Medical Product Quality Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chemical Disinfectants for Biohazardous Materials (3/21)
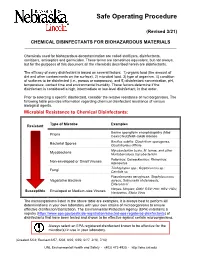
Safe Operating Procedure (Revised 3/21) CHEMICAL DISINFECTANTS FOR BIOHAZARDOUS MATERIALS ____________________________________________________________________________ Chemicals used for biohazardous decontamination are called sterilizers, disinfectants, sanitizers, antiseptics and germicides. These terms are sometimes equivalent, but not always, but for the purposes of this document all the chemicals described herein are disinfectants. The efficacy of every disinfectant is based on several factors: 1) organic load (the amount of dirt and other contaminants on the surface), 2) microbial load, 3) type of organism, 4) condition of surfaces to be disinfected (i.e., porous or nonporous), and 5) disinfectant concentration, pH, temperature, contact time and environmental humidity. These factors determine if the disinfectant is considered a high, intermediate or low-level disinfectant, in that order. Prior to selecting a specific disinfectant, consider the relative resistance of microorganisms. The following table provides information regarding chemical disinfectant resistance of various biological agents. Microbial Resistance to Chemical Disinfectants: Type of Microbe Examples Resistant Bovine spongiform encephalopathy (Mad Prions Cow) Creutzfeldt-Jakob disease Bacillus subtilis; Clostridium sporogenes, Bacterial Spores Clostridioides difficile Mycobacterium bovis, M. terrae, and other Mycobacteria Nontuberculous mycobacterium Poliovirus; Coxsackievirus; Rhinovirus; Non-enveloped or Small Viruses Adenovirus Trichophyton spp.; Cryptococcus sp.; -

Stanford Chem-H Presentation (PDF)
KiNativ® In situ kinase profiling Stanford University ChEM-H confidential @KiNativPlatform Principle of the KiNativ platform • ATP (or ADP) acyl phosphate binds to, and covalently modifies Lysine residues in the active site • Thus, ATP acyl phosphate with a desthiobiotin tag can be used capture and quantitate kinases in a complex lysate Acyl phosphate Desthiobiotin tag ATP 2 ATP acyl phosphate probe covalently modifies kinase in the active site Lysine 2 Lysine 1 3 ATP acyl phosphate probe covalently modifies kinase in the active site Lysine 2 Lysine 1 4 Samples trypsinized, probe-labeled peptides captured with streptavidin, and analyzed by targeted LC-MS2 Identification Quantitation Explicit determination of peptide Integration of signal from MS2 sequence and probe modification site fragment ions from MS2 spectrum 5 Comprehensive Coverage of Protein and Lipid Kinases Protein kinases Atypical kinases Green: Kinases detected on KiNativ Red: Kinases not detected on KiNativ ~80% of known protein and atypical kinases identified on the platform http://www.kinativ.com/coverage/protein-lipid.html 6 Profiling compound(s) on the KiNativ platform Control sample – add probe Sample: Lysate derived from any cell line or tissue from ANY species Treated sample – add inhibitor followed by probe Inhibited kinase Green: Kinases Blue: Probe Gray: Non-kinases Red: Inhibitor 7 Profiling compound(s) on the KiNativ platform Control sample – add probe MS signalMS Sample: Lysate derived from any cell line or tissue from ANY species Treated sample – add inhibitor -

