Stability of Anterior Open Bite Treatment with Molar Intrusion Using Skeletal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

International Magazine of Orthodontics 22017
orthoissn 1868-3207 Vol. 2 • Issue 2/2017 international magazine of orthodontics 22017 technique Tongue star 2 (TS2) – System for rapid open bite closure case report Use of diode laser in the treatment of gingival enlargement during orthodontic treatment industry report Sensorimotor training with RehaBite during orthodontic treatment 4th ORTHOCAPS® SYMPOSIUM 1 & 2 DECEMBER 2017 MUNICH, GERMANY Hotel Vier Jahreszeiten Kempinski, Munich Attendance fee: 299€ (includes 19% VAT) Registration fee includes: - Lunch and coffee breaks - Get together on Friday Course Language: English, simultaneous French translation available GUEST SPEAKERS BOLDT, Florian - Germany FARINA, Achille - Italy FERNANDEZ, Enrique - Spain Symbiosis and Uses of 3D Six Keys to Successful My Experience with Techniques in Daily Practice Treatments with Orthocaps® Orthocaps® KALIA, Sonil - United Kingdom ROLLET, Daniel - France SOREL, Olivier - France WILMES, Benedict - Germany Bio-mechanical Principles with Functional Occlusion Smile Design & Stripping Expanding the Horizons of Orthocaps® and Aligners, Why Orthocaps®? Essentials Aligner Therapy with TADs Ortho Caps GmbH, An der Bewer 8, Hamm 59069 Tel: +49 (0) 2385 92190 Fax: +49 (0) 2385 9219080 Email: [email protected] www.orthocaps.de editorial Dear readers, When I began working in the field of orthodontics (in the Middle Ages!), it was very differ- ent from what I encounter today in my daily practice. This is normal: with the progression of research on biology, biomechanics and biomaterials, as well as with the development of the technology, results have increasingly been improving, as have treatment times, aesthe tics and patient comfort. There is another important aspect too that has completely changed our way of working: Prof. -
Important Message
WE INTERRUPT YOUR REGULARLY SCHEDULED PROGRAM FOR AN IMPORTANT MESSAGE Q1 2018 inside this Disrupted: edition... New Rules for a New Type of Customer By Angela Weber, CMO OrthoSynetics Page 34 BUSINESS PRACTICE & DEVELOPMENT TRAVEL & LEISURE CLINICAL CORNER 18 15 37 From the Rear View Mirror Pro Travel Tips High Frequency Vibration Can BY DR. COURTNEY DUNN BY PROORTHO STAFF Reduce or Eliminate Pain During Aligner Treatment 30 20 BY DR. JONATHAN L. NICOZISIS Traveling to the Greek Islands New Gaidge CEO BY DR. DANIELA LOEBL INTERVIEW WITH RYAN MOYNIHAN 32 OFFICE LOGISTICS 34 Traveling to Peru Disrupted: New Rules for a New BY DR. DAVID WALKER 56 Type of Customer Beyond Reminders: BY ANGELA WEBER, CMO ORTHOSYNETICS 40 Tapping the Potential of Texting Traveling to Spain BY DR. KEITH DRESSLER 44 BY DR. DAVID MAJERONI What Would You Do If an Aligner 46 Store Opened Down the Street? ORTHOPUNDIT.COM BY DR. JENNIFER EISENHUTH Traveling to Europe BY DR. BEN BURRIS & BRIDGET BURRIS 09 MARKETING/ H.R. INSIGHT Don't Piss Momma Off! SOCIAL MEDIA BY DR. BEN BURRIS 05 28 24 Go High or Go Low - Just Don't Get Utilize Group Interviews To Made to Measure: Stuck in the Middle Maximize Hiring Success The Dubious Relationship Between BY DR. LEON KLEMPNER AND AMY EPSTEIN, BY BRIDGET BURRIS Eugenics and Orthodontics MBA ANSWERS FROM THE BY DR. MARC ACKERMAN 52 EDGE 59 5 Keys to Capturing the Fastest The Economy Is Booming – Why Growing Referral Source 10 Isn’t Your Practice? BY NICK DUNCAN Interviews with Dr. Jeff Kozlowski BY DR. -

