Treating Adult Patients with Bilateral Posterior Crossbite, Vertical Growth Pattern and Class II Division 1 Malocclusion with the Invisalign System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular Tads by Randy J
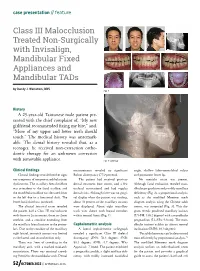
case presentation // feature Class III Malocclusion Treated Non-Surgically with Invisalign, Mandibular Fixed Appliances and Mandibular TADs by Randy J. Weinstein, DDS Fig. 1 History A 25-year-old Taiwanese male patient pre- sented with the chief complaint of, “My new girlfriend recommended fixing my bite,” and, “More of my upper and lower teeth should touch.” The medical history was unremark- able. The dental history revealed that, as a teenager, he received non-extraction ortho- dontic therapy for an unknown correction with removable appliance. Fig. 2: Overlay Clinical findings measurements revealed no significant angle, shallow labio-mentolabial sulcus Clinical findings revealed neither signs Bolton discrepancy (77.9 percent). and prominent lower lip. nor symptoms of temporomandibular joint The patient had received previous No mentalis strain was present. dysfunction. The maxillary dental midline dental treatment (one crown, and a few Although facial evaluation revealed man- was coincident to the facial midline, and occlusal restorations) and had regular dibular prognathism and possibly maxillary the mandibular midline was deviated 2mm dental visits. Although there was no gingi- deficiency (Fig. 2), a proportional analysis, to the left due to a functional shift. The val display when the patient was smiling, such as the modified Moorrees mesh lower facial third was increased. about 70 percent of the maxillary incisors diagram analysis using the Chinese adult The clinical intraoral exam revealed were displayed. About eight maxillary norms, was computed (Fig. 3). This dia- the patient had a Class III malocclusion teeth were shown with buccal corridors gram reveals proclined maxillary incisors with 0mm to 2mm overjet, 0mm to -2mm within normal limits (Fig. -

Comparison of a Tridimensional Cephalometric Analysis Performed
Maspero et al. Progress in Orthodontics (2019) 20:40 https://doi.org/10.1186/s40510-019-0293-x RESEARCH Open Access Comparison of a tridimensional cephalometric analysis performed on 3T- MRI compared with CBCT: a pilot study in adults Cinzia Maspero1,2*† , Andrea Abate1,2†, Francesca Bellincioni1,2†, Davide Cavagnetto1,2†, Valentina Lanteri1,2, Antonella Costa1 and Marco Farronato1,2 Abstract Objective: Since the introduction of cone-beam computed tomography (CBCT) in dentistry, this technology has enabled distortion-free three-dimensional cephalometric analysis for orthodontic and orthognathic surgery diagnosis. However, CBCT is associated with significantly higher radiation exposure than traditional routine bidimensional examinations for orthodontic diagnosis, although low-dose protocols have markedly reduced radiation exposure over time. The objective of this preliminary feasibility study is to compare the accuracy and diagnostic capabilities of an already-validated three-dimensional cephalometric analysis on CBCT to those of an analysis on 3-T magnetic resonance imaging (3T-MRI) to assess whether the latter can deliver a comparable quality of information while avoiding radiation exposure. Materials and methods: In order to test the feasibility of three-dimensional cephalometry on 3T-MRI, 18 subjects (4 male; 14 female) with mean age 37.8 ± SD 10.2, who had undergone both maxillofacial CBCT and maxillofacial 3T-MRI for various purposes within 1 month, were selected from the archive of the Department of Dentistry and Maxillofacial Surgery of Fondazione Ospedale Policlinico Maggiore, IRCCS, Milano, Italy. A three-dimensional cephalometric analysis composed of ten midsagittal and four bilateral landmarks and 24 measurements (11 angular, 13 linear) was performed on both scans using Mimics Research® v. -

Treatment Options for Jaw Growth Variations
TREATMENT OPTIONS FOR JAW GROWTH VARIATIONS An Editorial by Robert M. Mason, DMD, PhD PROBLEMS OF OVERGROWTH OF A JAW: It is well known among orthodontists that where there is a growth process involving overgrowth of a jaw, the rule is that growth should be allowed to proceed and then treat the situation after growth has ceased. The reason for this is that growth cannot be effectively stopped or otherwise modified to the extent that jaw growth can be overpowered; that is, “Mother Nature” is smarter than any of us in dentistry. What can be accomplished with an overgrowth of a jaw, however, is orthodontic “remodeling” of some of the parts which are expressing overgrowth. An example is a Class III “growing” mandible. Functional appliances, such as the Frankel or Bionator, can influence the shape of the growing mandible by remodeling, which may give the appearance of manipulating growth, while instead, long-term studies show that such jaw shape changes are only temporary. Over time, the overgrowth pattern returns. Hence, the orthodontic caveat: it is best to let a mandible grow to its full extent and then treat it either by a combination of jaw surgery and orthodontics, or orthodontics alone which may amount to “camouflaging” the problem. What happens dentally in the example of overgrowth of the mandible is that in an attempt for the body to try to maintain dental contacts, the lower incisors tip lingually and the upper incisors tip labially (facially) in an attempt to maintain anterior dental contact relationships as lower jaw growth continues. If the treatment decision is to try to correct the problem with orthodontics alone, Class III elastics would be used along with orthodontic fixed appliances to maintain the lingual tipping and maxillary flaring of incisors. -

TITLE: Photo-Activated Disinfection Therapy for Dental Surgery: Review of the Clinical Effectiveness
TITLE: Photo-Activated Disinfection Therapy for Dental Surgery: Review of the Clinical Effectiveness DATE: 11 September 2013 CONTEXT AND POLICY ISSUES The oral cavity harbors more than 700 prokaryote species;1 most of these species are normal flora of the healthy oral cavity.2 Some of these microorganisms are responsible for oral pathologies. Bacteria such as Actinobacillus actinomycetemcomitans, Prevotella intermedia, Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia are responsible for common forms of periodontal diseases,3 and Bacteroides, Peptostreptococcus, and microaerophilic Streptococcus species may cause osteomyelitis of the jaw.4 During a surgical intervention, disinfection of the oral cavity is attempted by using different chemical solutions such as chlorhexidine and iodine. This is done to prevent, or at least reduce the risk of wound infections or bacteremia following the surgical intervention.5 In the case of periodontal and endodontic treatments, mechanical cleaning of the affected surfaces are believed to be the gold standard.6 Photodynamic antimicrobial chemotherapy or light-activated disinfection is a technology based on the production of free oxygen radicals capable of affecting the membranes of microorganisms.7 The technique is composed of a photosensitizer substance that can be activated with a suitable wave length and light source. The photosensitizer, usually toluidine blue, is activated with a light source. After its activation, it produces energy capable of transforming the surrounding oxygen into free radicals. The free radical then attacks the exposed microorganisms.7 Photodynamic chemotherapy may be used in dentistry to reduce the bacterial load in cases of periodontal lesions and during root canals. Another potential use of this technique is as a pre- surgical disinfection method for the oral cavity to prevent oral flora from penetrating the bone and submucosal tissues during surgery. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

An Overview on Interproximal Enamel Reduction
DENTISTRY ISSN 2377-1623 http://dx.doi.org/10.17140/DOJ-1-104 Open Journal Review An Overview on Interproximal Enamel *Corresponding author Reduction Yanqi Yang Assistant Professor in Orthodontics Faculty of Dentistry, the University of Deborah Chee#, Chong Ren# and Yanqi Yang* Hong Kong, 2/F, Prince Philip Dental Hospital, 34 Hospital Road, Sai Ying #equally contributed Pun, Hong Kong, China Tel. +852-28590252 Orthodontics, Faculty of Dentistry, the University of Hong Kong, 34 Hospital Road, Hong Kong Fax: +852-25593803 SAR, China E-mail: [email protected] Volume 1 : Issue 1 ABSTRACT Article Ref. #: 1000DOJ1104 Ever since its first introduction seven decades ago, there has been continuous advance- ment of the concept and technique of Interproximal enamel reduction (IPR). It’s demonstrated Article History that with correct case selection and clinical performance, IPR is safe and effective for alleviat- Received: October 28th, 2014 ing crowding, improving dental and gingival aesthetics as well as facilitating post-treatment Accepted: December 5th, 2014 stability. The fulfilment of treatment outcomes depends on careful pre-treatment examination Published: December 8th, 2014 and planning, appropriate clinical procedures and effective post-treatment protection. This re- view aims to provide a general introduction to IPR in terms of its history background, risks and Citation benefits and clinical performance. Chee D, Ren C, Yang Y. An overview on interproximal enamel reduction. Dent Open J. 2014; 1(1): 14-18. doi: KEYWORDS: Interproximal enamel reduction; Orthodontic treatment; Crowding; Tooth re- 10.17140/DOJ-1-104 contouring. INTRODUCTION Interproximal enamel reduction (IPR) also described as “stripping”, “reproximation” and “slenderizing” has been applied in clinical orthodontics for almost seven decades.1,2 By removing part of the enamel tissue from the interproximal contact area, this technique has been proved to be effective in improving dental alignment, stability and aesthetics. -

