Program Monthly Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contact N°177-178 About This Issue of Contact for Health
1 Contact n°177-178 About this issue of Contact for Health: Our lead topic is AIDS and malaria and we have From Uganda, Dr Pepper, a Southern Baptist Conven- received news from East Africa: Kenya, Tanzania, and tion Missionary, physician and head of the HIV clinic, and Uganda; from Southern Africa and West Africa. internal medicine at the government teaching hospital MUTH, reports his practice of Biblical holistic care and The Ecumenical HIV/AIDS Initiative in Africa was his use of latest technologies: syringes where the launched in Nairobi. p.14 & 41 needle retracts after use. p.15 The Ecumenical Advocacy Alliance will be active in the The Safe Health Care and HIV coalition is petitioning 2004 IAS AIDS Conference in Bangkok. p.4 the 2004 World Health Assembly and proposing an amendment to insure total safety. p.42 “Africa could be depopulated by AIDS to an extent Coming together to confront AIDS, is the message of the not seen since Slavery!”, Reverend Dr. Samuel Kobia, The Inter Religious Council of Uganda received from General Secretary of the WCC, told Contact : “AIDS is Rev. Sam Lawrence Ruteikara, AIDS Director. p.15 the enemy”. p.5 The Church of the Province of West Africa, Anglican Special report TANZANIA (p.7-13) Provincial Health Service in Accra, Ghana, report that “In faith, we are breaking ground slowly”. p.16 “FAIR TRADE”, Tanzania’s Deputy Health Minister Hussein A. Mwinyi tells the world, “would best assist From the South African Catholic Bishops’ Conference Africa in meeting the challenge of HIV AIDS”. p.12 AIDS Office comes a call and a commitment for treat- ment. -

2019 Tanzania in Figures
2019 Tanzania in Figures The United Republic of Tanzania 2019 TANZANIA IN FIGURES National Bureau of Statistics Dodoma June 2020 H. E. Dr. John Pombe Joseph Magufuli President of the United Republic of Tanzania “Statistics are very vital in the development of any country particularly when they are of good quality since they enable government to understand the needs of its people, set goals and formulate development programmes and monitor their implementation” H.E. Dr. John Pombe Joseph Magufuli the President of the United Republic of Tanzania at the foundation stone-laying ceremony for the new NBS offices in Dodoma December, 2017. What is the importance of statistics in your daily life? “Statistical information is very important as it helps a person to do things in an organizational way with greater precision unlike when one does not have. In my business, for example, statistics help me know where I can get raw materials, get to know the number of my customers and help me prepare products accordingly. Indeed, the numbers show the trend of my business which allows me to predict the future. My customers are both locals and foreigners who yearly visit the region. In June every year, I gather information from various institutions which receive foreign visitors here in Dodoma. With estimated number of visitors in hand, it gives me ample time to prepare products for my clients’ satisfaction. In terms of my daily life, Statistics help me in understanding my daily household needs hence make proper expenditures.” Mr. Kulwa James Zimba, Artist, Sixth street Dodoma.”. What is the importance of statistics in your daily life? “Statistical Data is useful for development at family as well as national level because without statistics one cannot plan and implement development plans properly. -

Community Concerns of Orphans and Development Association (Cocoda) P
COMMUNITY CONCERNS OF ORPHANS AND DEVELOPMENT ASSOCIATION (COCODA) P. O. BOX 712, NJOMBE - CHAUNGINGI STREET ALONG SONGEA ROAD, OPPOSITE TANESCO REGIONAL OFFICE Email: [email protected] Website: www.cocoda.or.tz COCODA 2019 ANNUAL REPORT COMMUNITY CONCERN OF ORPHANS AND DEVELOPMENT ASSOCIATION REPORTING PERIOD: 1 JANUARY – 31 DECEMBER 2019 Projects Implemented Councils • SAUTI Project Njombe Region councils: Njombe Town Council • USAID KIZAZI KIPYA Project • • Njombe District Council • USAID Tulonge Afya • Makambako Town Council • Makete District Council • Wanging’ombe District Council • Ludewa District Council Prime Recipients Implementing Partners • DELOITTE CONSULTANCY LTD • LGAs JHPIEGO • • Health facilities • PACT TANZANIA • FHI360 Programme/Project Budget/Year Programme Duration • SAUTI 182,970,583 5 Years • USAID KIZAZI KIPYA 297,158,227 5 Years • USAID TULONGE AFYA 159,376,560 5 Years TOTAL: 639,505,370 Report Submitted By o Name: Mary Kahemele o Title: Executive Director o Organization: COCODA o Email address: [email protected] o Phone No: 0754 071 288 1 Table of Contents List of Acronyms / Abbreviations ................................................................................ 3 Executive Summary ................................................................................................... 4 PROJECT IMPLEMENTATION ..................................................................................... 5 I. SAUTI PROJECT ................................................................................................. -

Basic Demographic and Socio-Economic Profile
The United Republic of Tanzania Basic Demographic and Socio-Economic Profile National Bureau of Statistics Ministry of Finance Dar es Salaam and Office of Chief Government Statistician Ministry of State, President ‟s Office, State House and Good Governance Zanzibar April, 2014 UNITED REPUBLIC OF TANZANIA, ADMINISTRATIVE BOUNDARIES Basic Demographic and Socio-Economic Profile Foreword The 2012 Population and Housing Census (PHC) for the United Republic of Tanzania was carried out on the 26th August, 2012. This was the fifth Census after the Union of Tanganyika and Zanzibar in 1964. Other censuses were carried out in 1967, 1978, 1988 and 2002. The 2012 PHC, like previous censuses, will contribute to the improvement of quality of life of Tanzanians through the provision of current and reliable data for policy formulation, development planning and service delivery as well as for monitoring and evaluating national and international development frameworks. The 2012 PHC is unique as the collected information will be used in monitoring and evaluating the Development Vision 2025 for Tanzania Mainland and Zanzibar Development Vision 2020, Five Year Development Plan 2011/12–2015/16, National Strategy for Growth and Reduction of Poverty (NSGRP) commonly known as MKUKUTA and Zanzibar Strategy for Growth and Reduction of Poverty (ZSGRP) commonly known as MKUZA. The Census will also provide information for the evaluation of the Millennium Development Goals (MDGs) in 2015. The Poverty Monitoring Master Plan, which is the monitoring tool for NSGRP and ZSGRP, mapped out core indicators for poverty monitoring against the sequence of surveys, with the 2012 PHC being one of them. Several of these core indicators for poverty monitoring are measured directly from the 2012 PHC. -
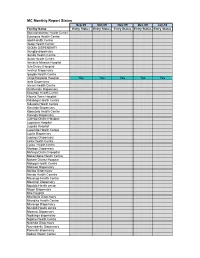
MC Monthly Report Status
MC Monthly Report Status Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Facility Name Entry Status Entry Status Entry Status Entry Status Entry Status Bomalang'ombe Health Centre Bulongwa Health Centre Idodi Health Centre Ifwagi Health Center IGOMA DISPENSARY Ihungilo dispensary Ikonda Health Centre Ikuwo Health Centre Ilembula Mission Hospital Ilula District Hospital Imalinyi Dispensary Ipogolo Health Centre Iringa Regional Hospital Yes Yes Yes Yes Yes Isele Dispensary Ismani Health Centre Itulahumba Dispensary Kasanga Health Centre Kibena Town Hospital Kidabaga Health Centre Kidugala Health Centre Kimande Dispensary Kiponzelo Health Centre Kisanga Dispensary Ludewa District Hospital Lugalawa Hospital Lugoda Hospital Lupembe Health Centre Lupila Dispensary Lupingu Dispensary Lwila Health Centre Lyasa Health centre Madege Dispensary Mafinga District Hospital Makambako Health Centre Makete District Hospital Makoga Health Centre Makowo Dispensary Maliwa Dispensary Manda Health Ceantre Mavanga Health Centre Mawengi Dispensary Mgololo Health center Migori Dispensary Milo Hospital Mtambula Dispensary Mtandika Health Centre Mtwango Dispensary Mundidi Health centre Mwatasi Dispensary Ngalanga dispensary Ngome Health Centre Nyombo Dispensary Nyumbanitu Dispensary Pomerini dispensary Sadani Health Center Saint Lukes Dispensary Tanangozi Dispensary TANWAT Hospital Tosamaganga District Hospital Ugwachanya Dispensary Ujuni Dispensary Ukalawa dispensary Uliwa Dispensary Usokami HC Key: Not Applicable Available Not Available Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10 -
