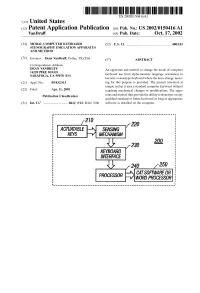
(12) Patent Application Publication (10) Pub. No.: US 2002/0150416A1 Vandruff (43) Pub
US 2002O150416A1 '(19) United States (12) Patent Application Publication (10) Pub. No.: US 2002/0150416A1 VanDruff (43) Pub. Date: Oct. 17, 2002 (54) MODAL COMPUTER KEYBOARD (52) U.S. Cl. .............................................................. 400/103 STENOGRAPHY EMULATION APPARATUS AND METHOD (76) Inventor: Dean VanDruff, Dallas, TX (US) (57) ABSTRACT Correspondence Address: DEAN VANDRUFF An apparatus and method to change the mode of computer 1422O PIKE ROAD SARATOGA, CA 95070 (US) keyboard use from alpha-numeric language orientation to become a Stenotype keyboard where the keys change mean (21) Appl. No.: 09/832,915 ing for this purpose is provided. The present invention is unique in that it uses a Standard computer keyboard without (22) Filed: Apr. 11, 2001 requiring mechanical changes or modifications. The appa Publication Classification ratus and method thus provide the ability to Stenotype on any qualified Standard or future keyboard as long as appropriate (51) Int. Cl." .................................. B41J 5/12; B41J 5/08 Software is installed on the computer. 220 SEWSNG MECHAWS 230 200 KEYBOARD INTERFACE 250 CATSOFTWARE OR WORD PROCESSOR Patent Application Publication Oct. 17, 2002 Sheet 1 of 2 US 2002/0150416A1 FIG. A 202 208 204 216 HOSTIPCI MAIN AUDIO B 206 210 214 218 219 - - - - - - - - - - - A232 LAN EXPANSION BUS GRAPHICS AUDIO/WIDEO HOSTBUSADAPER n 220 222 224 1/ !----Y---------- 200 FIG. 1B 20 220 ACTUATABLE SEWSNG MECHANISM KEYBOARD FIG 2 INTERFACE 250 PROCESSOR CATSOFTWAREPREESSR OR Patent Application Publication Oct. 17, 2002 Sheet 2 of 2 US 2002/0150416A1 UMBER BAR 1 2 3 4 6 7, 8 9 PPER BANK Swest." W 5 0 g WO WEL BANK FIG. -

An Improved Arabic Keyboard Layout
Sci.Int.(Lahore),33(1),5-15,2021 ISSN 1013-5316; CODEN: SINTE 8 5 AN IMPROVED ARABIC KEYBOARD LAYOUT 1Amjad Qtaish, 2Jalawi Alshudukhi, 3Badiea Alshaibani, 4Yosef Saleh, 5Salam Bazrawi College of Computer Science and Engineering, University of Ha'il, Ha'il, Saudi Arabia. [email protected], [email protected], [email protected], [email protected], [email protected] ABSTRACT: One of the most important human–machine interaction (HMI) systems is the computer keyboard. The keyboard layout (KL) dictates how a person interacts with a physical keyboard through the way in which the letters, numbers, punctuation marks, and symbols are mapped and arranged on the keyboard. Mapping letters onto the keys of a keyboard is complex because many issues need to be taken into considerations, such as the nature of the language, finger fatigue, hand balance, typing speed, and distance traveled by fingers during typing and finger movements. There are two main kinds of KL: English and Arabic. Although numerous research studies have proposed different layouts for the English keyboard, there is a lack of research studies that focus on the Arabic KL. To address this lack, this study analyzed and clarified the limitations of the standard legacy Arabic KL. Then an efficient Arabic KL was proposed to overcome the limitations of the current KL. The frequency of Arabic letters and bi-gram probabilities were measured on a large Arabic corpus in order to assess the current KL and to design the improved Arabic KL. The improved Arabic KL was then evaluated and compared against the current KL in terms of letter frequency, finger-travel distance, hand and finger balance, bi-gram frequency, row distribution, and most frequent words. -