Presentation
Strategies to support the COVID-19 response in LMICs A virtual seminar series Therapeutics Landscape for COVID-19 Natasha Mubeen Chida, MD MSPH Associate Program Director, Infectious Disease Fellowship Program Assistant Professor, Division of Infectious Diseases Johns Hopkins University School of Medicine Objectives • Review biological plausibility of Remdesivir for SARS-CoV-2 treatment • Review clinical data on Remdesivir • Review biological plausibility of Hydroxychloroquine for SARS-CoV-2 treatment • Review clinical data on Hydroxychloroquine • Discuss cytokine release syndrome in COVID-19 • Discuss use of anti IL-6 blockade for management of CRS • State ongoing clinical trials for Remdesivir, hydroxychloroquine, IL-6 blockade Sample of COVID-19 Therapeutic Landscape Antivirals Immune Modulators Other Baloxavir Anakinra ACEI/ARB Chloroquine/Hydroxychloroquine Convalescent Plasma Ascorbic Acid DAS-181 Corticosteroids Azithromycin Favipiravir IVIG Epoprostenol Interferon Lenzilumab Indomethacin Lopinavir/Ritonavir Ruxolitinib Ivermectin Neuraminidase inhibitors Sarilumab Niclosamide Remdesivir Sirolimus Nitazoxanide Ribavarin Tocilizumab Statins Umifenovir Acalabrutinib SARS-CoV-2 Liu C, et al. ACS Cent Sci. doi: 10.1021/acscentsci.0c00272 (2020). Jiang S, Hillyer C, Du L. Trends Immunol doi: 10.1016/j.it.2020.03.007 (2020). “Antivirals” Remdesivir • 2013 Ebola outbreak • CDC/USAMRIDD/Gilead Sciences identified nucleoside lead à prodrug, RDV • Metabolized to active form, adenosine nucleoside analog • Interferes with RNA polymerase • Evades -
Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination
Assessment of iodine deficiency disorders and monitoring their elimination A GUIDE FOR PROGRAMME MANAGERS Third edition Assessment of iodine deficiency disorders and monitoring their elimination A GUIDE FOR PROGRAMME MANAGERS Third edition WHO Library Cataloguing-in-Publication Data Assessment of iodine deficiency disorders and monitoring their elimination : a guide for programme managers. – 3rd ed. 1.Iodine – deficiency. 2.Nutrition disorders – prevention and control. 3.Sodium chloride, Dietary – therapeutic use. 4.Nutrition assessment. 5.Nutrition policy – standards. 6.Guidelines. I.World Health Organization. ISBN 978 92 4 159582 7 (NLM classification: WK 250) This report contains the collective views of an international group of experts, and does not necessarily represent the decisions or the stated policy of the World Health Organization. © World Health Organization 2007 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncom- mercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organi- zation concerning the legal status of any country, territory, city or area or of its authori- ties, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. -

Decontamination of Rooms, Medical Equipment and Ambulances Using an Aerosol of Hydrogen Peroxide Disinfectant B.M
Journal of Hospital Infection (2006) 62, 149–155 www.elsevierhealth.com/journals/jhin Decontamination of rooms, medical equipment and ambulances using an aerosol of hydrogen peroxide disinfectant B.M. Andersena,*, M. Rascha, K. Hochlina, F.-H. Jensenb, P. Wismarc, J.-E. Fredriksend aDepartment of Hospital Infection, Ulleva˚l University Hospital, Oslo, Norway bDivision of Pre-hospital Care, Ulleva˚l University Hospital, Oslo, Norway cDepartment of Medical Equipment, Ulleva˚l University Hospital, Oslo, Norway dHealth and Environment AS, Oslo, Norway Received 17 November 2004; accepted 1 July 2005 KEYWORDS Summary A programmable device (Sterinis, Gloster Sante Europe) Room decontamina- providing a dry fume of 5% hydrogen peroxide (H2O2) disinfectant was tion; Ambulance tested for decontamination of rooms, ambulances and different types of decontamination; medical equipment. Pre-set concentrations were used according to the Medical equipment decontamination; volumes of the rooms and garages. Three cycles were performed with Hydrogen peroxide increasing contact times. Repetitive experiments were performed using fume decontamina- Bacillus atrophaeus (formerly Bacillus subtilis) Raven 1162282 spores to tion; Spore test control the effect of decontamination; after a sampling plan, spore strips were placed in various positions in rooms, ambulances, and inside and outside the items of medical equipment. Decontamination was effective in 87% of 146 spore tests in closed test rooms and in 100% of 48 tests in a surgical department when using three cycles. One or two cycles had no effect. The sporicidal effect on internal parts of the medical equipment was only 62.3% (220 tests). When the devices were run and ventilated during decontamination, 100% (57/57) of spore strips placed inside were decontaminated. -