Distalization of the Mandibular Dentition with Mini-Implants to Correct a Class III Malocclusion with a Midline Deviation
CASE REPORT Distalization of the mandibular dentition with mini-implants to correct a Class III malocclusion with a midline deviation Kyu-Rhim Chung,a Seong-Hun Kim,b HyeRan Choo,c Yoon-Ah Kook,d and Jason B. Copee Uijongbu and Seoul, Korea, Philadelphia, Pa, and Dallas, Tex This article describes the orthodontic treatment for a young woman, aged 23 years 5 months, with a Class III malocclusion and a deviated midline. Two orthodontic mini-implants (C-implants, CIMPLANT Company, Seoul, Korea) were placed in the interdental spaces between the mandibular second premolars and first mo- lars. The treatment plan consisted of distalizing the mandibular dentition asymmetrically and creating space for en-masse retraction of the mandibular anterior teeth. C-implants were placed to provide anchorage for Class I intra-arch elastics. The head design of the C-implant minimizes gingival irritation during orthodontic treatment. Sliding jigs were applied buccally for distalization of the mandibular posterior teeth. The active treatment period was 18 months. Normal overbite and overjet were obtained, and facial balance was improved. (Am J Orthod Dentofacial Orthop 2010;137:135-46) very orthodontic tooth movement is accompa- patients. Therefore, several authors have attempted to nied by a reaction. This can make it difficult to treat this type of malocclusion by distal tooth movement Ecorrect a malocclusion by using intraoral appli- alone. For example, animal studies and clinical investi- ances alone, especially when complete distal movement gations have used conventional implants as absolute of the mandibular dentition is planned in nonsurgical anchorage2-4 and miniplates for intrusion or distalization Class III malocclusion treatment. -
Tongue - Cause and Correction of Anterior Open Bite Malocclusion
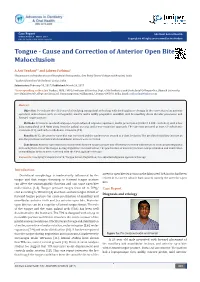
Case Report Adv Dent & Oral Health Volume 4 Issue 3 - March 2017 DOI: 10.19080/ADOH.2016.04.555636 Copyright © All rights are reserved by Arif Yezdani Tongue - Cause and Correction of Anterior Open Bite Malocclusion A Arif Yezdani*1 and Jabeen Fathima2 1Department of Orthodontics and Dentofacial Orthopaedics, Sree Balaji Dental College and Hospital, India 2 Yezdani Dental and Orthodontic Center, India Submission: February 10, 2017; Published: March 24, 2017 *Corresponding author:Arif Yezdani, MDS, FWFO, Professor & Director, Dept. of Orthodontics and Dentofacial Orthopaedics, Bharath University, Sree Balaji Dental College and Hospital, Narayanapuram, Pallikaranai, Chennai-600100, India, Email: Abstract Objective: open bite malocclusion with an orthognathic maxilla and a mildly prognathic mandible with bi-maxillary dento-alveolar protrusion and forward tongue Toposture. evaluate the efficiency of a low lying transpalatal arch along with fixed appliance therapy in the correction of an anterior Methods: Treatment involved strap-up of a pre-adjusted edgewise appliance, Roth’s prescription (0.022 X 0.028 - inch slot), with a low lying transpalatal arch 4mm away from the palatal mucosa, and a non-extraction approach. The case was assessed at start of orthodontic treatment (T1), and end of orthodontic treatment (T2). Results: At T2, the anterior open bite was corrected and the canines were treated to a class I relation. The proclined maxillary incisors as also the proclined and imbricated mandibular incisors were corrected. Conclusion: Anterior open bite malocclusion with forward tongue posture was effectively corrected with the use of a low lying transpalatal arch using the forces of the tongue during deglutition and mastication. -

Upper Anterior Intrusion with Mini-Implants to Correct Anterior Deep Bite in a Periodontally Compromised Class II Malocclusion
www.medigraphic.org.mx Revista Mexicana de Ortodoncia Vol. 2, No. 2 April-June 2014 pp 105-111 CASE REPORT Upper anterior intrusion with mini-implants to correct anterior deep bite in a periodontally compromised class II malocclusion. Case report Intrusión del segmento anterior superior con miniimplantes para eliminar la mordida profunda anterior en maloclusión clase II con compromiso periodontal. Reporte de un caso Carlos Eder Zamudio López,* Silvia Tavira Fernández§ ABSTRACT RESUMEN The use of mini-implants has revolutioned biomechanics in or- El uso de miniimplantes ha revolucionado la biomecánica de thodontics with better results as far as anchorage is concerned. We la ortodoncia con mejores resultados en cuanto al anclaje se have no limits when using these attachments depending only on refi ere. No hay límites al momento de utilizar estos aditamentos, our imagination. Anterior deep bites in severe class II malocclusion y depende únicamente de nuestra imaginación. Las mordidas patients are a common problem that causes orthodontists to focus profundas en la región anterior son un problema frecuente en therapy in biomechanics to eliminate the problem by extrusion of los pacientes con clase II severa, lo que nos obliga a enfocar posterior teeth or intrusion of the anterior. In this case, we decided nuestra terapéutica en una mecánica a corregir el problema to correct the anterior deep bite by intruding the incisors using as mediante la extrusión de los dientes posteriores, o bien, mediante anchorage two mini-implants. The case was compromised by perio- la intrusión de los dientes anteriores. En este caso, decidimos dontal disease with moderated loss of alveolar bone so we had to corregir la mordida profunda anterior mediante la intrusión de los choose biomechanics with a stable anchorage to achieve our goals. -

