Stages of Labour Chart
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Anatomy of the Rectum and Anal Canal
BASIC SCIENCE identify the rectosigmoid junction with confidence at operation. The anatomy of the rectum The rectosigmoid junction usually lies approximately 6 cm below the level of the sacral promontory. Approached from the distal and anal canal end, however, as when performing a rigid or flexible sigmoid- oscopy, the rectosigmoid junction is seen to be 14e18 cm from Vishy Mahadevan the anal verge, and 18 cm is usually taken as the measurement for audit purposes. The rectum in the adult measures 10e14 cm in length. Abstract Diseases of the rectum and anal canal, both benign and malignant, Relationship of the peritoneum to the rectum account for a very large part of colorectal surgical practice in the UK. Unlike the transverse colon and sigmoid colon, the rectum lacks This article emphasizes the surgically-relevant aspects of the anatomy a mesentery (Figure 1). The posterior aspect of the rectum is thus of the rectum and anal canal. entirely free of a peritoneal covering. In this respect the rectum resembles the ascending and descending segments of the colon, Keywords Anal cushions; inferior hypogastric plexus; internal and and all of these segments may be therefore be spoken of as external anal sphincters; lymphatic drainage of rectum and anal canal; retroperitoneal. The precise relationship of the peritoneum to the mesorectum; perineum; rectal blood supply rectum is as follows: the upper third of the rectum is covered by peritoneum on its anterior and lateral surfaces; the middle third of the rectum is covered by peritoneum only on its anterior 1 The rectum is the direct continuation of the sigmoid colon and surface while the lower third of the rectum is below the level of commences in front of the body of the third sacral vertebra. -

Introduction Remove the Udder Removing the Pizzle (Penis)
fig . removing the udder, cut outwards through the skin fig 2. removing the pizzle Introduction This guide describes the carcass dressing procedures either side of the pizzle joining the cuts around the that are ideally carried out in a deer larder, after back of the scrotum. Continue the single central cut the gralloch has been performed in the field. The through the skin almost to the anus, taking care not Gralloch guide should be considered essential to damage the haunches. Pull the pizzle free where it companion reading. Both are linked to the Carcass runs over the pelvis, cutting the blood vessels. Use Inspection, Carcass Transport, Basic Hygiene, and the knife to free the pizzle where it turns forward Larder guides. inside the “V” of the pelvis. Leave outside the carcass (draped down the back if the carcass is suspended). Remove the udder It will be removed with the aitch bone, bladder, Fig 1. This is best done in the larder but a large udder remainder of the rectum and anus, later. can prevent access to the rear end and may have to be removed in the field before opening the stomach. Split the aitch bone Pinch the skin just in front of the udder and pulling Figs 3. and 4. Note that some venison processors on it all the time, cut around the udder, removing it would prefer that the aitch bone remains intact, whole, with the skin. Do not take the cut any further check before cutting. While causing the least possible rearwards until back in the larder. -

How to Increase Your Enjoyment of Sex
BETTER SEX BETTER SEX BETTER SEX BETTER SEX BETTER SEX OF SEX ENJO YOUR INCREASE HOW TO for women and women for their partners YMENT “Sexual health is a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled.” Definition of sexual health, World Health Organisation SAFER SEX Using condoms for penetrative sex is the best way to protect yourself and your partners from Sexually Transmitted Infections, including HIV. Condoms also offer good protection from unwanted pregnancy. In the text of this booklet, we have chosen not to refer constantly to the use of condoms. Instead, we encourage you to make your own decisions about protecting yourself and others in each instance of sexual activity you undertake. 1 HOW TO INCREASE YOUR ENJOYMENT OF SEX This leaflet provides information on how to help yourself improve your enjoyment of sex. It has three main parts: Suggestions on how to improve sex generally, without doing formal exercises. These apply to both casual and regular partners. Exercises you can do on your own — for women who have difficulty getting turned on or experiencing orgasm, and who may or may not have a regular partner. Exercises you can do with a partner — for women who have difficulty getting turned on, or who have difficulty having an orgasm or enjoying penetrative sex. -

