FREE INQUIRY in CREATIVE SOCIOLOGY Volume34 Number I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Certified Products List
THE ART & CREATIVE MATERIALS INSTITUTE, INC. Street Address: 1280 Main St., 2nd Floor Mailing Address: P.O. Box 479 Hanson, MA 02341 USA Tel. (781) 293-4100 Fax (781) 294-0808 www.acminet.org Certified Products List March 28, 2007 & ANSI Performance Standard Z356._X BUY PRODUCTS THAT BEAR THE ACMI SEALS Products Authorized to Bear the Seals of The Certification Program of THE ART & CREATIVE MATERIALS INSTITUTE, INC. Since 1940, The Art & Creative Materials Institute, Inc. (“ACMI”) has been evaluating and certifying art, craft, and other creative materials to ensure that they are properly labeled. This certification program is reviewed by ACMI’s Toxicological Advisory Board. Over the years, three certification seals had been developed: The CP (Certified Product) Seal, the AP (Approved Product) Seal, and the HL (Health Label) Seal. In 1998, ACMI made the decision to simplify its Seals and scale the number of Seals used down to two. Descriptions of these new Seals and the Seals they replace follow: New AP Seal: (replaces CP Non-Toxic, CP, AP Non-Toxic, AP, and HL (No Health Labeling Required). Products bearing the new AP (Approved Product) Seal of the Art & Creative Materials Institute, Inc. (ACMI) are certified in a program of toxicological evaluation by a medical expert to contain no materials in sufficient quantities to be toxic or injurious to humans or to cause acute or chronic health problems. These products are certified by ACMI to be labeled in accordance with the chronic hazard labeling standard, ASTM D 4236 and the U.S. Labeling of Hazardous NO HEALTH LABELING REQUIRED Art Materials Act (LHAMA) and there is no physical hazard as defined with 29 CFR Part 1910.1200 (c). -

Some Products in This Line Do Not Bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal
# Some products in this line do not bear the AP Seal. Product Categories Manufacturer/Company Name Brand Name Seal Adhesives, Glue Newell Brands Elmer's Extra Strength School AP Glue Stick Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Gold Liner AP Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Silver Liner AP Adhesives, Glue New Port Sales, Inc. All Gloo CL Adhesives, Glue Leeho Co., Ltd. Leeho Window Paint Sparkler AP Adhesives, Glue Newell Brands Elmer's Xtreme School Glue AP Adhesives, Glue Newell Brands Elmer's Craftbond All-Temp Hot AP Glue Sticks Adhesives, Glue Daler-Rowney Limited Rowney Rabbit Skin AP Adhesives, Glue Kuretake Co., Ltd. ZIG Decoupage Glue AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2 Way Glue AP Squeeze & Roll Adhesives, Glue Kuretake Co., Ltd. Kuretake Oyatto-Nori AP Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Chisel Tip Adhesives, Glue Kuretake Co., Ltd. ZIG Memory System 2Way Glue AP Jumbo Tip Adhesives, Glue EK Success Martha Stewart Crafts Fine-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts Wide-Tip AP Glue Pen Adhesives, Glue EK Success Martha Stewart Crafts AP Ballpoint-Tip Glue Pen Adhesives, Glue STAMPIN' UP Stampin' Up 2 Way Glue AP Adhesives, Glue Creative Memories Creative Memories Precision AP Point Adhesive Adhesives, Glue Rich Art Color Co., Inc. Rich Art Washable Bits & Pieces AP Glitter Glue Adhesives, Glue Speedball Art Products Co. Best-Test One-Coat Cement CL Adhesives, Glue Speedball Art Products Co. Best-Test Rubber Cement CL Adhesives, Glue Speedball Art Products Co. -
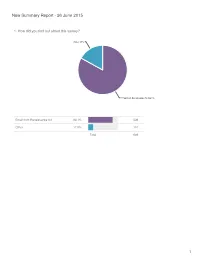
New Summary Report - 26 June 2015
New Summary Report - 26 June 2015 1. How did you find out about this survey? Other 17% Email from Renaissance Art 83.1% Email from Renaissance Art 83.1% 539 Other 17.0% 110 Total 649 1 2. Where are you from? Australia/New Zealand 3.2% Asia 3.7% Europe 7.9% North America 85.2% North America 85.2% 553 Europe 7.9% 51 Asia 3.7% 24 Australia/New Zealand 3.2% 21 Total 649 2 3. What is your age range? old fart like me 15.4% 21-30 22% 51-60 23.3% 31-40 16.8% 41-50 22.5% Statistics 21-30 22.0% 143 Sum 20,069.0 31-40 16.8% 109 Average 36.6 41-50 22.5% 146 StdDev 11.5 51-60 23.3% 151 Max 51.0 old fart like me 15.4% 100 Total 649 3 4. How many fountain pens are in your collection? 1-5 23.3% over 20 35.8% 6-10 23.9% 11-20 17.1% Statistics 1-5 23.3% 151 Sum 2,302.0 6-10 23.9% 155 Average 5.5 11-20 17.1% 111 StdDev 3.9 over 20 35.8% 232 Max 11.0 Total 649 4 5. How many pens do you usually keep inked? over 10 10.3% 7-10 12.6% 1-3 40.7% 4-6 36.4% Statistics 1-3 40.7% 264 Sum 1,782.0 4-6 36.4% 236 Average 3.1 7-10 12.6% 82 StdDev 2.1 over 10 10.3% 67 Max 7.0 Total 649 5 6. -

Mass Spectrometric Investigation of the Aging Processes of Ballpoint Ink for the Examination of Questioned Documents
MASS SPECTROMETRIC INVESTIGATION OF THE AGING PROCESSES OF BALLPOINT INK FOR THE EXAMINATION OF QUESTIONED DOCUMENTS INAUGURAL DISSERTATION For the degree of Doktor rer. nat. submitted to Justus-Liebig-University Giessen (Faculty of Biology and Chemistry) Céline Weyermann born on 13.03.1978 in La Chaux-de Fonds Switzerland. Giessen, 23th September 2005 Dean Prof. Dr. Jürgen Mayer 1st Referee Prof. Dr. Bernhard Spengler 2nd Referee Prof. Dr. Pierre Margot 3rd Referee Prof. Dr. Rudolf Geyer Zusammenfassung In den forensischen Wissenschaften ist die Bestimmung des Alters einer Kugelschreibereintragung (z.B. Kugelschreiberstrich) ein wichtiges Kriterium bei der Echtheitsprüfung von Dokumenten. Seit Beginn dieser Untersuchungen ist die Altersbestimmung eine wichtige und meist unbeantwortet gebliebene Frage geblieben. Die forensischen Wissenschaftler streiten sich über die Möglichkeit und die Validierung von Datierungsmethoden. Diese Kontroverse ist der Angangspunkt dieser Arbeit gewesen. Kugelschreiberpasten bestehen aus drei Hauptkomponenten: Lösungsmitteln (50%), Farbstoffen (25%) und Harzen (25%). Nach dem Auftragen der Pasten auf Papier findet mit der Zeit eine qualitative und quantitative Veränderung der Zusammensetzung der Kugelschreibereintragung statt. Während Farbstoffe ausbleichen, d.h. vor allem photochemisch abgebaut werden, wird das Alterungsverhalten der Lösungsmittel durch den Verdampfungs- und Diffusionsprozess charakterisiert. In der vorgestellten Arbeit, sind die Alterungsprozesse von Farbstoffen und Lösungsmitteln mittels -

Materialien – Supplies
Materialien – Supplies Schulranzen/Backpacks Schulranzen Midi Plus Schulranzen Midi Plus Schulranzen Midi Plus Schulranzen Midi Plus Motorrad/schoolbag Formula 1/schoolbag Geometrie/schoolbag Heart/schoolbag Midi Midi Plus Motorcycle Midi Plus Formula 1 Midi Plus Geometry Plus Heart $ 95.70 $ 95.70 $ 95.70 $ 95.70 Schulranzen Midi Plus Schulranzen Midi Plus Schulranzen Midi Plus Schulranzen Midi Plus Race Car/schoolbag Rainbow Dinosaurier/schoolbag Horse/schoolbag Midi Midi Plus Race Car Butterfly/schoolbag Midi Midi Plus Dinosaur Plus Horse Plus Rainbow Butterfly $ 95.70 $ 95.70 $ 95.70 $ 95.70 Schulranzen Midi Plus Die Schulranzen enthalten alle auch ein gefülltes Unicorn/schoolbag Schüleretui (16 Teile), ein Federmäppchen und Midi Plus Unicorn einen Sportbeutel. $ 95.70 The schoolbags all come with a filled pencil case (16 pcs.), a pencil pouch, and a sports bag. Federmäppchen/Pencil Cases a b a b d c d c e e a. Federmäppchen Motorcross/pencil case a. Federmäppchen Fußball/pencil case soccer Motorcross $5.65 $5.65 b. Federmäppchen Race Car/pencil case race car b. Federmäppchen Driven/pencil case driven $5.65 $5.65 c. Federmäppchen Shark/pencil case shark $5.65 c. Federmäppchen Kick it/pencil case kick it $5.65 d. Federmäppchen Space/pencil case space $5.65 d. Federmäppchen Dino/pencil case dino $5.65 e. Federmäppchen Truck/pencil case truck $5.65 e. Federmäppchen Jet/pencil case jet $5.65 a b a b c c d d a. Federmäppchen Flower Heart/pencil case flower a. Federmäppchen Horse/pencil case horse $5.65 heart $5.65 b. Federmäppchen Rainbow Butterfly/pencil case b. -

Publicizing the Mpowerment Project
mOdule Publicizing the Mpowerment Project Objectives To explain how to develop and implement a publicity plan that effectively reaches young gay/ bisexual men and promotes the Project and its activities. For the Mpowerment Project to be truly a communitywide HIV prevention program, as many young gay/bisexual men as possible must learn about the Project and its activities. Thus, effective publicity is an important Core Element to help the Project achieve its mission of reducing unsafe sex among young gay/bisexual men in the community. The most effective publicity campaigns: 1) use multiple strategies, 2) have clear goals, 3) reach all segments of the target audience, 4) are timely and ongoing, and 5) place a Publicity Coordinator or volunteer(s) in charge of implementation. In order to publicize the Project successfully, it is important to select the most appropriate messages to send out and decide how best to convey them. We encourage being as creative and thorough as possible in publicizing the Project. The best suggestions will likely come from the Core Group and other volunteers who are most familiar with their own community. What you’ll find in the Appendix to this module Figure 10.1 Sample Logo Contest Announcement. Figure 10.2 Sample Event Timeline. Figure 10.3 Publicity Plan. Figure 10.4 Sample Magazine Article written by a Project Coordinator in Dayton, Ohio. Figure 10.5 Sample Newspaper Ads. Mpowerment Project Logos from around the USA 2 Mpowerment Project Module 10 Publicizing the Mpowerment Project Goals of Publicity The goals -
Brands and Product Lines & Website Guide
plus Brands and Product Lines & Website Guide starts on page 56 Last Updated April 5, 2021 CONTACT [email protected] with questions, corrections, additions, updates Page 2 of 67 Product Guide Acetate Sheets Rolls Pads Grafix Jacquard Products / Rupert, Gibbon & Spider, Inc. MacPherson's SLS Arts Texas Art Supply/Art Supply Network Adhesives Alvin & Company Atlas Tape - Channeled Resources Grafix Grex Airbrush H. Schmincke & Co. GmbH & Co. KG HK Holbein, Inc Imagination International Jacquard Products / Rupert, Gibbon & Spider, Inc. Lineco MacPherson's Newell Brands SLS Arts Speedball Art Products Tombow Yasutomo Ziller's, LLC Advertising Art Materials Retailer Magazine Airbrush Equipment and Supplies Armadillo Art & Craft Grafix Grex Airbrush H. Schmincke & Co. GmbH & Co. KG HK Holbein, Inc Iwata-Medea Inc. Jacquard Products / Rupert, Gibbon & Spider, Inc. Page 3 of 67 MacPherson's SLS Arts SINOART Shanghai Co., Ltd Texas Art Supply/Art Supply Network Ziller's, LLC Albums Art and Photo Hahnemuhle USA Lineco MacPherson's SLS Arts Texas Art Supply/Art Supply Network Uchida of America Architectural Supplies ACCO UK. - ACCO Brands, Derwent Alumicolor Alvin & Company Grafix Jack Richeson & CO Inc. MacPherson's SINOART Shanghai Co., Ltd SLS Arts STAEDTLER-Mars Limited Studio Designs Texas Art Supply/Art Supply Network Tombow Artboard MultiMedia Aitoh Co. (WCG Group LLC, dba Aitoh Co.) Alvin & Company Crescent Cardboard, LLC Fredrix Canvas Grafix Heinz Jordan and Company Limited Hilltop Paper LLC Jack Richeson & CO Inc. Lineco Ranger Industries SINOART Shanghai Co., Ltd SLS Arts Texas Art Supply/Art Supply Network Block Printing ABIG GERMANY Armadillo Art & Craft Cranfield Colours Page 4 of 67 Educational Art and Craft Supplies Edward C Lyons Co. -
The Vine Volume 27 Issue 05 October AS LV / 2020
The Vine Volume 27 Issue 05 October AS LV / 2020 Regnum King & Queen of Lochac Theuderic and Engelin [email protected] Baron Agostino & Baroness Elizabeth [email protected] Champion of the Sword Lord Dino de Malta Champion of the Bow Emma of Aneala Champion of the Rapier Lord Zaven Zeitountsi Champion of Arts & Sciences Branwen of Werchesvorde Bard of Aneala Lady Gwyneth ferch Aeddan Seneschal Reeve Konrad Hildebrandt Leonie de Grey [email protected] [email protected] Arts & Sciences Constable Frances Affrica Ray Ula [email protected] [email protected] Marshal Chronicler Honourable Lord Lokki Rekkr Kilic [email protected] [email protected] Herald Blackwing Pursuivant List Keeper Gwyneth ferch Aeddan Isabel de Annesley [email protected] [email protected] Chatelaine Rapier Marshal Zaven Zeitountsi Dameon Greybeard [email protected] [email protected] Webminister Captain of Archers Julian Greenwood Branwen of Werschesvorde [email protected] [email protected] Youth Officer Pantero Pantera di Valembrosa [email protected] Baronial Missive Greetings to the Populace of Aneala, Thank you for your patience with us last month when you did not receive our Baronial Missive. It is neither the fault of the Chronicler nor the postal system – we were simply preoccupied preparing for Anealan Baronial Championship! Since last we wrote, we have had the great pleasure of attending two events “in person” rather than on Discord. The first was the Baroness’s Fighter Auction. -

Hate Violence Against Lesbian, Gay, Bisexual, Transgender, and HIV
Hate Violence A Report from Against Lesbian, Gay, the National Bisexual, Transgender, Coalition of Queer, and HIV- affected Anti-Violence Communities Programs In the United States in 2011 Hate Violence Against Lesbian, Gay, Bisexual, Transgender, Queer and HIV-affected Communities in the U.S. in 2011 NCAVP The National Coalition of Anti-Violence Programs authored this report. A program of the New York City Anti-Violence Project 240 W. 35th St., Suite 200 New York, NY 10001 www.ncavp.org Writing Ejeris Dixon, New York City Anti-Violence Project Chai Jindasurat, New York City Anti-Violence Project Victor Tobar, Consultant Data Collection and Data Analysis: Nahima Ahmed, Strength in Numbers Consulting Group Tasha Amezcua, New York City Anti-Violence Project Somjen Frazer, Strength in Numbers Consulting Group Jonathan Rodkin, Strength in Numbers Consulting Group Justin Rosado, New York City Anti-Violence Project Layout & Data Design Joyce Choi Li, New York City Anti-Violence Project Kate Traub, New York City Anti-Violence Project Additional Writing and Data Michelle Bramblett, Southern Poverty Law Center Kelly Clark, Gay Alliance of the Genesee Valley Kelcie Cooke, LMSW, Violence Recovery Program, Fenway Community Health Chris Cozad, Buckeye Region Anti-Violence Organization Aaron Eckhardt, MSW, Buckeye Region Anti-Violence Organization Ajené Farrar, New York City Anti-Violence Project Jake Finney, L.A. Gay & Lesbian Center Lisa Gilmore, LMHC, Center on Halstead Anti-Violence Project Sally Huffer, Montrose Counseling Center Elke Kennedy, -

Curriculum Vitae Andrew S. Walters Department of Psychological
Curriculum Vitae Andrew S. Walters Department of Psychological Sciences College of Social and Behavioral Sciences Northern Arizona University Flagstaff, Arizona 86011-5106 (928) 523.3206 E-Mail [email protected] Education MPH Epidemiology, University of California at Berkeley, May 1997 (Specialty Area: Multi-Cultural Health) Ph.D. Psychology, University of Georgia, August 1992 (Major Areas: Developmental & Health Psychology; Sexual Science) Gerontology Certificate, University of Georgia, March 1992 M.A. The Ohio State University, June 1988 B.S. The Ohio State University, June 1986 Employment 2013 - Present Professor, Department of Psychological Sciences 2014 - Present President’s Distinguished Teaching Fellow, Northern Arizona University 2008 - 2013 Associate Professor, Department of Psychology, Northern Arizona University 2008 - Present Mentor affiliated with the Research in Undergraduate Experience Program; National Science Foundation 2005 - 2008 Assistant Professor, Department of Psychology, Northern Arizona University 2005 - 2008 Program Evaluator, The WHEEL Council, Phoenix, AZ 2007 - Present Faculty Program Affiliate, Women’s and Gender Studies Program, Northern Arizona University 2003 - 2005 Associate Professor, Department of Psychology, Hobart & William Smith Colleges Faculty Appointments to Interdisciplinary Programs: Child Advocacy; Media and Society; Men’s Studies 1998 - 2003 Assistant Professor, Department of Psychology; Program in Men’s Studies Hobart and William Smith Colleges 2004 - 2007 [Volunteer] Consultant, The Central -

Art Hazards List
ART AND CRAFT MATERIALS THAT CANNOT BE PURCHASED FOR USE IN KINDERGARTEN THROUGH 6TH GRADE Office of Environmental Health Hazard Assessment – California Environmental Protection Agency September 2016 California Education Code Section 32064 prohibits schools from purchasing art or craft materials containing a toxic substance for use by students in kindergarten and grades 1-6 (K- 6). The law also requires the Office of Environmental Health Hazard Assessment (OEHHA) to develop a list of products that schools cannot purchase for use by students in K-6. This list (attached) is intended to assist schools, school districts, and governing authorities of private schools in complying with the purchasing requirements. Purchasers must ensure that all art and craft materials to be used by students bear a statement of conformity to ASTM D-4236 (Standard Practice for Labeling Art Materials for Chronic Health Hazards), as required by federal law. Items to be used by students in K-6 must not bear acute or chronic health hazard labels. Although not required by law, avoiding art materials that bear acute or chronic health hazard labels when purchasing for grades 7-12 is a good precautionary measure. Schools are encouraged to inventory existing art and craft supplies and remove materials bearing health hazard labels from K-6th grade classrooms. For further information, please see Art and Craft Materials in Schools: Guidelines for Purchasing and Safe Use, accompanying this list or available online (see below). OEHHA compiled the attached list based on product evaluations conducted by other entities1 according to federal requirements. Other art and craft materials that can be listed are products recalled in the past five years2 (no such products are listed at this time), as well as those brought to OEHHA’s attention as bearing health hazard labels. -
Spring 2011 Supplying Calligraphers, Lettering Artists, Illuminators
spring 2011 Supplying calligraphers, lettering artists, illuminators, bookbinders and papercraft enthusiasts worldwide with books, tools, and materials since 1981. 61 5 64 50 61 61 ORDER NOW! toll free: 800-369-9598 v web: www.JohnNealBooks.com Julie Eastman. B&L 8.2 “...an informative, engaging, Bill Waddington. B&L 8.2 and valued resource.” Need something new to inspire you? –Ed Hutchins Subscribe to Bound & Lettered and have each issue – filled with practical information on artists’ books, bookbinding, calligraphy and papercraft – delivered to your mailbox. Bound & Lettered features: how-to articles with helpful step-by-step instructions and illustrations, artist galleries featuring the works of accomplished calligraphers & book artists, useful articles on tools & materials, and book & exhibit reviews. You will find each issue filled with wonderful ideas and projects. Subscribe today! Annie Cicale. B&L 8.3 Every issue of Bound & Lettered has articles full of practical information for calligraphers, bookbinders and book artists. Fran Watson. B&L 8.3 Founded by Shereen LaPlantz, Bound & Lettered is a quarterly magazine of calligraphy, bookbinding and papercraft. Published by John Neal, Bookseller. Now with 18 color pages! Subscription prices: USA Canada Others Four issues (1 year) $26 $34 USD $40 USD Eight issues (2 years) $47 $63 USD $75 USD 12 issues (3 years) $63 $87 USD $105 USD mail to: Bound & Lettered, 1833 Spring Garden St., First Floor, Sue Bleiwess. B&L 8.2 Greensboro, NC 27403 b SUBSCRIBE ONLINE AT WWW .JOHNNEALBOOKS .COM B3310. Alphabeasties and Other Amazing Types by Sharon Werner and Sarah Forss. 2009. 56pp. 9"x11.5".