Predictive QSAR Tools to Aid in Early Process Development of Monoclonal Antibodies
Predictive QSAR tools to aid in early process development of monoclonal antibodies John Micael Andreas Karlberg Published work submitted to Newcastle University for the degree of Doctor of Philosophy in the School of Engineering November 2019 Abstract Monoclonal antibodies (mAbs) have become one of the fastest growing markets for diagnostic and therapeutic treatments over the last 30 years with a global sales revenue around $89 billion reported in 2017. A popular framework widely used in pharmaceutical industries for designing manufacturing processes for mAbs is Quality by Design (QbD) due to providing a structured and systematic approach in investigation and screening process parameters that might influence the product quality. However, due to the large number of product quality attributes (CQAs) and process parameters that exist in an mAb process platform, extensive investigation is needed to characterise their impact on the product quality which makes the process development costly and time consuming. There is thus an urgent need for methods and tools that can be used for early risk-based selection of critical product properties and process factors to reduce the number of potential factors that have to be investigated, thereby aiding in speeding up the process development and reduce costs. In this study, a framework for predictive model development based on Quantitative Structure- Activity Relationship (QSAR) modelling was developed to link structural features and properties of mAbs to Hydrophobic Interaction Chromatography (HIC) retention times and expressed mAb yield from HEK cells. Model development was based on a structured approach for incremental model refinement and evaluation that aided in increasing model performance until becoming acceptable in accordance to the OECD guidelines for QSAR models. -
Evaluating Disinfectants for Use Against the COVID-19 Virus
When it comes to choosing a disinfectant to combat the COVID-19 virus, research and health authorities suggest not all disinfectants are equally effective. The difference is in their active ingredient(s). HEALTH CANADA AND U.S. EPA ASSESSMENTS The work to evaluate disinfectants perhaps best starts with lists of approved disinfectants compiled by government health authorities. Health Canada has compiled a list of 85 hard surface disinfectant products (as of March 20, 2020) that meet their requirements for disinfection of emerging pathogens, including the virus that causes COVID-19. It can be accessed here. You can wade through the entire list. But if you locate the Drug Identification Number (DIN) on the disinfectant product label or the safety data sheet (SDS), then you can use the search function to quickly see if the product meets Health Canada requirements. A second list, updated on March 19, 2020, provides 287 products that meet the U.S. Environmental Protection Agency’s (EPA) criteria for use against SARS-CoV-2, the novel coronavirus that causes the disease COVID-19. This list can be found here. Like the Health Canada list, you can wade through this one too. However, to best use this list, you should locate the U.S. EPA registration number on the product label or SDS, and use that number to search the list. The U.S. EPA registration number of a product consists of two sets of numbers separated by a hyphen. The first set of numbers refers to the company identification number, and the second set of numbers following the hyphen represents the product number. -

Download Product Insert (PDF)
PRODUCT INFORMATION Pacritinib Item No. 16709 CAS Registry No.: 937272-79-2 Formal Name: 11-[2-(1-pyrrolidinyl)ethoxy]-14,19-dioxa- 5,7,27-triazatetracyclo[19.3.1.12,6.18,12] O heptacosa-1(25),2,4,6(27),8,10,12(26), 16E,21,23-decaene Synonym: SB1518 N N H MF: C28H32N4O3 FW: 472.6 N Purity: ≥98% O Stability: ≥2 years at -20°C Supplied as: A crystalline solid N O UV/Vis.: λmax: 285 nm Laboratory Procedures For long term storage, we suggest that pacritinib be stored as supplied at -20°C. It should be stable for at least two years. Pacritinib is supplied as a crystalline solid. A stock solution may be made by dissolving the pacritinib in the solvent of choice. Pacritinib is soluble in the organic solvent DMSO, which should be purged with an inert gas, at a concentration of approximately 0.5 mg/ml (slightly warmed). Pacritinib is sparingly soluble in aqueous solutions. To enhance aqueous solubility, dilute the organic solvent solution into aqueous buffers or isotonic saline. If performing biological experiments, ensure the residual amount of organic solvent is insignificant, since organic solvents may have physiological effects at low concentrations. We do not recommend storing the aqueous solution for more than one day. Description FMS-like tyrosine kinase 3 (FLT3) and Janus kinase 2 (JAK2) are tyrosine kinases that mediate cytokine signaling and are frequently mutated in cancers, particularly acute myeloid leukemia.1,2 Pacritinib is an 1 inhibitor of both FLT3 and JAK2 (IC50s = 22 and 23 nM, respectively). -