Treatment of Anterior Open Bite with the Bimler Functional Appliance
tist Den ry Dentistry Yañez et al., Dentistry 2014, 4:8 ISSN: 2161-1122 DOI: 10.4172/2161-1122.1000250 Case Report Open Access Treatment of Anterior Open Bite with the Bimler Functional Appliance: Report of Three Cases Ramirez-Yañez GO1*, Mahony D2 and Bimler B3 1Faculty of Dentistry, University of Manitoba, Winnipeg, Canada 2Private Practice, Sydney, Australia 3International Stomatopedic Institute, Wiesbaden, Germany *Corresponding author: German Ramirez-Yañez, Faculty of Dentistry, University of Manitoba, Winnipeg, Manitoba R3E 0W2, Canada, Tel: 1 289 430 5287; E-mail: [email protected] Rec date: Jun 25, 2014, Acc date: Jul 25, 2014, Pub date: Jul 27, 2014 Copyright: © 2014 Ramirez-Yañez GO, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited Abstract There is still controversy regarding the efficacy of functional appliances when treating malocclusion at an early age. Although a good outcome from treatment is important, the stability of the results over time becomes a major concern. This paper presents the results of three open bite cases treated with the Bimler type-A appliance in the mixed dentition. The open bite cases presented here demonstrate stability of the treatment results for more than 14 years without active retention after the active treatment period. A comparison between these cases and those performed with an elastic functional appliance, and the action of that appliance on tongue posture, are discussed. The cases presented in this paper support treating malocclusions at an early age with functional appliances. -

Correction of Dentofacial Deformities with Orthognathic Surgery. Outcome
CORRECTION OF KARI DENTOFACIAL DEFORMITIES PANULA WITH ORTHOGNATHIC Department of Oral and Maxillofacial Surgery, SURGERY Institute of Dentistry, Outcome of treatment with special reference to University of Oulu costs, benefits and risks OULU 2003 KARI PANULA CORRECTION OF DENTOFACIAL DEFORMITIES WITH ORTHOGNATHIC SURGERY Outcome of treatment with special reference to costs, benefits and risks Academic Dissertation to be presented with the assent of the Faculty of Medicine, University of Oulu, for public discussion in the Auditorium 1 of the Institute of Dentistry, on May 9th, 2003, at 12 noon. OULUN YLIOPISTO, OULU 2003 Copyright © 2003 University of Oulu, 2003 Reviewed by Docent Knut Tornes Docent Pekka Ylipaavalniemi ISBN 951-42-6993-4 (URL: http://herkules.oulu.fi/isbn9514269934/) ALSO AVAILABLE IN PRINTED FORMAT Acta Univ. Oul. D 718, 2003 ISBN 951-42-6992-6 ISSN 0355-3221 (URL: http://herkules.oulu.fi/issn03553221/) OULU UNIVERSITY PRESS OULU 2003 Panula, Kari, Correction of dentofacial deformities with orthognathic surgery. Outcome of treatment with special reference to costs, benefits and risks Department of Oral and Maxillofacial Surgery, Institute of Dentistry, University of Oulu, P.O.Box 5281, FIN-90014 University of Oulu, Finland Oulu, Finland 2003 Abstract Considerable amounts of research have been done on various aspects of orthognathic surgery during its short history. Nevertheless, there are no comprehensive publications on the cost-risk-benefit analysis of the entire process of orthognathic surgery. The purpose of the present study was to evaluate the psychosocial and biophysiological outcomes of orthognathic surgery with special reference to complications and financial costs. The study series consisted of patients referred for consultations and treatment of dentofacial deformities and involved a total of 953 patients and 20 controls. -

