Review Functional and Oncological Outcomes with Male Nerve Sparing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Functional Anatomy of the Hypothalamic–Pituitary–Gonadal Axis and 1 the Male Reproductive Tract
Cambridge University Press 978-1-107-01212-7 - Fertility Preservation in Male Cancer Patients Editor-in-Chief John P. Mulhall Excerpt More information Section 1 Anatomy and physiology Chapter Functional anatomy of the hypothalamic–pituitary–gonadal axis and 1 the male reproductive tract Nelson E. Bennett Jr. Anatomy of reproductive function The reproductive functional axis of the male can be divided into three major subdivisions: (1) the hypo- thalamus, (2) the pituitary gland, and (3) the testis. Each level elaborates a signal, or transmitter molecule, that stimulates or inhibits the subsequent level of the axis. The end result is the production and expulsion of semen that contains spermatozoa. This chapter exam- ines the hypothalamic–pituitary–gonadal (HPG) axis, and reviews the functional anatomy of the testis, epi- didymis, vas deferens, seminal vesicles, prostate, and penis. Hypothalamus and anterior pituitary gland The control of male sexual and reproductive func- tion begins with secretion of gonadotropin-releasing hormone (GnRH) by the hypothalamus (Fig. 1.1). This hormone in turn stimulates the anterior pituitary gland to secrete two downstream hormones (termed gonadotropins). These hormones are luteinizing hor- mone (LH) and follicle-stimulating hormone (FSH). LH is the primary stimulus for the testicular secre- tion of testosterone, while FSH mainly stimulates spermatogenesis. Gonadotropin-releasing hormone (GnRH) Figure 1.1. Feedback regulation of the hypothalamic– The neuronal cells of the arcuate nuclei of the hypo- pituitary–gonadal (HPG) axis in males. Positive (stimulatory) effects are shown by + and inhibitory (negative feedback) effects by –. thalamus secrete GnRH, a 10-amino-acid peptide. The GnRH, gonadotropin-releasing hormone; LH, luteinizing hormone; endingsoftheseneuronsterminateinthemedian FSH, follicle-stimulating hormone. -

Male Sexual Impotence: a Case Study in Evaluation and Treatment
FAMILY PRACTICE GRAND ROUNDS Male Sexual Impotence: A Case Study in Evaluation and Treatment John G. Halvorsen, MD, MS, Craig Mommsen, MD, James A. Moriarty, MD, David Hunter, MD, Michael Metz, PhD, and Paul Lange, MD Minneapolis, Minnesota R. JOHN HALVORSEN {Assistant Professor, De cavernosa. There is also a very important suspensory lig D partment o f Family Practice and Community ament—a triangular structure attached at the base of the Health)-. Male sexual impotence is the inability to obtain penis and to the pubic arch blending with Buck’s fascia and sustain an erection adequate to permit satisfactory around the penis—that is responsible for forming the angle penetration and completion of sexual intercourse. Im of the erect penis. potence is defined as primary if erections have never oc The arterial supply to the penis flows from the aorta curred, and secondary if they have previously occurred through the common iliac, hypogastric, and internal pu but subsequently have ceased. The cause of sexual im dendal systems. The artery of the penis is a branch of the potence may be psychogenic, organic, or mixed. In the internal pudendal artery and has four branches. The first past, the common belief was that 90 percent of impotence branch, the artery to the bulb, supplies the corpus spon was psychological.1,2 Recent research indicates, however, giosum, the glans, and the bulb. The second branch is the that over one half of men with impotence suffer from an urethral artery. The artery of the penis then terminates organic disorder, although often there is considerable into the dorsal artery of the penis (which supplies the deep overlap between both psychological and organic causes.3,4 fascia, the penile skin, and the frenulum) and the deep or A knowledge of the anatomy of the penis and the com profunda branch (which supplies the corpora cavernosa plex physiology of erection is necessary to understand the on each side). -

