Highland Primary Care Nhs Trust
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Full Set of Board Papers
Assynt House Beechwood Park Inverness, IV2 3BW Telephone: 01463 717123 Fax: 01463 235189 Textphone users can contact us via Date of Issue: Typetalk: Tel 0800 959598 23 November 2012 www.nhshighland.scot.nhs.uk HIGHLAND NHS BOARD MEETING OF BOARD Tuesday 4 December 2012 at 8.30 am Board Room, Assynt House, Beechwood Park, Inverness AGENDA 1 Apologies 1.1 Declarations of Interest – Members are asked to consider whether they have an interest to declare in relation to any item on the agenda for this meeting. Any Member making a declaration of interest should indicate whether it is a financial or non-financial interest and include some information on the nature of the interest. Advice may be sought from the Board Secretary’s Office prior to the meeting taking place. 2 Minutes of Meetings of 2 October and 6 November 2012 and Action Plan (attached) (PP 1 – 24) The Board is asked to approve the Minute. 2.1 Matters Arising 3 PART 1 – REPORTS BY GOVERNANCE COMMITTEES 3.1 Argyll & Bute CHP Committee – Draft Minute of Meeting held on 31 October 2012 (attached) (PP 25 – 40) 3.2 Highland Health & Social Care Governance Committee Assurance Report of 1 November 2012 (attached) (PP 41 – 54) 3.3 Highland Health & Social Care Governance Committee – Terms of Reference for approval by the Board (attached) (PP 55 – 58) 3.4 Clinical Governance Committee – Draft Minute of Meeting of 13 November 2012 (attached) (PP 59 – 68) 3.5 Improvement Committee Assurance Report of 5 November 2012 and Balanced Scorecard (attached) (PP 69 – 80) 3.6 Area Clinical Forum – Draft Minute of Meeting held on 27 September 2012 (attached) (PP 81 – 88) 3.7 Asset Management Group – Draft Minutes of Meetings of 18 September and 23 October 2012 (attached) (PP 89 – 96) 3.8 Pharmacy Practices Committee (a) Minute of Meeting of 12 September 2012 – Gaelpharm Limited (attached) (PP 97 – 118) (b) Minute of Meeting of 30 October 2012 – Mitchells Chemist Limited (attached) (PP 119 – 134) The Board is asked to: (a) Note the Minutes. -

Gàidhlig (Scottish Gaelic) Local Studies Vol
Gàidhlig (Scottish Gaelic) Local Studies Vol. 22 : Cataibh an Ear & Gallaibh Gàidhlig (Scottish Gaelic) Local Studies 1 Vol. 22: Cataibh an Ear & Gallaibh (East Sutherland & Caithness) Author: Kurt C. Duwe 2nd Edition January, 2012 Executive Summary This publication is part of a series dealing with local communities which were predominantly Gaelic- speaking at the end of the 19 th century. Based mainly (but not exclusively) on local population census information the reports strive to examine the state of the language through the ages from 1881 until to- day. The most relevant information is gathered comprehensively for the smallest geographical unit pos- sible and provided area by area – a very useful reference for people with interest in their own communi- ty. Furthermore the impact of recent developments in education (namely teaching in Gaelic medium and Gaelic as a second language) is analysed for primary school catchments. Gaelic once was the dominant means of conversation in East Sutherland and the western districts of Caithness. Since the end of the 19 th century the language was on a relentless decline caused both by offi- cial ignorance and the low self-confidence of its speakers. A century later Gaelic is only spoken by a very tiny minority of inhabitants, most of them born well before the Second World War. Signs for the future still look not promising. Gaelic is still being sidelined officially in the whole area. Local council- lors even object to bilingual road-signs. Educational provision is either derisory or non-existent. Only constant parental pressure has achieved the introduction of Gaelic medium provision in Thurso and Bonar Bridge. -
Draft CCC Minutes SEPT 2016
Draft Minutes for approval CREICH COMMUNITY COUNCIL Minutes of meeting held on Tuesday 20th September 2016 at 7.30pm in Rosehall Village Hall Present: Pete Campbell, Chair, (PC), Ron Boothroyd, Vice Chair (RB), Russell Taylor, Treasurer, Also present: Michael Baird (MB), Norman Vincent (NV), Jennifer Munro (JM) Police Scotland: PC Dave Thompson (DT) and PC Chris Wylie (CW) Apologies: Russell Smith (RS), John White (JW), Norman MacDonald (NM), Brian Coghill (BC) and Highland Councillor George Farlow (GF) Secretary: Mary Goulder (MG) Item 1. Welcome/Apologies (as above)/Police report (See below). Pete Campbell welcomed everyone but recorded that the meeting was not quorate due to the apologies received from elected members. It was agreed to conduct the meeting to the best ability of those members present and that no decisions could be taken without the opinions of the others. An email will be circulated after the meeting with any recommendations made to seek approval/rejection as appropriate. MG Action. Item 2. Minutes of August meeting/matters arising (if not on agenda). The minutes of the August meeting were approved, as a true and accurate record; proposed: Russell Taylor, seconded: Ron Boothroyd. (1) Invitation to THC Roads Manager and Police Scotland Area Commander. This is proposed for the October CC meeting (18th) and invitations will be issued. MG Action. From the floor NV asked to register is complaint that since he raised the traffic issues in Bonar at the June meeting, to date no action has been taken by the CC. Chair advised that had been agreed at the last meeting that the North Area Commander Police Scotland and the Head of Roads at Highland Council would be invited to attend the October meeting. -
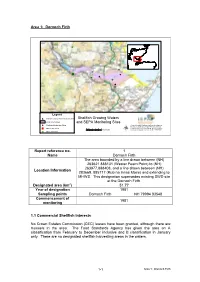
Area 1: Dornoch Firth Shellfish Growing Waters and SEPA Monitoring Sites Report Reference No. 1 Name Dornoch Firth Location
Area 1: Dornoch Firth ^_ ^_ ^_ ^_ ^_ ^_^_ ! ^_ # ^_ # ^_ ^_ Legend # Shellfish Growing Waters Monitoring Sites Shellfish Growing Waters Shellfish Growing Waters and SEPA Monitoring Sites ! Shellfish Production Sites (c) 2004 Scottish Environment Protection Agency. Includes material based upon Ordnance Survey " Marine Fish Farms 00.51 2 3 4 5 mapping with permission of H.M. Stationery Office. Kilometers (c) Crown Copyright. Licence number 100020538. ^_ Major Discharges µ Report reference no. 1 Name Dornoch Firth The area bounded by a line drawn between (NH) 263621 888131 (Wester Fearn Point) to (NH) 263977,888408, and a line drawn between (NH) Location Information 283669, 885717 (Rub na Innse Moire) and extending to MHWS. This designation supersedes existing SWD site at the Dornoch Firth. Designated area (km2) 51.77 Year of designation 1981 Sampling points Dornoch Firth NH 79994 83548 Commencement of 1981 monitoring 1.1 Commercial Shellfish Interests No Crown Estates Commission (CEC) leases have been granted, although there are mussels in the area. The Food Standards Agency has given the area an A classification from February to December inclusive and B classification in January only. There are no designated shellfish harvesting areas in the waters. 1- 1 Area 1: Dornoch Firth 1.2 Bathymetric Information This shellfish water encompasses almost the entire area of the Dornoch Firth. The area is some 22 km long by a maximum of 5.5 km wide. The maximum charted depth (at LAT) is <10 m. Approximately half of the area is <0 m chart depth, ie intertidal area exposed at low tide. -

Ardgay District
ARDGAY & DISTRICT Community Council newsletter Price: £1.00 ISSN (Online) 2514-8400 = Issue No. 36 = SUMMER 2017 = New Hub opening this summer The new Kyle of Sutherland Hub is almost com- plete. Here is a taste of what is to come. THE TEAM HAVE BEEN appointed Ann Renouf, Café Supervisor, and we would like to welcome Emma Mackay, General As- Adele Newlands, Hub Manag- sistant, and Clark Goodison, er; Vicky Karl, Café Manager; Cleaner. (Continue on page 9) The bright red Hub, as seen from Tulloch. THE CURRENT CC WAS FORMED IN FEBRUARy 2016 Achievements and challenges of your Community Council from June 2016 WE REPRODUCE Betty the issues discussed at Wright’s annual report our meetings? Which from our AGM. Our will feature in next year’s Chairperson thanks all agendas? We have cre- who have given freely of ated a map highlighting their time to CC business. the work of your CC in (Pages 4-6) What were 2016-2017. (Page 5). Opening of the Falls of Shin Visitor Attraction. The work of the Kyle of Plans to supply access to Sutherland Development Trust Superfast broadband to all Helen Houston reports on current and future projects What to do if you have been ‘left out’ Page 8 of the Trust (Pages 14-15) Beginning of the works on the Business Barn & Art Shed in Ardgay (Page 11) Know more about East Sutherland Energy Advice Service (Page 17) George Farlow’s farewell message Page 7 All you need Volunteering a to know opportunities 32 pages featuring Letters to the Editor, about horses in your Opening times, on the road area Telephone guide, Bus & Train timetable, Page 10 Page 20 Crosswords, Sudoku.. -

2014 2 Friendly Companion January 2014
TThhee Friendly Companion Friendly Companion “The L ORD hath made all things for Himself.” (Proverbs 16. 4.) January 2014 2 Friendly Companion January 2014 Editor: Mr. G.D. Buss, “Bethany,” 7 Laines Head, Chippenham, Wiltshire, SN15 1PH. Tel: 01249 656910. Email: [email protected] All correspondence (except that which relates to subscriptions) to be sent to the Editor. Annual Subscriptions inc. postage: U.K. U.S.A. & Canada Australia Europe (Netherlands) £13.50 $36 A$38 €25.00 All correspondence concerning subscriptions should be addressed to Mr. D. Christian, 5, Roundwood Gardens, Harpenden, Herts. AL5 3AJ. Cheques should be made out to Gospel Standard Publications. For United States and Canada, please send to Mr. G. Tenbroeke, 1725 Plainwood Drive, Sheboygan, Wisconsin 53081, USA. Volume 140 January 2014 CONTENTS Our Monthly Message 3 Our Front Cover Picture 4 Good Wishes 5 For The Very Little Ones: Naomi Returns 6 Colouring Text: Ruth 1. 22. 7 Bible Lessons: The Burial Of Jesus 8 Three ‘B’s For 2014 10 A Dark Episode 12 Naaman 17 Sin 17 The Necessity Of Divine Life 18 Editor’s Postbag 18 Fascinating Flowerpots 19 Bible Study For The Older Ones: Light And Darkness (I) 20 Bible Questions: Washing And Making Clean 22 Poetry: A Conversation Between Two Brothers 24 Friendly Companion January 2014 3 OUR MONTHLY MESSAGE Dear Children and Young People, As you pick up the Friendly Companion this month it will be to read the first issue of another year. How quickly, to those of us who are older, do the years fly past! When you are younger, often time seems to drag, and there is a danger that you might wish your time away faster than God intends. -

An Interim Report on the Results of the Lairg Project 1988 - 1992 R.P.J
AN INTERIM REPORT ON THE RESULTS OF THE LAIRG PROJECT 1988 - 1992 R.P.J. McCullagh Abstract This paper reviews the archaeological fieldwork undertaken at Lairg, Sutherland from 1988 to 1991 and reports on the preliminary results ofpost-excavation analyses. This programme was established at the instigation of regional and national heritage agencies to advise on a route for a proposed upgraded road. Standard and innovatory techniques of archaeological excavation and survey were combined with various environmental approaches in an attempt to map the evolution of the present-day landscape. In particular, the project has sought to identify and analyse the crucial role of land-use in this evolution. Introduction The recent archaeological work at Lairg, in eastern Sutherland, took place within a corridor of land that straddles the A836. This corridor measures 2.2 miles (3.5km) by a maximum of 330yds (O.3km) and runs north from Achinduich farm to about 0.6 miles (lkm) south of the village of Lairg (Fig. 1). The then Highland Regional Roads Authority (HRRA) informed Historic Scotland and sought assistance in achieving a route that would cause the least damage to the archaeological remains in the corridor. The archaeological project that developed from this enquiry has been funded by Highland Regional Council and Historic Scotland. The fieldwork spanned four years: 1988 a topographic survey of upstanding monuments; 1989 a test-pit sampling programme; 1990 a short season of scientific sampling; 1990 an eight week season of excavations; 1991 a further eight week season of excavations. Further fieldwork directed towards the sampling needs of two associated research studentships (see below) has also been undertaken. -

