A Study of the Commodification of Health Services in Ireland
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Economics of Commodity Market Manipulation: a Survey
The Economics of Commodity Market Manipulation: A Survey Craig Pirrong Bauer College of Business University of Houston February 11, 2017 1 Introduction The subject of market manipulation has bedeviled commodity markets since the dawn of futures trading. Allegations of manipulation have been extremely commonplace, but just what constitutes manipulation, and how charges of manipulation can be proven, have been the subject of intense controversy. The remark of a waggish cotton trader in testimony before a Senate Com- mittee in this regard is revealing: “the word manipulation . initsuse isso broad as to include any operation of the cotton market that does not suit the gentleman who is speaking at the moment.” The Seventh Circuit Court of Appeals echoed this sentiment, though less mordantly, in its decision in the case Cargill v. Hardin: “The methods and techniques of manipulation are limited only by the ingenuity of man.” Concerns about manipulation have driven the regulation of commodity markets: starting with the Grain Fu- tures Act of 1922, United States law has proscribed manipulation, including 1 specifically “corners” and “squeezes.” Exchanges have an affirmative duty to police manipulation, and in the United States, the Commodity Futures Trad- ing Commission and the Department of Justice can, and have exercised, the power to prosecute alleged manipulators. Nonetheless, manipulation does occur. In recent years, there have been allegations that manipulations have occurred in, inter alia, soybeans (1989), copper (1995), gold (2004-2014) nat- ural gas (2006), silver (1998, 2007-2014), refined petroleum products (2008), cocoa (2010), and cotton (2011). Manipulation is therefore both a very old problem, and a continuing one. -

Price Discovery in the Futures and Cash Market for Sugar
University of Wisconsin-Madison Department of Agricultural & Applied Economics March 2005 Staff Paper No. 469 Price Discovery in the World Sugar Futures and Cash Markets: Implications for the Dominican Republic By Hector Zapata T. Randall Fortenbery Delroy Armstrong __________________________________ AGRICULTURAL & APPLIED ECONOMICS ____________________________ STAFF PAPER SERIES Copyright © 2005 Hector Zapata, T. Randall Fortenbery and Delroy Armstrong. All rights reserved. Readers may make verbatim copies of this document for non-commercial purposes by any means, provided that this copyright notice appears on all such copies. Price Discovery in the World Sugar Futures and Cash Markets: Implications for the Dominican Republic by Hector O Zapata Department of Agricultural Economics & Agribusiness Louisiana State University Baton Rouge, Louisiana Phone: (225) 578-2766 Fax: (225) 578-2716 e-mail: [email protected] T. Randall Fortenbery Department of Agricultural and Applied Economics University of Wisconsin – Madison Madison, Wisconsin Phone: (608) 262-4908 Fax: (608) 262-4376 e-mail: [email protected] Delroy Armstrong Department of Agricultural Economics & Agribusiness Louisiana State University Baton Rouge, Louisiana Phone: (225) 578-2757 Fax: (225) 578-2716 e-mail: [email protected] ___________ 1Hector Zapata and D. Armstrong are Professor and research assistant, respectively, Department of Agricultural Economics and Agribusiness, Louisiana State University, Baton Rouge, Louisiana. Dr. T Randall Fortenbery is the Renk Professor of Agribusiness, at the Department of Agriculture and Applied Economics, University of Wisconsin, Madison, Wisconsin. Price Discovery in the World Sugar Futures and Dominican Republic Cash Market Abstract This paper examines the relationship between #11 sugar futures prices traded in New York and the world cash prices for exported sugar. -