Senorita: a Chorded Keyboard for Sighted, Low Vision, and Blind
Senorita: A Chorded Keyboard for Sighted, Low Vision, and Blind Mobile Users Gulnar Rakhmetulla Ahmed Sabbir Arif Human-Computer Interaction Group Human-Computer Interaction Group University of California, Merced University of California, Merced Merced, CA, United States Merced, CA, United States [email protected] [email protected] Figure 1. With Senorita, the left four keys are tapped with the left thumb and the right four keys are tapped with the right thumb. Tapping a key enters the letter in the top label. Tapping two keys simultaneously (chording) enters the common letter between the keys in the bottom label. The chord keys are arranged on opposite sides. Novices can tap a key to see the chords available for that key. This figure illustrates a novice user typing the word “we”. She scans the keyboard from the left and finds ‘w’ on the ‘I’ key. She taps on it with her left thumb to see all chords for that key on the other side, from the edge: ‘C’, ‘F’, ‘W’, and ‘X’ (the same letters in the bottom label of the ‘I’ key). She taps on ‘W’ with her right thumb to form a chord to enter the letter. The next letter ‘e’ is one of the most frequent letters in English, thus has a dedicated key. She taps on it with her left thumb to complete the word. ABSTRACT INTRODUCTION Senorita is a novel two-thumb virtual chorded keyboard for Virtual Qwerty augmented with linguistic and behavioral mod- mobile devices. It arranges the letters on eight keys in a single els has become the dominant input method for mobile devices. -

Gesture Typing on Smartwatches Using a Segmented QWERTY Around the Bezel
SwipeRing: Gesture Typing on Smartwatches Using a Segmented QWERTY Around the Bezel Gulnar Rakhmetulla* Ahmed Sabbir Arif† Human-Computer Interaction Group Human-Computer Interaction Group University of California, Merced University of California, Merced Figure 1: SwipeRing arranges the standard QWERTY layout around the edge of a smartwatch in seven zones. To enter a word, the user connects the zones containing the target letters by drawing gestures on the screen, like gesture typing on a virtual QWERTY. A statistical decoder interprets the input and enters the most probable word. A suggestion bar appears to display other possible words. The user could stroke right or left on the suggestion bar to see additional suggestions. Tapping on a suggestion replaces the last entered word. One-letter and out-of-vocabulary words are entered by repeated strokes from/to the zones containing the target letters, in which case the keyboard first enters the two one-letter words in the English language (see the second last image from the left), then the other letters in the sequence in which they appear in the zones (like multi-tap). Users could also repeatedly tap (instead of stroke) on the zones to enter the letters. The keyboard highlights the zones when the finger enters them and traces all finger movements. This figure illustrates the process of entering the phrase “the world is a stage” on the SwipeRing keyboard (upper sequence) and on a smartphone keyboard (bottom sequence). We can clearly see the resemblance of the gestures. ABSTRACT player or rejecting a phone call), checking notifications on incoming Most text entry techniques for smartwatches require repeated taps to text messages and social media posts, and using them as fitness enter one word, occupy most of the screen, or use layouts that are trackers to record daily physical activity. -

Text Input Methods for Indian Languages Sowmya Vajjala, International Institute of Information Technology
Iowa State University From the SelectedWorks of Sowmya Vajjala 2011 Text Input Methods for Indian Languages Sowmya Vajjala, International Institute of Information Technology Available at: https://works.bepress.com/sowmya-vajjala/3/ TEXT INPUT METHODS FOR INDIAN LANGUAGES By Sowmya V.B. 200607014 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF Master of Science (by Research) in Computer Science & Engineering Search and Information Extraction Lab Language Technologies Research Center International Institute of Information Technology Hyderabad, India September 2008 Copyright c 2008 Sowmya V.B. All Rights Reserved Dedicated to all those people, living and dead, who are directly or indirectly responsible to the wonderful life that I am living now. INTERNATIONAL INSTITUTE OF INFORMATION TECHNOLOGY Hyderabad, India CERTIFICATE It is certified that the work contained in this thesis, titled “ Text input methods for Indian Languages ” by Sowmya V.B. (200607014) submitted in partial fulfillment for the award of the degree of Master of Science (by Research) in Computer Science & Engineering, has been carried out under my supervision and it is not submitted elsewhere for a degree. Date Advisor : Dr. Vasudeva Varma Associate Professor IIIT, Hyderabad Acknowledgements I would like to first express my gratitude to my advisor Dr Vasudeva Varma, for being with me and believing in me throughout the duration of this thesis work. His regular suggestions have been greatly useful. I thank Mr Prasad Pingali for his motivation and guidance during the intial phases of my thesis. I thank Mr Bhupal Reddy for giving me the first lessons in my research. I entered IIIT as a novice to Computer Science in general and research in particular. -