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

Vascularization of the Penis of a Man
Roczniki Akademii Medycznej w Białymstoku · Vol. 49, 2004 · Annales Academiae MedicaeVascularization Bialostocensis of the penis of a man 285 Vascularization of the penis of a man Okolokulak E, Volchkevich D The Human Anatomy Department, Grodno State Medical University, Grodno, Belarus Abstract Conclusions: The penis receives blood from external and internal pudendal arteries, which are very variable. The Purpose: The study of the features of the blood supply of venous blood of the penis flows off in three types of veins. a penis of the man. Material and methods: Macromicropreparation, angio- graphy, corrosion method, morphometry, statistical method. Key words: penis, veins of penis, arteries of penis, erectile Results: The penis has three venous collector-execut- dysfunction. ing outflow of blood. First of them is submitted surface dorsal vein, which is shaped from small-sized venous ves- sels of skin, subcutaneous fat and surface fascia of penis. Introduction The beginning deep dorsal vein, which will derivate second venous collector, gives veniplex of head of the penis. The The development of the medical technology has deepened spongy veins outstanding as third venous collector, reach the knowledge of organic violations of gears of erection. It was the bulb of penis, where they receive small-sized bulbar vein. straightened out, that more than 50% from them cause vascular The arterial blood supply of penis happens at the expense of disorders [1-4]. It has given a particular push to more detailed external and internal pudendal arteries. The external puden- learning extra- and intraorgans vessels of the penis. At the same dal artery starts from an internal wall of femoral artery on time, the problems of vascularization and relationships of blood 2.5-2.7 cm below inguinal ligament. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
www.kjurology.org DOI:10.4111/kju.2010.51.1.70 Case Report Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis Kyung Hwa Choi, Seung Hwan Lee, Won Sug Jung1, Byung Ha Chung Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, 1National Health Insurance Corporation Ilsan Hospital, Goyang, Korea We report a rare case of robot-assisted laparoscopic radical prostatectomy (RARP) in Article History: a patient with a preexisting penile prosthesis. In this case, we completed RARP without received 27 August, 2009 14 October, 2009 removing the reservoir by using a deflation-inflation technique, and there were no com- accepted plications related to the prosthesis. The patient had a negative surgical margin. The Corresponding Author: preserved three-piece inflatable penile prosthesis continued to function properly in 1 Byung Ha Chung month. Reservoir-preserving RARP is technically feasible and safe. However, it is im- Department of Urology, Yonsei portant to be aware of device-related complications. Long-term studies on the mechan- University Health System, Gangnam Severance Hospital, 712, Eonju-ro, ical survival rate and patient satisfaction should be also performed. Dogok-dong, Gangnam-gu, Seoul Key Words: Robotics, Prostatectomy, Penile prosthesis, Prostatic neoplasms 135-720, Korea TEL: +82-2-2019-3474 FAX: +82-2-3462-8887 E-mail: [email protected] Prostate cancer has been reported to occur most frequently CASE REPORT in men over 40 years of age. In organ-confined cases, radical prostatectomy is the treatment of choice. After the in- 1. Patient troduction of the da VinciⓇ surgical system (Intuitive The patient was a 64-year-old male diagnosed with aci- Surgical, Sunnyvale, USA), robot-assisted laparoscopic nar-type prostate adenocarcinoma with a Gleason score of radical prostatectomy (RARP) has become a mainstay of 6 (3+3) by prostate biopsy. -
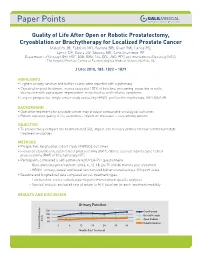
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder -

Robotic-Assisted Laparoscopic Radical Prostatectomy After Aborted Retropubic Radical Prostatectomy
J Robotic Surg (2013) 7:301–304 DOI 10.1007/s11701-012-0377-9 CASE REPORT Robotic-assisted laparoscopic radical prostatectomy after aborted retropubic radical prostatectomy Keith J. Kowalczyk • Andy C. Huang • Stephen B. Williams • Hua-yin Yu • Jim C. Hu Received: 11 March 2012 / Accepted: 31 July 2012 / Published online: 19 August 2012 Ó Springer-Verlag London Ltd 2012 Abstract Robotic-assisted laparoscopic prostatectomy of the endopelvic fascia due to poor visualization, a (RALP) has surged in popularity since US Food and Drug prominent pubic tubercle, and a narrow pelvis. The Administration approval in 2000. Advantages include enhanced visualization and precision of the robotic plat- improved visualization and increased instrument dexterity form allowed adequate exposure of the prostate and within the pelvis. Obesity and narrow pelves have been allowed us to proceed with an uncomplicated prostatecto- associated with increased difficulty during open retropubic my, which was not possible to perform easily via an open radical prostatectomy (RRP), but the robotic platform approach. The bladder was densely adherent to the pubis theoretically allows one to perform a radical prostatectomy and the anterior prostatic contour and apex were difficult to despite these challenges. We present an example of a develop due to a dense fibrotic reaction from the previous RALP performed following an aborted RRP. A 49-year-old endopelvic fascia incision. However, we were able to male with intermediate risk prostate cancer and body mass successfully complete RALP with subtle technical modi- index of 38 kg/m2 presented for RALP after RRP was fications. Estimated blood loss was 160 mL and operating aborted by an experienced open surgeon following incision time was 145 min. -

SŁOWNIK ANATOMICZNY (ANGIELSKO–Łacinsłownik Anatomiczny (Angielsko-Łacińsko-Polski)´ SKO–POLSKI)
ANATOMY WORDS (ENGLISH–LATIN–POLISH) SŁOWNIK ANATOMICZNY (ANGIELSKO–ŁACINSłownik anatomiczny (angielsko-łacińsko-polski)´ SKO–POLSKI) English – Je˛zyk angielski Latin – Łacina Polish – Je˛zyk polski Arteries – Te˛tnice accessory obturator artery arteria obturatoria accessoria tętnica zasłonowa dodatkowa acetabular branch ramus acetabularis gałąź panewkowa anterior basal segmental artery arteria segmentalis basalis anterior pulmonis tętnica segmentowa podstawna przednia (dextri et sinistri) płuca (prawego i lewego) anterior cecal artery arteria caecalis anterior tętnica kątnicza przednia anterior cerebral artery arteria cerebri anterior tętnica przednia mózgu anterior choroidal artery arteria choroidea anterior tętnica naczyniówkowa przednia anterior ciliary arteries arteriae ciliares anteriores tętnice rzęskowe przednie anterior circumflex humeral artery arteria circumflexa humeri anterior tętnica okalająca ramię przednia anterior communicating artery arteria communicans anterior tętnica łącząca przednia anterior conjunctival artery arteria conjunctivalis anterior tętnica spojówkowa przednia anterior ethmoidal artery arteria ethmoidalis anterior tętnica sitowa przednia anterior inferior cerebellar artery arteria anterior inferior cerebelli tętnica dolna przednia móżdżku anterior interosseous artery arteria interossea anterior tętnica międzykostna przednia anterior labial branches of deep external rami labiales anteriores arteriae pudendae gałęzie wargowe przednie tętnicy sromowej pudendal artery externae profundae zewnętrznej głębokiej -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular