Deep Overbite Malocclusion M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

V September 2006
CORRELATING POSITION OF HYOID BONE AND MANDIBLE TO THIRD CERVICAL VERTEBRA IN PATIENTS WITH CLASS I, CLASS II AND CLASS III SKELETAL MALOCCLUSION – A CEPHALOMETRIC STUDY Dissertation Submitted to THE TAMIL NADU DR.M.G.R. MEDICAL UNIVERSITY Towards the partial fulfillment for the degree of MASTER OF DENTAL SURGERY BRANCH – V ORTHODONTICS SEPTEMBER 2006 Certificate This is to certify that Dr. VIJJAYKANTH Post Graduate Student (2003-2006) in the Department of Orthodontics, Tamilnadu Government Dental College & Hospital, Chennai has done this dissertation titled “CORRELATING POSITION OF HYOID BONE AND MANDIBLE TO THIRD CERVICAL VERTEBRA IN PATIENTS WITH CLASS I, CLASS II AND CLASS III SKELETAL MALOCCLUSION – A CEPHALOMETRIC STUDY” under our guidance and supervision in partial fulfillment of the regulations laid down by the Tamilnadu Dr.M.G.R. Medical University, Chennai for M.D.S., Branch – V Orthodontics, Degree Examination. Dr.L.Muthusamy, M.D.S., Dr.W.S.Manjula, M.D.S., Professor and Head, Additional Professor, Department of Orthodontics Department of Orthodontics Tamilnadu Govt. Dental College and Hospital, Tamilnadu Govt. Dental College and Hospital, Chennai-600 003. Chennai-600 003. Dr.C. Kumaravelu, M.D.S., Principal Tamilnadu Govt. Dental College and Hospital, Chennai-600 003. C O N T E N T S PAGE NO. 1 INTRODUCTION 01 2 AIMS AND OBJECTIVES 04 3 REVIEW OF LITERATURE 05 4 MATERIALS AND METHODS 24 5 RESULTS 29 6 DISCUSSION 41 7 SUMMARY AND CONCLUSION 50 8 BIBLIOGRAPHY 52 LIST OF BAR DIAGRAMS Bar Diagram Bar Diagram Title No 1. Cephalometric mean and standard deviation for each group Cephalometric mean values for male and female subjects for each 2. -

Therapeutic Management of Patients with Class III Skeletal Malocclusion
Szpyt Justyna, Gębska Magdalena. Therapeutic management of patients with class III skeletal malocclusion. Mandibular prognathism, maxillary retrognathism – a case report. Journal of Education, Health and Sport. 2019;9(5):20-31. eISSN 2391-8306. DOI http://dx.doi.org/10.5281/zenodo.2656446 http://ojs.ukw.edu.pl/index.php/johs/article/view/6872 https://pbn.nauka.gov.pl/sedno-webapp/works/912455 The journal has had 7 points in Ministry of Science and Higher Education parametric evaluation. Part B item 1223 (26/01/2017). 1223 Journal of Education, Health and Sport eISSN 2391-8306 7 © The Authors 2019; This article is published with open access at Licensee Open Journal Systems of Kazimierz Wielki University in Bydgoszcz, Poland Open Access. This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author (s) and source are credited. This is an open access article licensed under the terms of the Creative Commons Attribution Non commercial license Share alike. (http://creativecommons.org/licenses/by-nc-sa/4.0/) which permits unrestricted, non commercial use, distribution and reproduction in any medium, provided the work is properly cited. The authors declare that there is no conflict of interests regarding the publication of this paper. Received: 15.04.2019. Revised: 25.04.2019. Accepted: 01.05.2019. Therapeutic management of patients with class III skeletal malocclusion. Mandibular prognathism, maxillary retrognathism – a case report Justyna Szpyt1, Magdalena Gębska2 1. Physiotherapy student, Faculty of Health Sciences, Pomeranian Medical University in Szczecin. -