Commodity Prices and Markets, East Asia Seminar on Economics, Volume 20
This PDF is a selection from a published volume from the National Bureau of Economic Research Volume Title: Commodity Prices and Markets, East Asia Seminar on Economics, Volume 20 Volume Author/Editor: Takatoshi Ito and Andrew K. Rose, editors Volume Publisher: University of Chicago Press Volume ISBN: 0-226-38689-9 ISBN13: 978-0-226-38689-8 Volume URL: http://www.nber.org/books/ito_09-1 Conference Date: June 26-27, 2009 Publication Date: February 2011 Chapter Title: The Relationship between Commodity Prices and Currency Exchange Rates: Evidence from the Futures Markets Chapter Authors: Kalok Chan, Yiuman Tse, Michael Williams Chapter URL: http://www.nber.org/chapters/c11859 Chapter pages in book: (47 - 71) 2 The Relationship between Commodity Prices and Currency Exchange Rates Evidence from the Futures Markets Kalok Chan, Yiuman Tse, and Michael Williams 2.1 Introduction We examine relationships among currency and commodity futures markets based on four commodity- exporting countries’ currency futures returns and a range of index- based commodity futures returns. These four commodity- linked currencies are the Australian dollar, Canadian dollar, New Zealand dollar, and South African rand. We fi nd that commodity/currency relation- ships exist contemporaneously, but fail to exhibit Granger- causality in either direction. We attribute our results to the informational efficiency of futures markets. That is, information is incorporated into the commodity and cur- rency futures prices rapidly and simultaneously on a daily basis. There are a few studies on the relationship between currency and com- modity prices. A recent study by Chen, Rogoff, and Rossi (2008) using quar- terly data fi nds that currency exchange rates of commodity- exporting coun- tries have strong forecasting ability for the spot prices of the commodities they export. -

Cointegration Analysis of the World's Sugar Market
Economics COINTEGRATION ANALYSIS OF THE WORLD’S SUGAR MARKET: THE EXISTENCE OF THE LONG-TERM EQUILIBRIUM Elena Kuzmenko1, Luboš Smutka2, Wadim Strielkowski3, Justas Štreimikis4, Dalia Štreimikienė5 1 Czech University of Life Sciences, Faculty of Economics and Management, Department of Economics, Czech Republic, ORCID: 0000-0002-2091-4630, [email protected]; 2 Czech University of Life Sciences, Faculty of Economics and Management, Department of Economics, Czech Republic, ORCID: 0000-0001-5385-1333, [email protected]; 3 Czech University of Life Sciences, Faculty of Economics and Management, Department of Economics, Czech Republic, ORCID: 0000-0001-6113-3841, [email protected]; 4 University of Economics and Human Science in Warsaw, Faculty of Management and Finances, Finance and Accounting Department, Poland, ORCID: 0000-0003-2619-3229, [email protected]; 5 Vilnius University, Kaunas Faculty, Institute of Social Sciences and Applied Informatics, Lithuania, ORCID: 0000-0002-3247-9912, [email protected] (corresponding author). Abstract: This paper addresses the issue of interconnection among major sugar markets and commodity/exchange stocks in different parts of the world using the Johansen cointegration approach and vector error correction model. Due to a high degree of sugar market fragmentation and corresponding diversity in price levels and its volatility in different regions, the results of our analysis sheds some light on the very fact of a ‘single’ global sugar market existence and can be important not just with regard to producers and buyers of sugar but for the international investors as well, both in the light of risk governance and maximizing profitability. Using the evaluation of the extent of connection among regional sugar markets, one can assess potential benefits available to investors through international diversification between the analyzed markets. -
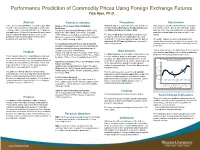
Performance Prediction of Commodity Prices Using Foreign Exchange Futures Yisa Ajao, Ph.D
Performance Prediction of Commodity Prices Using Foreign Exchange Futures Yisa Ajao, Ph.D. Abstract Relevant Literature Procedures Conclusions In an experimental quantitative research design, data Origins of Dow Jones Financial Markets Historical data were downloaded from the websites of This study demonstrated that historical records from from the Futures Market for commodities and foreign Predictions the U.S. Commodity Futures Trading Commission Forex futures can be paired with matching records exchange futures covering 1986-2011 were obtained The theories developed by Fibonacci (1175-1250), and Wikiposit Historical Futures Data. from wheat (or any commodity) futures and obtain a and addressed. A General Regression Neural Network Dow (1851-1902), Elliot (1871-1948), and Gann prediction of market prices to within a 4.42% error was overlaid on this data to deduce a time-series (1878-1955) are essentially the backbones to the The data included daily commodity closing prices in margin. prediction model for wheat prices. Performance study of the movements of financial markets (Frost & the futures market for each trading day from 1985 prediction error was only 4.42%. Prechter, 2005; Schlanger, 2009) through 2011. From these data bank, specific data for The public, traders, investors, and analysts can wheat and US $1 Treasury Note were extracted for include this method as a new tool in the arsenal in the Forecasting Commodity Prices and Comments data mining purposes. ongoing search for a more reliable commodity futures Questions regarding forecast accuracy and financial predictions. markets eventually became a substantive topic of retrospective studies exemplified by Data Analysis This method can serve as confirmation of the results of Problem Hansen and Hodrick (1980), Turnovsky (1983), Fama other analytic and fundamental methods of obtaining (1984), Hodrick and Srivastava (1986), (Choe, 1990a), The Runs test was used to validate data randomness. -

Karl Polanyi's Critique
Author: Block • Filename: POMF-CH.4 LHP: THE POWER OF MARKET FUNDAMENTALISM RHP: TURNING THE TABLES Words: 6,291 / Chars: 40,895 • 1 • Printed: 06/18/14 8:39 PM Author: Block • Filename: POMF-CH.4 4 Turning the Tables Polanyi’s Critique of Free Market Utopianism In The Rhetoric of Reaction, Albert Hirschman (1991), identifies three distinct “rhetorics” that conservatives have used to discredit reform movements since the French Revolution. Chapter 6 of this volume is devoted to the “rhetoric of perversity”—the claim that a reform will have exactly the opposite of its intended effects and will hurt the intended beneficiaries. The second, “the rhetoric of jeopardy” is exemplified by Friedrich Hayek’s The Road to Serfdom (2007 [1944]); it is the claim that a reform will erode the freedoms we depend on. Hirschman’s third is the “rhetoric of futility”—the insistence that a reform is literally impossible because it goes against everything that we know is natural about human beings and social arrangements. This is the ploy that Malthus used in his Essay on the Principle of Population (1992 [1798]) to challenge the egalitarian ideas of William Godwin. Malthus professed to admire the beauty of Godwin’s vision, but he ultimately dismissed the vision as impossible. It was futile because Malthus declared it to be against the laws of nature—in other words, utopian. The rhetoric of futility is the main weapon that conservative intellectuals have wielded against socialists and communists for more than two centuries. They contend that an egalitarian social order would destroy any incentives for effort and creativity, which makes it utterly inconsistent with human nature. -

Hydro-Social Permutations of Water Commodification in Blantyre City, Malawi
Hydro-Social Permutations of Water Commodification in Blantyre City, Malawi A thesis submitted to the University of Manchester for the degree of Doctor of Philosophy in the Faculty of Humanities 2014 Isaac M.K. Tchuwa School of Environment Education and Development Table of Contents Table of Contents ............................................................................................................ 2 List of Figures ................................................................................................................. 6 List of Tables ................................................................................................................... 7 List of Graphs ................................................................................................................. 7 List of Photos .................................................................................................................. 8 List of Maps .................................................................................................................... 9 Abstract ......................................................................................................................... 10 Declaration .................................................................................................................... 11 Copyright Statement .................................................................................................... 12 Acknowledgements .................................................................................................... -

Commodity Futures Markets
Task Force on Commodity Futures Markets Final Report TECHNICAL COMMITTEE OF THE INTERNATIONAL ORGANIZATION OF SECURITIES COMMISSIONS MARCH 2009 CONTENTS Chapter Page Executive Summary 3 Background 4 Discussion 6 Volatility and the role of increased participation by financial participants in 6 the Futures Markets Greater transparency of fundamental commodity market information is 11 needed Transparency and Market Surveillance 14 Enforcement Challenges Involving Commodity Futures Markets 18 Enhancing Global Co-Operation 20 Appendix 22 2 Executive Summary The IOSCO Task Force on Commodity Futures Markets (Task Force) was formed following the concerns expressed by the G-8 Finance Ministers regarding the price rises and volatility in agricultural and energy in 2008. The Task Force has made the following conclusions and practical recommendations: Reports by international organizations, central banks and regulators in response to the above concerns that were reviewed by the Task Force suggest that economic fundamentals, rather than speculative activity, are a plausible explanation for recent price changes in commodities. However, given the complexity and often opacity of factors that drive price discovery in futures markets, and the critical importance of these issues to world economies, continued monitoring is appropriate to improve understanding of futures market price formation and the interaction between regulated futures markets and related commodity markets1; The Task Force has identified factors that potentially inhibit the ability of commodity futures market regulators (futures market regulators)2 to access relevant information concerning the related commodity markets, over which futures market regulators generally do not have authority, that may be needed to understand fully price formation in a particular futures market contract or to detect manipulative or other abusive trading by market participants holding large positions in those commodity contracts. -

The Dynamics of Commodity Spot and Future Markets
The Dynamics of Commodity Spot and Futures Markets: A Primer Robert S. pindyck* I discuss the short-run dynamics of commodity prices, production, and inventories, as well as the sources and effects of market volatility. I explain how prices, rates of production, ana’ inventory levels are interrelated, and are determined via equilibrium in two interconnected markets: a cash market for spot purchases and sales of the commodity, and a market for storage. I show how equilibrium in these markets affects and is affected by changes in the level qf price volatility. I also explain the role and behavior of commodity futures markets, and the relationship between spot prices, futures prices, and inventoql behavior. I illustrate these ideas with data for the petroleum complex - crude oil, heating oil, and gasoline - over the past two decades. INTRODUCTION The markets for oil products, natural gas, and many other commodities are characterized by high levels of volatility. Prices and inventory levels fluctuate considerably from week to week, in part predictably (e.g., due to seasonal shifts in demand) and in part unpredictably. Furthermore, levels of volatility themselves vary over time. This paper discusses the short-run dynamics of commodity prices, production, and inventories, as well as the sources and effects of market volatility. I explain how prices, rates of production, and inventory levels are interrelated, and are determined via equilibrium in two interconnected markets: a cash market for spot purchases and sales of the commodity, and a market for storage. I also explain how equilibrium in these markets affects and is affected by changes in the level of price volatility. -

An Overview of Major Sources of Data and Analyses Relating to Physical Fundamentals in International Commodity Markets
AN OVERVIEW OF MAJOR SOURCES OF DATA AND ANALYSES RELATING TO PHYSICAL FUNDAMENTALS IN INTERNATIONAL COMMODITY MARKETS No. 202 June 2011 AN OVERVIEW OF MAJOR SOURCES OF DATA AND ANALYSES RELATING TO PHYSICAL FUNDAMENTALS IN INTERNATIONAL COMMODITY MARKETS Pilar Fajarnes No. 202 June 2011 UNCTAD/OSG/DP/2011/2 ii The opinions expressed in this paper are those of the author and are not to be taken as the official views of the UNCTAD Secretariat or its Member States. The designations and terminology employed are also those of the author. UNCTAD Discussion Papers are read anonymously by at least one referee, whose comments are taken into account before publication. Comments on this paper are invited and may be addressed to the authors, c/o the Publications Assistant, Macroeconomic and Development Policies Branch (MDPB), Division on Globalization and Development Strategies (DGDS), United Nations Conference on Trade and Development (UNCTAD), Palais des Nations, CH-1211 Geneva 10, Switzerland (Telefax no: +41 (0)22 917 0274 / Telephone no: +41 (0)22 917 5896). Copies of Discussion Papers may also be obtained from this address. UNCTAD Discussion Papers are available on the UNCTAD website at http://www.unctad.org. JEL classification: O13, G14, D83 iii Contents Page Abstract ........................................................................................................................................................ 1 I. INTRODUCTION ................................................................................................................................ -