Comparative Safety and Efficacy of Anti-PD-1 Monotherapy, Chemotherapy
Lv et al. Journal for ImmunoTherapy of Cancer (2019) 7:159 https://doi.org/10.1186/s40425-019-0636-7 COMMENTARY Open Access Comparative safety and efficacy of anti-PD- 1 monotherapy, chemotherapy alone, and their combination therapy in advanced nasopharyngeal carcinoma: findings from recent advances in landmark trials Jia-Wei Lv1†, Jun-Yan Li1†, Lin-Na Luo2†, Zi-Xian Wang2* and Yu-Pei Chen1* Abstract Recent phase 1–2 trials reported manageable safety profiles and promising antitumor activities of anti-PD-1 drugs (pembrolizumab, nivolumab, camrelizumab and JS001) with/without chemotherapy in recurrent/metastatic nasopharyngeal carcinoma (RM-NPC), however head-to-head comparison among these regimens is lacking. We aimed to comprehensively compare the efficacy and safety of different anti-PD-1 drugs, standard chemotherapy, and their combination therapy in RM-NPC. Adverse event (AE) and objective response rate (ORR) were assessed. The pooled incidence rates of grade 1–5/3–5 AEs were 74.1%/29.6, 54.2%/17.4, 92.3%/24.5, 96.8%/16.1, 91.2%/42.8, and 100%/87.9% for pembrolizumab, nivolumab, JS001, camrelizumab, chemotherapy and camrelizumab+chemotherapy, respectively, which suggested that nivolumab and pembrolizumab exhibited the optimal safety regarding grade 1–5 AEs whereas camrelizumab and nivolumab regarding grade 3–5 AEs. As second- or later-line therapy, ORR was higher with camrelizumab (34.1%), followed by pembrolizumab (26.3%), JS001 (23.3%), and nivolumab (19.0%); whereas ORR with first-line nivolumab reached 40%. Additionally, first-line camrelizumab+chemotherapy achieved a dramatically higher ORR than that with chemotherapy alone (90.9% vs. -

Antimicrobial Activity of Cationic
ANTIMICROBIAL ACTIVITY OF CATIONIC ANTISEPTICS IN LAYER-BY-LAYER THIN FILM ASSEMBLIES A Thesis by CHARLENE MYRIAH DVORACEK Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE May 2009 Major Subject: Mechanical Engineering ANTIMICROBIAL ACTIVITY OF CATIONIC ANTISEPTICS IN LAYER-BY-LAYER THIN FILM ASSEMBLIES A Thesis by CHARLENE MYRIAH DVORACEK Submitted to the Office of Graduate Studies of Texas A&M University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE Approved by: Chair of Committee, Jaime Grunlan Committee Members, Michael Benedik Xinghang Zhang Head of Department, Dennis O'Neal May 2009 Major Subject: Mechanical Engineering iii ABSTRACT Antimicrobial Activity of Cationic Antiseptics in Layer-by-Layer Thin Film Assemblies. (May 2009) Charlene Myriah Dvoracek, B.S., Rose-Hulman Institute of Technology Chair of Advisory Committee: Dr. Jaime Grunlan Layer-by-layer (LbL) assembly has proven to be a powerful technique for assembling thin films with a variety of properties including electrochromic, molecular sensing, oxygen barrier, and antimicrobial. LbL involves the deposition of alternating cationic and anionic ingredients from solution, utilizing the electrostatic charges to develop multilayer films. The present work incorporates cationic antimicrobial agents into the positively-charged layers of LbL assemblies. When these thin films are exposed to a humid environment, the antimicrobial molecules readily diffuse out and prevent bacterial growth. The influence of exposure time, testing temperature, secondary ingredients and number of bilayers on antimicrobial efficacy is evaluated here. Additionally, film growth and microstructure are analyzed to better understand the behavior of these films. -