Pan Imaging News V3 I4
Volume 4, Issue 4 US $6.00 Editor: Allan G. Farman, BDS, PhD (odont.), Assessing Growth and Development with Panoramic DSc (odont.), Diplomate of the Radiographs and Cephalometric Attachments: A critical American Board of Oral and Maxillofacial Radiology, Professor of tool for dental diagnosis and treatment planning Radiology and Imaging Sciences, Department of Surgical and Hospital By Dr. Allan G. Farman Dentistry, The University of It is recommended that radio- indicator of age is that the three Louisville School of Dentistry, graphs be made periodically including permanent molar teeth in each quad- Louisville, KY. both during the mixed dentition (8-9 rant erupt approximately at six-year year old) and adolescence (12-14 year intervals. The first permanent molar Featured Article: old) to evaluate growth and develop- erupts around 6 years, the second Assessing Growth and Development ment, and to look for asymptomatic permanent molar around 12 years, and with Panoramic Radiographs and dental disease [1-3]. Substantial the third molars around 18 years. Root Cephalometric Attachments: A critical differences in the assessed biological formation for permanent teeth is tool for dental diagnosis and and the known chronological age can completed roughly three years following treatment planning be indicators of a variety of inherited eruption. The first major attempt at and congenital conditions. Further, local developing a chronology for human In The Recent Literature: failure in dental eruption within the tooth development was that of Logan normal time range can be evidence of and Kronfeld (1933) and with minor Implantology dental impaction and possibly of a modification is still usable as a rough pathological process such as a hamar- and ready guide. -

The National Dental Practice-Based Research Network Adult Anterior
ORIGINAL ARTICLE The National Dental Practice-Based Research Network Adult Anterior Open Bite Study: Treatment recommendations and their association with patient and practitioner characteristics Greg Huang,a Camille Baltuck,b Ellen Funkhouser,c Hsuan-Fang (Cathy) Wang,a,d Lauren Todoki,a Sam Finkleman,a Peter Shapiro,a Roozbah Khosravi,a Hsiu-Ching (Joanna) Ko,a Geoffrey Greenlee,a Jaime De Jesus-Vinas,e Michael Vermette,f Matthew Larson,g Calogero Dolce,h Chung How Kau,i and David Harnick,j and the National Dental Practice-Based Research Network Collaborative Groupk Seattle, Wash, Portland, Ore, Birmingham, Ala, Taipei, Taiwan, San Juan, PR, Concord, NH, Eau Claire, Wis, Gainesville, Fla, and Albuquerque, NM Introduction: This aim of this paper is to describe and identify the practitioner and patient characteristics that are associated with treatment recommendations for adult anterior open bite patients across the United States. Methods: Practitioners and patients were recruited within the framework of the National Dental Practice-Based Research Network. Practitioners were asked about their demographic characteristics and their treatment recommendations for these patients. The practitioners also reported on their patients' dentofacial characteristics and provided initial cephalometric scans and intraoral photographs. Patients were asked about their demographic characteristics, previous orthodontic treatment, and goals for treatment. Four main treatment groups were evaluated: aligners, fixed appliances, temporary anchorage devices (TADs), and orthognathic surgery. Extractions were also investigated. Predictive multivariable models were created comparing various categories of treatment as well as extraction/nonextraction decisions. Results: Ninety-one practitioners (mostly orthodontists) and 347 patients were recruited from October 2015 to December 2016. Increased aligner recommendations were associated with white and Asian patients, the presence of tongue habits, and female practitioners. -

Granular Cell Tumour of the Tongue in a 17Yearold Orthodontic Patient: A
bs_bs_banner Oral Surgery ISSN 1752-2471 CASE REPORT Granular cell tumour of the tongue in a 17-year-old orthodontic patient: a case report P.Hita-Davis1, P.Edwards2, S. Conley3 & T.J.Dyer4 1Oral Maxillofacial Surgery, School of Dentistry, Ann Arbor, MI, USA 2Department of Oral Pathology,Medicine and Radiology, Indiana University, Indianapolis, IN, USA 3Department of Orthodontics and Pediatric Dentistry, University of Michigan, Ann Arbor, MI, USA 4Oral Surgery, Boston University, Boston, MA, USA Key words: Abstract cyst, diagnosis, examination To describe the clinical presentation of a granular cell tumour (GCT) in an Correspondence to: orthodontic patient, as well as discuss its aetiology and treatment of Dr P Hita-Davis choice. We present a case of GCT of the tongue in an otherwise healthy Oral Maxillofacial Surgery 17-year-old male patient along with a brief review of literature on GCTs. School of Dentistry The lesion was surgically excised and orthodontic treatment was success- 1011 N. University Avenue Ann Arbor, MI 48109 fully finalised. Clinically, GCTs are indistinguishable from other benign USA connective tissue and neural tissue neoplasms and may be found in any Tel.:+1 734 764 1542 site, with cases commonly involving the gastrointestinal system, breast Fax: +1 734 615 8399 and lung. However, over 50% of cases involve the head and neck, with email: [email protected] the tongue being the most frequently involved site (65–85% of oral GCTs). GCTs demonstrate a close anatomical relationship with peripheral Accepted: 6 June 2013 nerve fibres and demonstrate the presence of myelin and axon-like doi:10.1111/ors.12055 structures thus lending credence to their neural origin. -
The Effectiveness of Tipback Mechanics for Correction of Class II Malocclusion" (2014)
University of Connecticut OpenCommons@UConn Master's Theses University of Connecticut Graduate School 7-3-2014 The ffecE tiveness of Tipback Mechanics for Correction of Class II Malocclusion Nandakumar Janakiraman University of Connecticut School of Medicine and Dentistry, [email protected] Recommended Citation Janakiraman, Nandakumar, "The Effectiveness of Tipback Mechanics for Correction of Class II Malocclusion" (2014). Master's Theses. 632. https://opencommons.uconn.edu/gs_theses/632 This work is brought to you for free and open access by the University of Connecticut Graduate School at OpenCommons@UConn. It has been accepted for inclusion in Master's Theses by an authorized administrator of OpenCommons@UConn. For more information, please contact [email protected]. The Effectiveness of Tipback Mechanics for Correction of Class II Malocclusion. Nandakumar Janakiraman B.D.S. Government Dental College, Bangalore University, 1997. M.D.S. Government Dental College, NTR University, 2002. A Thesis Submitted in Partial Fulfillment of the Requirements for the Degree of Masters of Dental Science at the University of Connecticut 2014 i APPROVAL PAGE Master of Dental Science Thesis The Effectiveness of Tipback Mechanics for Correction of Class II Malocclusion Presented by Nandakumar Janakiraman, BDS, MDS Major Advisor________________________________________________ Flavio A. Uribe DDS, MDentSc Associate Advisor_____________________________________________ Ravindra Nanda BDS, MDS, PhD Associate Advisor_____________________________________________ David Shafer DMD University of Connecticut 2014 ii Acknowledgments I want to thank my parents, my wife and kids for all the sacrifices they make to make my dream come true. I want to thank Dr. Nanda, Dr. Uribe and School of Dental Medicine, University of Connecticut, for their support, encouragement, constant guidance and making my dream of becoming an Orthodontist in US. -

Common Icd-10 Dental Codes
COMMON ICD-10 DENTAL CODES SERVICE PROVIDERS SHOULD BE AWARE THAT AN ICD-10 CODE IS A DIAGNOSTIC CODE. i.e. A CODE GIVING THE REASON FOR A PROCEDURE; SO THERE MIGHT BE MORE THAN ONE ICD-10 CODE FOR A PARTICULAR PROCEDURE CODE AND THE SERVICE PROVIDER NEEDS TO SELECT WHICHEVER IS THE MOST APPROPRIATE. ICD10 Code ICD-10 DESCRIPTOR FROM WHO (complete) OWN REFERENCE / INTERPRETATION/ CIRCUM- STANCES IN WHICH THESE ICD-10 CODES MAY BE USED TIP:If you are viewing this electronically, in order to locate any word in the document, click CONTROL-F and type in word you are looking for. K00 Disorders of tooth development and eruption Not a valid code. Heading only. K00.0 Anodontia Congenitally missing teeth - complete or partial K00.1 Supernumerary teeth Mesiodens K00.2 Abnormalities of tooth size and form Macr/micro-dontia, dens in dente, cocrescence,fusion, gemination, peg K00.3 Mottled teeth Fluorosis K00.4 Disturbances in tooth formation Enamel hypoplasia, dilaceration, Turner K00.5 Hereditary disturbances in tooth structure, not elsewhere classified Amylo/dentino-genisis imperfecta K00.6 Disturbances in tooth eruption Natal/neonatal teeth, retained deciduous tooth, premature, late K00.7 Teething syndrome Teething K00.8 Other disorders of tooth development Colour changes due to blood incompatability, biliary, porphyria, tetyracycline K00.9 Disorders of tooth development, unspecified K01 Embedded and impacted teeth Not a valid code. Heading only. K01.0 Embedded teeth Distinguish from impacted tooth K01.1 Impacted teeth Impacted tooth (in contact with another tooth) K02 Dental caries Not a valid code. Heading only. -