1 COUNTYOFNEWYORK . in the Matter of Proving the Last Will And
1 COUNTY OF NEW YORK. In the Matter of Proving the Last Will and Testament of J ~ / Amended and Supplemental ANDREW CARNEGIE ( Notice of Probate. Deceased, > | Sec. 2616. And a Codicil thereto as a Will and Codicil of Real and\ ^ Personal Property. TO THE FOLLOWING NAMED PERSONS: TAKE NOTICE that the last will and testament of Andrew Carnegie, late of the County of New York, State of New York, deceased, has been offered for probate, and that the names and post-office addresses of the proponent and of the legatees, devisees and other beneficiaries, as set forth in the petition herein, who have not been cited or have not appeared or waived citation, are as follows: Home Trust Company, the proponent, whose post-office address is 51 Newark Street, Hoboken, New Jersey. Name of Legatee, Devisee or Beneficiary Post-Office Address Mrs. Leander M. Morris Oakmont, Allegheny County, Pa. Miss Cora B. Morris, 231 Hulton Road Oakmont, Allegheny County, Pa. Miss Mary B. Morris, 231 Hulton Road Oakmont, Allegheny County, Pa. Mrs. Thetta Quay Franks 135 East 66th Street, New York City. Cooper Union for the Advancement of Science and Art Cooper Square, cor. Third Aye,, New York. University of Pittsburgh , State Hall, Grant Boulevard, Pitts• burgh, Pa. Authors' Club, New York Carnegie Hall, New York City. Hampton Normal & Agricultural Institute Hampton, Virginia. Stevens Institute of Technology Castle Point, Hoboken, N. J. St. Andrews Society of the State of New York New York City. George Irvine - Fairfaaven, Watson Street,Baucbory, Kincardineshire, Scotland. Mrs. Eliza S. Nicoll InVerkip, Renfrewshire, Scotland. Miss Margaret Anderson 3.Roseburn Place, Murrayfield, Edin• burgh, Scotland. -

Scotland) Act 1997
Directorate for Planning and Environmental Appeals abcdefghijklmnopqrstu TOWN AND COUNTRY PLANNING (SCOTLAND) ACT 1997 REPORT TO THE HIGHLAND COUNCIL DEVELOPMENT PLAN EXAMINATION: SUTHERLAND LOCAL PLAN Reporters: Allison Coard MA MPhil MRTPI Richard Dent BA(Hons) DipTP FRTPI Date of Report: January 2010 CONTENTS Issue No Subject Page No 1. Dornoch - Prospects/General Comment 1- 3 2. Dornoch - General Comment 4- 6 3. Dornoch - H1 Bishopfield 7- 9 4. Dornoch - H2 Earl’s Cross 10 - 11 5. Dornoch - H3 Sutherland Road 12 - 14 6. Dornoch - H4 Meadows Park Road 15 - 18 7. Dornoch - MU1 Dornoch North 19 - 23 8. Dornoch - LT Dornoch North Expansion 24 - 25 9. Dornoch - C1 Meadows Park 26 - 27 10. Embo Settlement Development Area 28 - 32 11. Golspie Settlement Development Area 33 12. Golspie - H3 Adjacent Macleod House 34 - 35 13. Golspie - MU1 Mackay House Hotel Site 36 - 37 14. Golspie - MU2 Drummuie 38 - 40 15. Pittenrail - MU1 Mart and Adjoining Land 41 - 42 16. Brora Settlement Development Area 43 17. Brora - Prospects 44 18. Brora - Development Factors 45 19. Brora - H1 East Brora Muir 46 - 47 20. Brora - H2 Tordale, & H3, West of Masonic Hall, 48 - 50 Settlement Development Area (H5, South of Academy Street (deleted)) 21. Brora - H4, Rosslyn Street; MU4, Former Mackays 51 - 53 Yard 22. Brora - MU1 Former Radio Station 54 - 55 23. Brora - MU2 Scotia House 56 - 58 24. Brora - MU3 Carrol House 59 - 60 25. Brora - I1 Adjoining Industrial Estate 61 26. Helmsdale - North of Rockview Place & I1 North of 62 - 64 Industrial Estate 27. Helmsdale - MU1 Shore Street 65 28. -

Minutes of Meeting Held on Monday, 10Th June 2019 in Ardgay Hall at 7.00Pm Minutes Approved 12/08/2019
Minutes of meeting held on Monday, 10th June 2019 in Ardgay Hall at 7.00pm Minutes approved 12/08/2019 Present: Betty Wright, Chair (BW), Silvia Muras, Vice Chair (SM), Marion Turner, Secretary/Treasurer (MT), Andy Wright (AW), Apologies: Buster Crabb (BC), Rob Pope (RP) Also present: Vicky and John Denniston, Lee McNeish (LMN) Police Scotland: No representative Minutes Secretary: Mary Goulder Items 1/2. Welcome/Apologies (as above). Chair Betty Wright opened the meeting which followed directly after the AGM. Item 3. Minutes of last meeting. The minutes of the April meeting were approved as a true and accurate record, proposed: Silvia Muras; seconded: Marion Turner. Item 4. Matters arising. (1) Highland Council and Climate