ORTHODONTIC PERSPECTIVES on OROFACIAL MYOFUNCTIONAL THERAPY Robert M
49 from: International Journal of Orofacial Myology, S pedal Issue "Orofacial Myology: CUrrent Trends", volume 14, #1, March, 1988. ORTHODONTIC PERSPECTIVES ON OROFACIAL MYOFUNCTIONAL THERAPY Robert M. Mason, Ph.D., D.M.D. Professor and Chief of Orthodontics Division of Plastic, Reconstructive,Maxillofacial and Oral Surgery Department of Surgery, Duke University Medical Center, Durham, North Carolina Uke most other specialty areas, orthodontics has a rich behavior in an intertwined environment of anatomical and professional literature containing disagreement and physiological relationships. That is, a tongue thrust debate on a number of topics. One area of controversy swallow or a lips-apart resting position, for example, may since the inception of orthodontics in the late 1800s is occur for a single reason or combination of reasons. The the relationship between tongue functions and the challenge for the clinician is to identify the various fac- development of malocclusions. tors that combine to produce the observation identified Many orthodontists continue to believe strongly that as a variation. tongue functions cause certain types of malocclusions Tongue thrusting during swallowing may be a and lead to altered patterns of facial development. Others necessary adaptation to maintain the size of the airway implicate the tongue as the cause of negative tooth posi- for successful passage of food to the esophagus. A small tion changes (or "relapse") sometimes seen following the oral isthmus due to enlarged faucial tonsils may obligate completion of orthodontic treatment. On the other hand, the tongue to move forward as the bolus of food exits many orthodontists express no concern that tongue func- the oral cavity during the process of swallowing.The tions contribute importantly to the problems seen in their squirting forward of the tongue during such an adapta- clinical practices. -

Angle Class I Malocclusion, with Anterior Open Bite, Treated with Extraction of Permanent Teeth*
C ASO C LÍNI C O B B O Má oclusão Classe I de Angle, com mordida aberta anterior, tratada com extração de dentes permanentes* Mírian Aiko Nakane Matsumoto** Resumo A mordida aberta é uma anomalia com características distintas que, além da complexi- dade dos múltiplos fatores etiológicos, traz consequências estéticas e funcionais. Muitas alternativas têm sido utilizadas em seu tratamento, entre elas a grade palatina, forças ortopédicas, ajuste oclusal, camuflagem com ou sem exodontias, mini-implantes ou mi- niplacas e cirurgia ortognática. O diagnóstico preciso e a determinação da etiologia permitem estabelecer os objetivos e o plano de tratamento ideal para essa má oclusão. O presente relato descreve o tratamento de uma má oclusão Classe I de Angle, com padrão esquelético de Classe II e mordida aberta anterior, realizado em duas fases e que foi apresentado à diretoria do Board Brasileiro de Ortodontia e Ortopedia Facial (BBO), representando a categoria 2, como parte dos requisitos para a obtenção do título de Diplomado pelo BBO. Palavras-chave: Má oclusão de Classe I de Angle. Mordida aberta. Ortodontia corretiva. Extração dentária. INTRODUÇÃO estado de saúde geral, sem relato de doenças gra- Paciente do sexo feminino, leucoderma, 12 ves ou traumas. anos de idade, foi encaminhada pela fonoaudió- loga para tratamento ortodôntico e apresentou- DIAGNÓSTICO se com queixa principal de “falta de contato en- Ao exame clínico, evidenciava-se o terço infe- tre os dentes anteriores e posição alterada dos ca- rior da face aumentado, a deficiência de selamento ninos superiores”. Na anamnese, relatou ter sido labial, perfil levemente convexo, ângulo nasolabial portadora de hábito de sucção de chupeta até os obtuso e boa linha cérvico-mandibular (Fig. -
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations
Treatment of Class II, Division 2 Malocclusion in Adults: Biomechanical Considerations FLAVIO URIBE, DDS, MDS RAVINDRA NANDA, BDS, MDS, PHD reatment of Class II malocclusion in adoles- inclined upper central and lower incisors, and Tcents has always relied on growth modifica- labially flared maxillary lateral incisors. These tion. The majority of treatment modalities, such patients also tend to exhibit problems with the as functional appliances, are directed at stopping upper and lower occlusal planes, such as deep or redirecting maxillary growth and simultane- curves of Spee. The soft-tissue drape of the lips ously stimulating mandibular growth.1-3 On the often conforms to the malocclusion, so that the other hand, in adult patients with severe Class II lips may be redundant with a deep mentolabial malocclusions, generally involving extremely sulcus. Because of the deep bite and supraerup- deficient mandibles, orthognathic surgery is tion of the maxillary incisors, the gingival mar- often the only possible treatment. gins of the maxillary anterior teeth are usually Although camouflage may be attempted by malaligned, and the lingually inclined mandibu- extracting premolars, the soft-tissue objectives lar incisors may have excessively high gingival may be impossible to meet. Even so, a recent margins (Fig. 1). study has shown that patient satisfaction with camouflage treatment was similar to that achieved with surgical mandibular advance- ment.4 In Class II patients with mild-to-moderate skeletal discrepancies, dental compensation may well be the treatment of choice. Common treat- ment procedures for such patients include flaring of incisors, interproximal tooth reduction, and extractions. Treatment of an adult Class II patient requires careful diagnosis and a treatment plan involving esthetic, occlusal, and functional con- siderations.5-7 The treatment objectives must include the chief complaint of the patient, and A the mechanics plan should be individualized based on the specific treatment goals. -