Commodities, World Markets, and Early American Labor Donovan P
University of Connecticut OpenCommons@UConn Honors Scholar Theses Honors Scholar Program Spring 5-1-2017 The fforE ts of Trade: Commodities, World Markets, and Early American Labor Donovan P. Fifield University of Connecticut, [email protected] Follow this and additional works at: https://opencommons.uconn.edu/srhonors_theses Recommended Citation Fifield, Donovan P., "The Efforts of Trade: Commodities, World Markets, and Early American Labor" (2017). Honors Scholar Theses. 527. https://opencommons.uconn.edu/srhonors_theses/527 The Efforts of Trade: Commodities, World Markets, and Early American Labor By: Donovan Fifield University of Connecticut Spring 2017 Fifield 1 Variation is a noteworthy characteristic of early American labor. Within different regions, one would have seen many different local economies and social systems revolving around how people were employed. From this variation arises the question of why labor took different forms in different areas. This consideration relies on multiple factors pertaining to both society and the natural environment. These factors could be seen to have existed in a complex system where no one factor was the primary determining power involved in the way labor manifested itself in a region. However, common patterns did in fact emerge in regions with similar labor systems, but such patterns were not fully determinative so much as they provided an environment where certain forms of labor could take hold. Despite the dynamic nature of this system, one common tie can be seen to have had a ubiquitous effect on each early American region, which is the globalization of the commodity. The commodity itself, while varying greatly in type and production, formed a “backbone” around which the economy developed. -

Commodities: Hedging, Regulation, and Documentation
Commodities: Hedging, Regulation, and Documentation Kathryn F. Murphy Husch Blackwell What is a Commodity? . Black’s Law Dictionary definition of Commodities: Goods, wares, and merchandise of any kind; movables; articles of trade or commerce. Commodity Market: A market that trades in the economic sector rather than manufactured products. There are over fifty commodity markets worldwide © 2017 Husch Blackwell LLP © 2017 Husch Blackwell LLP. All Rights Reserved Types of Commodities . Grains, Food & Fiber: – corn, oats, rice, soybeans, rapeseed, soybean meal, soybean oil, wheat, milk, cocoa, coffee, cotton, sugar, orange juice . Livestock & Meat: – lean hogs, live cattle, feeder cattle . Energy: – WTI crude oil, Brent crude, ethanol, natural gas, heating oil, gulf coast gasoline, RBOB gasoline, propane, PTA . Metals: – Copper, lead, zinc, tin, aluminum, nickel, cobalt, recycled steel, molybdenum, gold, platinum, palladium, silver © 2017 Husch Blackwell LLP Commodity Price Risk - Hedging . Protection against the impact of a potential negative event. – similar to insurance – hedging occurs almost everywhere, and we see it everyday . Hedging tool for commodity price risk – Financial derivative products © 2017 Husch Blackwell LLP © 2017 Husch Blackwell LLP. All Rights Reserved Financial Derivative Products . Financial derivative products are used for risk management purposes (hedging) or to increase exposure to price movements (speculation) – futures, options, swaps. – over 90% of the 500 largest companies worldwide use derivative products to manage and hedge against their business risks . Derives its value from an underlying asset – commodity (soybeans) or financial (interest rates) – Example: interest rate swap – 2 party contract for the exchange of interest rate payments at set times – exchange of a fixed interest rate for a floating interest rate to reduce exposure to interest rate fluctuations.