COVID-19 Testing FAQ
COVID-19 Testing FAQ GENERAL INFORMATION What kind of COVID tests are being offered? - The below tests are available to all TAMU students, faculty and staff: o Antibody blood/serology test ($): available for a minimal charge at Student Health Services; determines the likelihood of a previous COVID-19 infection o Curative nasal swab/PCR: self-collect nasal swab funded by Texas A&M University System; determines an active COVID-19 infection o SHS nasal swab/PCR ($): self-collect nasal swab available for a minimal charge at Student Health Services; determines an active COVID-19 infection o Saliva sample: self-collect saliva sample funded by Texas A&M University System; non-diagnostic COVID test Which test should I choose? - Curative nasal swab and saliva sample are funded by Texas A&M University and free of charge. - Antibody blood/serology test and SHS nasal swab are available at Student Health Services for a minimal charge. Insurance will be billed for these tests. Insurance may cover the cost in full, but it is encouraged to check with your insurance provider before scheduling the test. An SHS medical provider will follow up with the patient and assist in his/her care before and after results are available, and will be able to answer any questions the individual may have regarding COVID-19. If I think I have been exposed to COVID, when should I get tested? - If you are sick and/or had a potential exposure to COVID, visit the Texas A&M University COVID page for detailed guidance: https://www.tamu.edu/coronavirus/sick-campus-members/. -

Reseptregisteret 2013–2017 the Norwegian Prescription Database
LEGEMIDDELSTATISTIKK 2018:2 Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Reseptregisteret 2013–2017 Tema: Legemidler og eldre The Norwegian Prescription Database 2013–2017 Topic: Drug use in the elderly Christian Berg Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Utgitt av Folkehelseinstituttet/Published by Norwegian Institute of Public Health Område for Helsedata og digitalisering Avdeling for Legemiddelstatistikk Juni 2018 Tittel/Title: Legemiddelstatistikk 2018:2 Reseptregisteret 2013–2017 / The Norwegian Prescription Database 2013–2017 Forfattere/Authors: Christian Berg, redaktør/editor Hege Salvesen Blix Olaug Fenne Kari Furu Vidar Hjellvik Kari Jansdotter Husabø Irene Litleskare Marit Rønning Solveig Sakshaug Randi Selmer Anne-Johanne Søgaard Sissel Torheim Acknowledgement: Julie D. W. Johansen (English text) Bestilling/Order: Rapporten kan lastes ned som pdf på Folkehelseinstituttets nettsider: www.fhi.no The report can be downloaded from www.fhi.no Grafisk design omslag: Fete Typer Ombrekking: Houston911 Kontaktinformasjon/Contact information: Folkehelseinstituttet/Norwegian Institute of Public Health Postboks 222 Skøyen N-0213 Oslo Tel: +47 21 07 70 00 ISSN: 1890-9647 ISBN: 978-82-8082-926-9 Sitering/Citation: Berg, C (red), Reseptregisteret 2013–2017 [The Norwegian Prescription Database 2013–2017] Legemiddelstatistikk 2018:2, Oslo, Norge: Folkehelseinstituttet, 2018. Tidligere utgaver / Previous editions: 2008: Reseptregisteret 2004–2007 / The Norwegian Prescription Database 2004–2007 2009: Legemiddelstatistikk 2009:2: Reseptregisteret 2004–2008 / The Norwegian Prescription Database 2004–2008 2010: Legemiddelstatistikk 2010:2: Reseptregisteret 2005–2009. Tema: Vanedannende legemidler / The Norwegian Prescription Database 2005–2009.