Enhancing the Predictability of Clear Aligners
Enhancing Predictability of Clear Aligners Bowman DRASTIC PLASTIC: ENHANCING THE PREDICTABILITY OF CLEAR ALIGNERS S. Jay Bowman ABSTRACT Once limitations of clear aligner treatments were identified, conceptualizing techniques to improve the predictability in producing desired results was the next logical step. A variety of concepts, methods, and adjuncts have subsequently been introduced to enhance the efficiency and effectiveness of clear aligners. As a consequence, the scope of biomechanics and type of malocclusions that can be more predictably treated has increased. As one example, the inclusion of miniscrew temporary skeletal anchorage has permitted the addition of direct and indirect anchorage to support and control more predictable programmed tooth movements with aligners. After reviewing the reported shortcomings of plastic aligners, this chapter explores possibilities for improving predictability of aligner therapy. KEY WORDS: Clear Aligners, Miniscrews, Bootstrap Elastic, Attachments, Bonded Buttons INTRODUCTION It has been 20 years since the introduction of a commercialized clear aligner product to the orthodontic marketplace. Based on suggestion by Harold D. Kesling over 50 years earlier, Invisalign and later, increasingly numerous propriety alternatives have come to pass; including the exponential growth of so-called direct-to-consumer (DTC or DIY) offerings [1]. From the original questions of whether even “acceptable” results could be obtained from a sequence of aligners, these queries have now evolved into: Is an orthodontist even needed to be interjected between the manufacturer’s plastic and their “customers?” So, the idea of moving teeth with plastic was nothing new, but the use of software to attempt to predict desired tooth movement and the associated 3D representations of individual tooth position were innovative. -
Motion 3D Q&A
THE SAGITTAL FIRST REVOLUTION CARRIERE® MOTION 3D™ Q&A Join the REVOLUTION! #TheHappinessRevolution CLINICAL ADVICE PROVIDED BY: Dr. Carrière received his dental degree from the University of Complutense in Madrid, in 1991. He then attended the University of Barcelona where Dr. Carrière completed his Orthodontic training and received his Master of Science in Orthodontics in 1994. In 2006, he received his Doctorate in Orthodontics, Cum Laude, from the University of Barcelona. Dr. Carrière was the Winner of the prestigious “Joseph E. Johnson Award” and the International Design Award Delta Gold ADI-FAD 2009 for the “Carriere Distalizer MB”. Dr. Carrière is also a Member of the Editorial Review Board for the American Journal of Orthodontics and Dentofacial Orthopedics. As an invited professor of several Orthodontic departments throughout the world, Dr. Carrière lectures internationally when he is not treating patients in his private practice in Barcelona, Spain. Dr. Luis Carrière Dr. Paquette received his dental degree from UNC School of Dentistry in 1979 and a Master’s in Pediatric Dentistry from UNC in 1983. His Master’s thesis won a national research award that same year. He is board certified by the American Board of Pediatric Dentistry. He obtained his Master’s degree and specialty certificate in orthodontics from the St. Louis University in 1990. Dr. Paquette’s Master’s thesis in orthodontics won the coveted Milo Hellman award in 1991. He is an active member of the Schulman Group. Dr. Paquette is passionate about advancing the art and science of orthodontics. He has published numerous articles and lectures nationally and internationally. -

Elastics and Elastomeric in Orthodontics Practice REVIEW ARTICLE
IJPCDR Elastics and Elastomeric in Orthodontics Practice REVIEW ARTICLE Elastics and Elastomeric in Orthodontics Practice 1Sagar Mapare, 2Kanish Bansal, 3Ranjit Pawar, 4Richa Mishra, 5Ashutosh Sthapak, 6Sayed F Khadri ABSTRACT provides the clinician with the ability to correct both Elastics and elastomeric are an important part of orthodontic anteroposterior and vertical discrepancies. treatment with patients’ cooperation; they are used for Both natural rubber and synthetic elastomers are correction of anteroposterior and vertical discrepancies; there widely used in orthodontic therapy. Naturally produced are many types of elastics placement in relation with treatment latex elastics are used in the Begg technique to provide requirements. Elastics can be classified in many ways: intermaxillary traction and intramaxillary forces. Syn- according to the material, their availability, their uses, and force. Elastomer is a general term that encompasses materials that, thetic elastomeric materials in the form of chains find their after substantial deformation, rapidly return to their original greatest application with edgewise mechanics where they dimensions. Natural rubber is the first known elastomeric, are used to move the teeth along the arch wire. used by the ancient Incan and Mayan civilizations. Rubber-like The links of chain fit firmly under the wings of an materials that are made from chemicals were called synthetic edgewise bracket so that chain elastomers also serve to rubber because they were intended as substitutes for natural rubber. replace metal as the ligating force that holds the arch The types of elastic based on their use are class I, II, III, wire to the teeth. Since they are so positively located on palatal, lingual, cross, etc. -