change. The CC has asked THC to declare a Climate Emergency. A motion on this subject was carried and a committee is being formed within THC. CC will monitor with interest. A local group, Planet Sutherland, has been set up aiming to spread awareness and action. At the April CC meeting Cllr Currie spoke about THC’s Waste Management plans. It was agreed that the Waste Management Officer should be invited to the next CC meeting. A list of specific questions will be sent to him with the invitation to the August meeting. BW Action. (2) Recycling point. The bins are back in place. (3) Development at Port of Cromarty Firth. No reply as yet from Joanne Sutherland. Fears remain regarding the increase in traffic to and from Ardchronie Quarry though it is understood some of the required stone will be brought in by sea. -
Cycle Routes Around Dornoch
Cycle Routes Around Dornoch quiet roads and glorious scenery Includes the Good Cycling Code his part of Sutherland was Spinningdale Mill T made for cycling – quiet (Route 5) roads, gentle gradients, and just so much to see. All our cycle routes start at the Tourist Information Centre in The Square, Dornoch, where you’ll find a vast amount of help, information, personal attention and local knowledge. Routes have been planned to avoid major roads and steep gradients wherever possible, whilst taking in the most spectacular scenery, historical sites and places where you’re most likely to see some of our more exotic Highland wildlife. Routes 1 and 2 take you past the fishing village of Embo to within sight of the old ferry port of Littleferry, visible across Loch Fleet, an internationally-renowned nature reserve where you can see an incredibly diverse range of ducks and waders. Route 3 extends the tour, beside the remains of the old “Dornoch Light Railway” line, along the edge of Loch Fleet to join the A9 at Cambusavie. Route 4 will show you the disused Dornoch Firth ferry terminal at Meikle Ferry, site of a great disaster in 1809 when 99 passengers were drowned in a storm. It took nearly 200 years to bridge the Firth here, although lighthouse designer George Stephenson drew up plans for a huge wooden bridge in 1831 which you can see in Dornoch’s “Historylinks” museum. Route 5 is for the energetic romantic, following the old A9 towards Bonar Bridge and ‘cutting the corner’ through Migdale’s “Fairy Glen,” an area of outstanding natural beauty. -

SUTHERLAND Reference to Parishes Caithness 1 Keay 6 J3 2 Thurso 7 Wick 3 Olrig 8 Waiter 4 Dunnet 9 Sauark 5 Canisbay ID Icajieran
CO = oS BRIDGE COUNTY GEOGRAPHIES -CD - ^ jSI ;co =" CAITHNESS AND SUTHERLAND Reference to Parishes Caithness 1 Keay 6 J3 2 Thurso 7 Wick 3 Olrig 8 Waiter 4 Dunnet 9 SaUark 5 Canisbay ID IcaJieran. Sutherland Durnesx 3 Tatujue 4 Ibrr 10 5 Xildsjnan 11 6 LoiK 12 CamJbriA.gt University fi PHYSICAL MAP OF CAITHNESS & SUTHERLAND Statute Afiie* 6 Copyright George FkOip ,6 Soni ! CAITHNESS AND SUTHERLAND CAMBRIDGE UNIVERSITY PRESS C. F. CLAY, MANAGER LONDON : FETTER LANE, E.C. 4 NEW YORK : THE MACMILLAN CO. BOMBAY | CALCUTTA !- MACMILLAN AND CO., LTD. MADRAS J TORONTO : THE MACMILLAN CO. OF CANADA, LTD. TOKYO : MARUZEN-KABUSHIKI-KAISHA ALL RIGHTS RESERVED CAITHNESS AND SUTHERLAND by H. F. CAMPBELL M.A., B.L., F.R.S.G.S. Advocate in Aberdeen With Maps, Diagrams, and Illustrations CAMBRIDGE AT THE UNIVERSITY PRESS 1920 Printed in Great Britain ly Turnbull &* Spears, Edinburgh CONTENTS CAITHNESS PACK 1. County and Shire. Origin and Administration of Caithness ...... i 2. General Characteristics .... 4 3. Size. Shape. Boundaries. Surface . 7 4. Watershed. Rivers. Lakes . 10 5. Geology and Soil . 12 6. Natural History 19 Coast Line 7. ....... 25 8. Coastal Gains and Losses. Lighthouses . 27 9. Climate and Weather . 29 10. The People Race, Language, Population . 33 11. Agriculture 39 12. Fishing and other Industries .... 42 13. Shipping and Trade ..... 44 14. History of the County . 46 15. Antiquities . 52 1 6. Architecture (a) Ecclesiastical . 61 17. Architecture (6) Military, Municipal, Domestic 62 1 8. Communications . 67 19. Roll of Honour 69 20. Chief Towns and Villages of Caithness . 73 vi CONTENTS SUTHERLAND PAGE 1.