Dental Health Following Cancer Treatment
Survivorship Clinic Dental health following cancer treatment Treatment for cancer often increases the risk for dental problems. As a cancer survivor, it is important for you to understand the reasons why dental care is especially important for maintaining your health. What are the risk factors for dental problems after cancer treatment? Treatment with chemotherapy before your permanent teeth were fully formed. Radiation that included the mouth and/or salivary glands, such as the following: Cranial (whole brain) Craniospinal Nasopharyngeal (nose and throat) Oropharyngeal (mouth and throat) Orbital Eye Ear Infratemporal (midfacial area behind the cheekbones) Cervical (neck) Cervical spine (spine in the neck area) Mantle (neck and chest areas) Total body irradiation (TBI) What dental problems can occur following treatment for cancer? Problems that may be a result of chemotherapy include: Increased risk for cavities Shortening or thinning of the roots of the teeth Absence of teeth or roots Problems with development of tooth enamel resulting in white or discolored patches on the teeth, grooves and pits in the teeth, and/or Easy staining of the teeth Because teeth develop slowly, these problems are more likely to develop in people who received chemotherapy over a prolonged period (several years). Fred Hutchinson Cancer Research Center Survivorship Program Survivorship Clinic Problems that may be a result of radiation to the mouth and/or salivary glands include: Increased risk for cavities Shortening or thinning of the roots -
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations
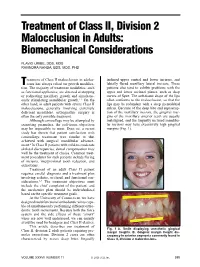
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD reatment of Class II malocclusion in adoles- inclined upper central and lower incisors, and Tcents has always relied on growth modifica- labially flared maxillary lateral incisors. These tion. The majority of treatment modalities, such patients also tend to exhibit problems with the as functional appliances, are directed at stopping upper and lower occlusal planes, such as deep or redirecting maxillary growth and simultane- curves of Spee. The soft-tissue drape of the lips ously stimulating mandibular growth.1-3 On the often conforms to the malocclusion, so that the other hand, in adult patients with severe Class II lips may be redundant with a deep mentolabial malocclusions, generally involving extremely sulcus. Because of the deep bite and supraerup- deficient mandibles, orthognathic surgery is tion of the maxillary incisors, the gingival mar- often the only possible treatment. gins of the maxillary anterior teeth are usually Although camouflage may be attempted by malaligned, and the lingually inclined mandibu- extracting premolars, the soft-tissue objectives lar incisors may have excessively high gingival may be impossible to meet. Even so, a recent margins (Fig. 1). study has shown that patient satisfaction with camouflage treatment was similar to that achieved with surgical mandibular advance- ment.4 In Class II patients with mild-to-moderate skeletal discrepancies, dental compensation may well be the treatment of choice. Common treat- ment procedures for such patients include flaring of incisors, interproximal tooth reduction, and extractions. Treatment of an adult Class II patient requires careful diagnosis and a treatment plan involving esthetic, occlusal, and functional con- siderations.5-7 The treatment objectives must include the chief complaint of the patient, and A the mechanics plan should be individualized based on the specific treatment goals. -