Medically Necessary Orthodontic Treatment – Dental
UnitedHealthcare® Dental Coverage Guideline Medically Necessary Orthodontic Treatment Guideline Number: DCG003.08 Effective Date: November 1, 2020 Instructions for Use Table of Contents Page Related Medical Policy Coverage Rationale ....................................................................... 1 • Orthognathic (Jaw) Surgery Definitions ...................................................................................... 1 Applicable Codes .......................................................................... 3 Description of Services ................................................................. 3 References ..................................................................................... 3 Guideline History/Revision Information ....................................... 4 Instructions for Use ....................................................................... 4 Coverage Rationale Orthodontic treatment is medically necessary when the following criteria have been met: All services must be approved by the plan; and The member is under the age 19 (through age 18, unless the member specific benefit plan document indicates a different age); and Services are related to the treatment of a severe craniofacial deformity that results in a physically Handicapping Malocclusion, including but not limited to the following conditions: o Cleft Lip and/or Cleft Palate; o Crouzon Syndrome/Craniofacial Dysostosis; o Hemifacial Hypertrophy/Congenital Hemifacial Hyperplasia; o Parry-Romberg Syndrome/Progressive Hemifacial Atrophy; -

Research Article
z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 10, Issue, 07, pp.71222-71228, July, 2018 ISSN: 0975-833X RESEARCH ARTICLE THE TONGUE SPEAKS A LOT OF HEALTH. 1,*Dr. Firdous Shaikh, 2Dr. Sonia Sodhi, 3Dr Zeenat Fatema Farooqui and 4Dr. Lata Kale 1PG Student, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 2Professor, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 3Fatema Farooqui, Chief Medical Officer, Sri Ram Homeopathic Clinic and Research Center, Solapur 4Professor and Head, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad ARTICLE INFO ABSTRACT Article History: Multifunctional organ of the human body without a bone yet strong is the tongue. It mainly consists Received 26th April, 2018 of the functional portion of muscle mass, mucosa, fat and the specialized tissue of taste i.e. the Received in revised form papillae. Diseases may either result from internal/ systemic causes of extrinsic causes like trauma, 14th May, 2018 infection, etc. A new method for classification has been proposed in this review for diseases of Accepted 09th June, 2018 tongue. This review mainly focuses on encompassing almost each aspect that the body reflects via its th Published online 30 July, 2018 mirror in mouth, the tongue. Key Words: Tongue, Diseases of Tongue, Discoloration of Tongue, Oral health, Hairy Tongue. Copyright © 2018, Firdous Shaikh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

Therapeutic Management of Patients with Class III Skeletal Malocclusion
Szpyt Justyna, Gębska Magdalena. Therapeutic management of patients with class III skeletal malocclusion. Mandibular prognathism, maxillary retrognathism – a case report. Journal of Education, Health and Sport. 2019;9(5):20-31. eISSN 2391-8306. DOI http://dx.doi.org/10.5281/zenodo.2656446 http://ojs.ukw.edu.pl/index.php/johs/article/view/6872 https://pbn.nauka.gov.pl/sedno-webapp/works/912455 The journal has had 7 points in Ministry of Science and Higher Education parametric evaluation. Part B item 1223 (26/01/2017). 1223 Journal of Education, Health and Sport eISSN 2391-8306 7 © The Authors 2019; This article is published with open access at Licensee Open Journal Systems of Kazimierz Wielki University in Bydgoszcz, Poland Open Access. This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author (s) and source are credited. This is an open access article licensed under the terms of the Creative Commons Attribution Non commercial license Share alike. (http://creativecommons.org/licenses/by-nc-sa/4.0/) which permits unrestricted, non commercial use, distribution and reproduction in any medium, provided the work is properly cited. The authors declare that there is no conflict of interests regarding the publication of this paper. Received: 15.04.2019. Revised: 25.04.2019. Accepted: 01.05.2019. Therapeutic management of patients with class III skeletal malocclusion. Mandibular prognathism, maxillary retrognathism – a case report Justyna Szpyt1, Magdalena Gębska2 1. Physiotherapy student, Faculty of Health Sciences, Pomeranian Medical University in Szczecin.