SAGCOT) Public Disclosure Authorized Investment Project
THE UNITED REPUBLIC OF TANZANIA PRIME MINISTER’S OFFICE Public Disclosure Authorized Southern Agricultural Growth Corridor of Tanzania (SAGCOT) Public Disclosure Authorized Investment Project SRATEGIC REGIONAL ENVIRONMENTAL Public Disclosure Authorized AND SOCIAL ASSESSMENT (SRESA) This SRESA report was prepared for the Government of Tanzania by Environmental Resources Management Limited (ERM) under a contract as part of SAGCOT preparatory activities Public Disclosure Authorized DECEMBER 2013 CONTENTS EXECUTIVE SUMMARY I 1 INTRODUCTION 1 1.1 BACKGROUND 1 1.2 PROGRAMMEOVERVIEW 1 1.3 STUDY OBJECTIVE 2 1.4 PURPOSE OF THIS REPORT 3 1.5 APPROACH AND METHODOLOGY 3 1.5.1 Overview 3 1.5.2 Screening 4 1.5.3 Scoping 4 1.5.4 Baseline Description 4 1.5.5 Scenario Development 4 1.5.6 Impact Assessment 5 1.5.7 Development of Mitigation Measures 5 1.5.8 Consultation 6 1.5.9 Constraints and Limitations 6 1.6 REPORT LAYOUT 6 2 THE SOUTHERN AGRICULTURAL GROWTH CORRIDOR OF TANZANIA 8 2.1 THE SAGCOT PROGRAMME 8 2.1.1 The SAGCOT Concept 8 2.1.2 SAGCOT Organisation 11 2.2 PROPOSED WORLD BANK SUPPORTED SAGCOT INVESTMENT PROJECT 14 2.2.1 General 14 2.2.2 Catalytic Fund 15 2.2.3 Support Institutions 16 3 THE AGRICULTURE SECTOR IN TANZANIA 20 3.1 INTRODUCTION 20 3.2 AGRICULTURE AND THE TANZANIAN ECONOMY 20 3.2.1 Overview 20 3.2.2 Land Use 25 3.3 PRIORITIES FOR DEVELOPMENT OF THE AGRICULTURE SECTOR 25 3.3.1 Current Initiatives for Agricultural Development 25 3.3.2 Rationale for SAGCOT Programme 29 3.3.3 District Level Agricultural Planning 30 3.4 FINANCING POLICIES -
Children Left Behind Barriers to Testing And
WORKING PAPER WORKING WORKING PAPER WORKING The Children Left Behind Barriers to Identifying and Enrolling Children with HIV into Care and Treatment Programs The Children Left Behind Jackson Mbogela AlfredBarriers Kyando to Testing and Enrolling Riziki Mahenge Children in HIV Care and Treatment in Njombe Region, Tanzania July 2017 May 2018 Publication ID Code Goes Here PAPER WORKING PAPER WORKING The Children Left Behind Barriers to Testing and Enrolling Children in HIV Care and Treatment in Njombe Region, Tanzania Jackson Mbogela, MPH Alfred I. Kyando, MSc Riziki Mahenge, LLB May 2018 This research has been supported by the President’s MEASURE Evaluation–Tanzania Emergency Plan for AIDS Relief (PEPFAR) through the TCRS Building, United States Agency for International Development (USAID) under the terms of MEASURE Evaluation-Tanzania 1st Floor, Plot No. 436, Mwai Kibaki associate award AID-621-LA-14-00001. MEASURE Road, Mikocheni B. Evaluation–Tanzania is implemented by the Carolina Population Center at the University of North Carolina at Dar es Salaam, TZ Chapel Hill, in partnership with ICF International; John Snow, Inc.; Management Sciences for Health; Palladium; +255 22 277 3023 and Tulane University. Views expressed are not necessarily www.measureevaluation.org/tanzania those of PEPFAR, USAID or the United States government. WP-18-206 ACKNOWLEDGEMENTS The Pima Uishi Kwa Matumaini (PIUMA) research team would like to thank the United Stated Agency for International Development (USAID), through the MEASURE Evaluation–Tanzania project, which enabled this study to be conducted. We are in debt to the acting Regional Medical Officer for Njombe region, Eusebi Kessy, MD, for coordinating with Town Council Medical Doctor and District Medical Officer and to allow us to conduct this study in Njombe Town Council and Wanging’ombe District Council. -

Addressing Witchcraft in Tanzania: Case Study of a Promising Approach Credit for Cover Photo: UNICEF/UNI197925/Schermbrucker
Addressing witchcraft in Tanzania: case study of a promising approach Credit for cover photo: UNICEF/UNI197925/Schermbrucker Acknowledgements The UNICEF Eastern and Southern African Regional Office (ESARO) commissioned Child Frontiers to develop a compendium of promising practices on ending harmful practices and violence against children across the region. This documentation was written by Emma de Vise-Lewis of Child Frontiers with essential contributions from UNICEF Tanzania Country Office staff, and government, NGOs and other partners. Thanks also go to Jean Francois Basse and Mona Aika of UNICEF ESARO for their leadership and support throughout the process of developing the brief. The publication was designed by hopeworks. April 2021 © UNICEF/UNI91272/Noorani © Purpose of the case study Introduction The purpose of this case study is to highlight a Violence against children includes ‘all forms of promising programme, service or approach that physical or mental violence, injury and abuse, is supported by the UNICEF country office and neglect or negligent treatment, maltreatment that seeks to address issues of violence against or exploitation, including sexual abuse’.1 children in Tanzania. It provides an outline of According to the Global End Violence Against the work that is being done, and an analysis of Children campaign, one billion girls and boys its successes and challenges. The information suffer from violence every year, including presented is based on a documentary review physical, emotional and sexual violence.2 and interviews -

United Republic of Tanzania
United Republic of Tanzania The United Republic of Tanzania Jointly prepared by Ministry of Finance and Planning, National Bureau of Statistics and Njombe Regional Secretariat Njombe Region National Bureau of Statistics Njombe Dodoma November, 2020 Njombe Region Socio-Economic Profile, 2018 Foreword The goals of Tanzania’s Development Vision 2025 are in line with United Nation’s Sustainable Development Goals (SDGs) and are pursued through the National Strategy for Growth and Reduction of Poverty (NSGRP) or MKUKUTA II. The major goals are to achieve a high-quality livelihood for the people, attain good governance through the rule of law and develop a strong and competitive economy. To monitor the progress in achieving these goals, there is need for timely, accurate data and information at all levels. Problems especially in rural areas are many and demanding. Social and economic services require sustainable improvement. The high primary school enrolment rates recently attained have to be maintained and so is the policy of making sure that all pupils who passed Primary School Leaving Examination must join form one. The Nutrition situation is still precarious; infant and maternal mortality rates continue to be high and unemployment triggers mass migration of youths from rural areas to the already overcrowded urban centres. Added to the above problems, is the menace posed by HIV/AIDS, the prevalence of which hinders efforts to advance into the 21st century of science and technology. The pandemic has been quite severe among the economically active population leaving in its wake an increasing number of orphans, broken families and much suffering. AIDS together with environmental deterioration are problems which cannot be ignored. -

United Republic of Tanzania President’S Office Regional Administration and Local Government
UNITED REPUBLIC OF TANZANIA PRESIDENT’S OFFICE REGIONAL ADMINISTRATION AND LOCAL GOVERNMENT WANGING’OMBE DISTRICT COUNCIL COUNCIL STRATEGIC PLAN FOR THE YEAR 2015/16 – 2019/20 Prepared by, District Executive Director, Wanging’ombe District Council, P.O.Box 64, WANGING’OMBE – NJOMBE REGION EXECUTIVE SUMMARY Wanging’ombe is a relatively newly established District council which was officially registered on 18, March, 2013. Like any other Council in Tanzania, Wanging’ombe district council operates with statutory powers and in line with legislation and regulations enacted by the parliament under the Local Government Act No. 7 of 1982. The council is given wide-ranging functions include: To maintain and facilitate the maintenance of peace, order and good governance in their area of jurisdiction, To promote the social welfare and economic well-being of all persons within its area of jurisdiction; Subject to the national policy and plans for the rural and urban development, to further the social and economic development of its area of jurisdiction. In fulfilling the Wanging’ombe district council’s functions, the district requires a comprehensive decision making to trigger sustainable local economic development through strategic planning at local level. This strategic plan will assist the District council to improve performance, to create more relevant institutional structures, to increase levels of institutional, departmental, and individual accountability; to improve transparency and communication between management, employees and stakeholders and to establish priorities for efficient and effective use of resource. This strategic plan document is divided into Five Chapters, where first chapter provides background information and strategic planning process, second chapter provides situational analysis of the district where a through diagnosis of the internal environment in 19 service areas was conducted, as well as the external environment which the district is operating under in executing this strategic plan. -

An End of Project Review for the Agro-Dealer Development Project Funded by Agra in Tanzania
AN END OF PROJECT REVIEW FOR THE AGRO-DEALER DEVELOPMENT PROJECT FUNDED BY AGRA IN TANZANIA FINAL REPORT Prepared by: Kobe Konsult Ltd JUED Business Centre, 34 Garden Road, Mikocheni A, P.O. Box 32187, Dar es Salaam Phone: +255 22 277 4436 / 0754 300 767 Fax: +255 22 277 4426 Email: [email protected] August 2012 TABLE OF CONTENTS LIST OF FIGURES .................................................................................................................. iv LIST OF TABLES ...................................................................................................................... v ACKNOWLEDGEMENTS ..................................................................................................... vii Executive Summary ................................................................................................................ viii 1.0 INTRODUCTION................................................................................................................. 1 1.1 Background and Rationale ....................................................................................... 1 1.2 Evaluation Objectives and Scope ............................................................................. 1 1.2.1 Specific objectives ........................................................................................................ 2 2.0 METHODOLOGY AND APPROACH ............................................................................. 2 2.1 Review of Secondary Data ....................................................................................... -
Accelerating Mini-Grid Deployment in Sub-Saharan Africa: Lessons from Tanzania I Design and Layout By: Jenna Park [email protected] TABLE of CONTENTS
Public Disclosure Authorized Public Disclosure Authorized ACCELERATING MINI- GRID DEPLOYMENT IN SUB-SAHARAN AFRICA Lessons from Tanzania Public Disclosure Authorized LILY ODARNO, ESTOMIH SAWE, MARY SWAI, MANENO J.J. KATYEGA AND ALLISON LEE Public Disclosure Authorized WRI.ORG Accelerating Mini-Grid Deployment in Sub-Saharan Africa: Lessons from Tanzania i Design and layout by: Jenna Park [email protected] TABLE OF CONTENTS 1 Foreword 3 Preface 5 Executive Summary 13 Introduction 19 Overview of Mini-Grids in Tanzania 39 The Institutional, Policy, and Regulatory Framework for Mini-Grids in Tanzania 53 Mini-Grid Ownership and Operational Models 65 Planning and Securing Financing for Mini-Grid Projects 79 How Are Mini-Grids Contributing to Rural Development? 83 Conclusions and Recommendations 86 Appendix A: People Interviewed for This Report 88 Appendix B: Small Power Producers That Signed Small Power Purchase Agreements and Submitted Letters of Intent 90 Appendix C: Policies, Strategies, Acts, Regulations, Technical Standards, and Programs, Plans, and Projects on Mini-Grids 94 Abbreviations 95 Glossary 96 Bibliography 99 Endnotes Accelerating Mini-Grid Deployment in Sub-Saharan Africa: Lessons from Tanzania iii iv WRI.org FOREWORD More than half of the 1 billion people in the world In Tanzania, a slow environmental clearance without electricity live in Sub-Saharan Africa, procedure delayed the deployment of some mini- and rapid population growth is projected to grids despite a streamlined regulatory process. outpace electric grid expansion. For communities across the region, a consistent and affordable Invest in both qualitative and quantitative ▪ supply of electricity can open new possibilities for assessments of the development impacts socioeconomic progress.