Congenital Hypothyrodism and Its Oral Manifestations Hipotiroidismo Congénito Y Sus Manifestaciones Bucales
www.medigraphic.org.mx Revista Odontológica Mexicana Facultad de Odontología Vol. 18, No. 2 April-June 2014 pp 133-138 CASE REPORT Congenital hypothyrodism and its oral manifestations Hipotiroidismo congénito y sus manifestaciones bucales Marxy E Reynoso Rodríguez,* María A Monter García,§ Ignacio Sánchez FloresII ABSTRACT RESUMEN Hypothyroidism is one of the most common thyroid disorders. El hipotiroidismo es el más común de los trastornos de la tiroides, Hypothyroidism can be congenital in cases when the thyroid puede ser congénito si la glándula tiroides no se desarrolla correc- gland does not develop normally. Female predominance is a tamente (hipotiroidismo congénito). La predominancia femenina es characteristic of congenital hypothyroidism. Dental characteristics una característica. Entre las características odontológicas del hi- of hypothyroidism are thick lips, a large-sized tongue which, due potiroidismo se observan labios gruesos, lengua de gran tamaño, to its position, can elicit anterior open bite as well as fanned-out que debido a su posición suele producir mordida abierta anterior y anterior teeth. In these cases, delayed eruption of primary and dientes anteriores en abanico, destaca que la dentición temporal y permanent dentitions can be observed, and teeth, even though permanente presentan un retardo eruptivo característico y, aunque normal-sized, are crowded due to the small-sized jaws. This study los dientes son de tamaño normal, suelen estar apiñados por el ta- presents clinical cases of female patients diagnosed with congenital maño pequeño de los maxilares. Se presentan dos casos clínicos hypothyroidism who sought treatment at the Dental Pediatrics Unit de pacientes de sexo femenino que acuden a la clínica de Especia- of the Autonomous University of the State of Mexico. -

Single Nucleotide Polymorphisms (Snps) of COL1A1 and COL11A1 in Class II Skeletal Malocclusion of Ethnic Javanese Patient
Clinical, Cosmetic and Investigational Dentistry Dovepress open access to scientific and medical research Open Access Full Text Article ORIGINAL RESEARCH Single Nucleotide Polymorphisms (SNPs) of COL1A1 and COL11A1 in Class II Skeletal Malocclusion of Ethnic Javanese Patient This article was published in the following Dove Press journal: Clinical, Cosmetic and Investigational Dentistry I Gusti Aju Wahju Ardani1 Background: The prevalence of malocclusion cases in the orthodontic specialist clinic in Aulanni’am2 Airlangga University’s Dental Hospital in Surabaya, Indonesia, in 2014–2016 is fairly high, Indeswati Diyatri3 as 55.34% of the occurrences were identified as class II skeletal malocclusion. This type of skeletal malocclusion, which is usually recognized in adults, occurs as a result of variation 1Orthodontics Department, Faculty of Dental Medicine, Airlangga University, during growth and development. Lately, there have been many reports on gene polymorph- Surabaya, Indonesia; 2Biochemistry isms of COL1A1 and COL11A1, which are assumed to be associated with class II skeletal Department, Faculty of Veterinary malocclusion in Caucasians. Medicine, Brawijaya University, Malang, Indonesia; 3Oral Biology, Faculty of Purpose: This study aims to analyze the relationship between single nucleotide polymorph- Dental Medicine, Airlangga University, isms (SNPs) of COL1A1 and COL11A1 with class II skeletal malocclusion in Javanese Surabaya, Indonesia ethnic group patients with mandibular micrognathism. Materials and Methods: The diagnosis of class II skeletal malocclusion was established using the lateral cephalometric radiographs (ANB angle ≥4°) (n=50). DNA was extracted from the patient’s peripheral blood. After that, PCR, electrophoresis, and DNA sequencing were conducted on the extracted DNA based on COL1A1 and COL11A1 primers. Results: The SNPs in COL1A1 are c.20980G/A in 27 patients and c.20980G>A in 8 patients, whereas SNPs in COL11A1 are both c.134373C/A and c.134555C/T in 8 patients and both c.[134373A>C] and c.134582G>A in 10 patients.