Clavier DUCK
Clavier DUCK : Utilisation d'un syst`emede d´eduction de mots pour faciliter la saisie de texte sur ´ecrantactile pour les non-voyants Philippe Roussille, Mathieu Raynal, Christophe Jouffrais To cite this version: Philippe Roussille, Mathieu Raynal, Christophe Jouffrais. Clavier DUCK : Utilisation d'un syst`emede d´eduction de mots pour faciliter la saisie de texte sur ´ecrantactile pour les non- voyants. 27`eme conf´erencefrancophone sur l'Interaction Homme-Machine., Oct 2015, Toulouse, France. ACM, IHM-2015, pp.a19, 2015, <10.1145/2820619.2820638>. <hal-01218748> HAL Id: hal-01218748 https://hal.archives-ouvertes.fr/hal-01218748 Submitted on 21 Oct 2015 HAL is a multi-disciplinary open access L'archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destin´eeau d´ep^otet `ala diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publi´esou non, lished or not. The documents may come from ´emanant des ´etablissements d'enseignement et de teaching and research institutions in France or recherche fran¸caisou ´etrangers,des laboratoires abroad, or from public or private research centers. publics ou priv´es. Clavier DUCK : Utilisation d’un système de déduction de mots pour faciliter la saisie de texte sur écran tactile pour les non-voyants. Philippe Roussille Mathieu Raynal Christophe Jouffrais Université de Toulouse & Université de Toulouse & CNRS & Université de CNRS ; IRIT ; CNRS ; IRIT ; Toulouse ; IRIT ; F31 062 Toulouse, France F31 062 Toulouse, France F31 062 Toulouse, France [email protected] [email protected] [email protected] RÉSUMÉ fournissant des claviers logiciels qui s’affichent sur ces L’utilisation des écrans tactiles et en particulier les cla- surfaces tactiles. -

Manual Text Entry Remains One of the Dominant Forms of Human- Computer Interaction
Poika Isokoski Manual Text Input: Experiments, Models, and Systems academic dissertation To be presented, with the permission of the Faculty of Information Sciences of the University of Tampere, for public discussion in Auditorium A1 on April 23rd, 2004, at noon. department of computer sciences university of tampere A-2004-3 tampere 2004 Supervisor: Professor Roope Raisamo Department of Computer Sciences University of Tampere, Finland Opponent: Dr. Shumin Zhai IBM Almaden Research Center, USA Reviewers: Professor Heikki Mannila Basic Research Unit Helsinki Institute for Information Technology, Finland Professor Ari Visa Signal Processing Laboratory Tampere University of Technology, Finland Department of Computer Sciences FIN-33014 UNIVERSITY OF TAMPERE Finland Electronic dissertation Acta Electronica Universitatis Tamperensis 340 ISBN 951-44-5959-8 ISSN 1456-954X http://acta.uta.fi ISBN 951-44-5955-5 ISSN 1459-6903 Tampereen yliopistopaino Oy Tampere 2004 Abstract Despite the emergence of speech controlled computers and direct manipula- tion that both have diminished the need to operate computers with textual commands, manual text entry remains one of the dominant forms of human- computer interaction. This is because textual communication is one of the main reasons for using computers. Mobile and pervasive computing have been popular research areas re- cently. Thus, these issues have a major part in the thesis at hand. Most of the text entry methods that are discussed are for mobile computers. One of the three main contributions of the work is an architecture for a middle- ware system intended to support personalized text entry in an environment permeated with mobile and non-mobile computers. The two other main contributions in this thesis are experimental work on text entry methods and models of user performance in text entry tasks.