Invisalign Treatment Planning Guide 1 Align Technology, Inc
Table of Contents INTRODUCTION . 2 Getting Quality Clinical Outcomes with Invisalign. 2 Invisalign Applicability . 3 DIAGNOSIS AND TREATMENT OPTIONS 1. Crowding . 4 2. Spacing. 10 3. Narrow Arches . 16 4. Crossbite. 20 5. Deep Bite . 24 6. Open Bite . 28 7. Class II . 32 Invisalign 8. Class III . 38 CLINICAL NOTES Treatment IPR . 5 Tooth Size Discrepancy . 11 Planning Staging . 12 Auxiliary Treatment. 12 Guide Expansion . 17 Attachments. 25 Anchorage . 42 APPENDIX Prescription Form Tips. 44 Glossary . 46 Index. 48 Credits . 54 Invisalign Treatment Planning Guide 1 Align Technology, Inc. Introduction HOW TO USE THIS GUIDE Getting Quality Clinical The guide is organized by patient diagnosis. ABOUT THIS GUIDE Match your patient’s diagnosis to the appropriate Outcomes with Invisalign The goal of this guide is to provide you with a diagnosis decision tree to see some possible treat- decision making tool you can use while selecting ment options. Read the accompanying treatment Successful clinical outcomes with Invisalign and treatment planning your Invisalign cases. notes and evaluate your options given your start with attention to detail during case By outlining typically used Invisalign approaches Invisalign experience level. See Figure A, below. selection and treatment planning. Here are and discussing their complexity and predict- five guidelines for setting up your cases that ABOUT THIS SERIES ability, we hope to make the treatment planning pay great dividends later: This guide is the first in a three-part series options and implications more clear for you of Invisalign patient care references, comple- to evaluate. 1. Submit high quality records. Accurate menting the ClinCheck® Evaluation Guide PVS impressions and clear patient photos and (D4458) and the Invisalign Clinical Monitoring Align Technology is not a provider of medical, radiographs are critical for the creation of your Guide (D4219). -

Director's Remarks
The British Orthodontic Society Clinical Effectiveness Bulletin No.33 November 2014 Clinical Governance Directorate of the British Orthodontic Society Director’s Remarks Moving House! lthough this is the autumn edition of the 1st Prize Clinical Effectiveness Bulletin, I think there An audit of compliance in Orthodontics with has been something of a spring clean within Department of Health 2007 “Smokefree and A Smiling” guidance. the editorial ranks. This edition has been jointly produced by Kate House, the outgoing editor, and A.McMullin and S. Caldwell (University Dental Jadbinder Seehra, our new incoming editor. The Hospital Manchester). team have worked hard to produce an excellent Bulletin with an interesting range of articles. There 2nd Prize are some familiar themes again, patient satisfaction Use of the PAR index to assess outcomes of and multidisciplinary care, but some more varied orthognathic surgery in cleft lip and palate patients. projects looking at the periodontal health of our C. Rolland (VT dentist), C. Chambers (Bristol patients and their dietary habits, reflecting the wider Dental Hospital) and S. Deacon (Frenchay Hospital scope of our practice. and Bristol Dental Hospital). Knowing that audit is strong within our specialty, 3rd Prize I was interested to read that the Healthcare Quality Orthodontic treatment and orthognathic surgery – Improvement Partnership (HQIP), the organisation do we predict the length of treatment accurately? tasked with promoting quality in healthcare, in C. Dunbar, G. McIntyre (Dundee Dental Hospital) particular increasing the impact that clinical audit and S. Laverick (Ninewells Hospital, Dundee). has on healthcare quality in England and Wales, recently promoted its second ‘Audit Awareness Many congratulations to all the winning authors.