Clinical, Pathologic and Pharmacologic Correlations 2004
HUMAN REPRODUCTION: CLINICAL, PATHOLOGIC AND PHARMACOLOGIC CORRELATIONS 2004 Course Co-Director Kirtly Parker Jones, M.D. Professor Vice Chair for Educational Affairs Department of Obstetrics and Gynecology Course Co-Director C. Matthew Peterson, M.D. Professor and Chief Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology 1 Welcome to the course on Human Reproduction. This syllabus has been recently revised to incorporate the most recent information available and to insure success on national qualifying examinations. This course is designed to be used in conjunction with our website which has interactive materials, visual displays and practice tests to assist your endeavors to master the material. Group discussions are provided to allow in-depth coverage. We encourage you to attend these sessions. For those of you who are web learners, please visit our web site that has case studies, clinical/pathological correlations, and test questions. http://medstat.med.utah.edu/kw/human_reprod 2 TABLE OF CONTENTS Page Lectures/Examination................................................................................................................................... 4 Schedule........................................................................................................................................................ 5 Faculty .......................................................................................................................................................... 8 Groups ......................................................................................................................................................... -
Pregnancy Guide (PDF)
ɶɶYourɶPregnancyɶGuide ©ɶ2012ɶStartɶSmartɶforɶYourɶBaby.ɶAllɶrightsɶreserved. ɶ Start Smart Pregnancy Book Congratulations! You are going to have a tips to manage morning sickness from other baby! Having a baby is a special privilege. moms-to-be like you. Read about needed tests It is the beginning of the strongest of all and times you’ll want to visit the doctor. bonds—the bond between a parent and child. Some people read this booklet cover to cover. Both first-time moms and women who Others turn to the section they want to know already have children will want to read this more about. Glance at the What’s booklet. Learn how you can give your baby a Inside section to guide you to each topic. healthy start in life by taking care of yourself Also, be sure to share this booklet with while you are pregnant. See how your baby is your friends and family as you enter an growing each month. Find out tried and true exciting new journey—the birth of your baby. For more information on prenatal care, visit us at www.startsmartforyourbaby.com ❘ 4 ❘ Start Smart Pregnancy Book ɶ What’s Inside: Your First OB Visit .................................................2 Your Case Manager Can Help You Stay Healthy ...............................3 Prenatal Testing .....................................................4 Body Basics— Your Reproductive System .................................8 Taking Care of Your Emotions ...........................40 A Peek Inside Your Body .....................................9 Getting Ready for the Big Day ...........................41 -
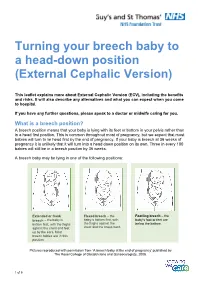
Turning Your Breech Baby to a Head-Down Position (External Cephalic Version)
Turning your breech baby to a head-down position (External Cephalic Version) This leaflet explains more about External Cephalic Version (ECV), including the benefits and risks. It will also describe any alternatives and what you can expect when you come to hospital. If you have any further questions, please speak to a doctor or midwife caring for you. What is a breech position? A breech position means that your baby is lying with its feet or bottom in your pelvis rather than in a head first position. This is common throughout most of pregnancy, but we expect that most babies will turn to lie head first by the end of pregnancy. If your baby is breech at 36 weeks of pregnancy it is unlikely that it will turn into a head down position on its own. Three in every 100 babies will still be in a breech position by 36 weeks. A breech baby may be lying in one of the following positions: Extended or frank Flexed breech – the Footling breech – the breech – the baby is baby is bottom first, with baby’s foot or feet are bottom first, with the thighs the thighs against the below the bottom. against the chest and feet chest and the knees bent. up by the ears. Most breech babies are in this position. Pictures reproduced with permission from ‘A breech baby at the end of pregnancy’ published by The Royal College of Obstetricians and Gynaecologists, 2008. 1 of 5 What causes breech? Breech is more common in women who are expecting twins, or in women who have a differently-shaped womb (uterus). -

Bowel Function Anatomy
BOWEL FUNCTION ANATOMY Most of America gives little thought to bowel control. However, bowel control is actually a complex process involving the coordination of many different muscles and nerves. The bowel is considered to be a part of the digestive or gastrointestinal system. It is designed to help the body absorb nutrients and fluids from the foods we eat and drink. After taking out everything the body needs, the bowel then expels the leftover waste. The beginning of the bowel is the small intestine, sometimes referred to as the small bowel. This is where the useful nutrients are absorbed from what you eat. The small bowel delivers the waste to the colon, or large bowel. The colon is a 5-6 foot long muscular tube that delivers stool to the rectum. As the stool moves through the colon, the fluids are removed and absorbed into the body. The consistency of the stool is dependent upon many things, including how long the stool sits in the colon, how much of the water has been absorbed from the waste, and the amount of fiber and fluids in your diet. Stool consistency can vary from hard lumps to mushy to very loose, watery stool. The best and easiest consistency of stool is soft, like toothpaste; this consistency may be attained by adding fiber to your diet. Fiber helps move waste through the colon because it is indigestible by the human body. In other words, fiber adds ‘bulk’ to the stool. It is important to eat a diet high in fiber, however, most Americans lack fiber in their diet. -

Anal Sex an Informative Guide by Bedroom Kandi
AN INTRODUCTION TO ANAL SEX AN INFORMATIVE GUIDE BY BEDROOM KANDI Anal sex encompasses a variety of sexual acts involving the anus and rectum. These can include anal fingering, analingus (oral-anal sex, sometimes called “rimming”), anal insertion (using an object like a strap-on or other toy) and anal intercourse (penis-in-anus sex). Anal sex can be enjoyed by individuals of any gender, and any orientation. Everyone has a back door, after all! But it requires preparation, care, and patience to make it pleasurable. Communication is Key! No surprise butt-sex. Always check in with your partner, talk things through, and 36% communicate about whether you’re Of American Women both on board for trying anal. Check in during anal sex to report having tried ? make sure you’re both enjoying yourselves! ANAL SEX “Is Anal Sex Common?” International Society for Sexual Medicine :) http://www.issm.info/sexual-health-qa/is-anal-sex-common/ www.bedroomkandi.com ©2017 Bedroom Kandi WHY TRY ANAL? IT FEELS GOOD - There are a lot IT FEELS BAD - in a good way! The of nerve endings to stimulate around taboos around anal sex can make it a the anus, including those in the man’s thrill and add something exciting to your prostate. bedroom routine. You naughty thing! IT SPICES THINGS UP - Trying IT CAN SUBVERT GENDER new things keeps things fresh, and ROLES - Either partner can penetrate anal sex will open up a whole new or receive, (using strap-ons or other toys range of sexual positions and activities for Lesbian or Straight couples), so you for you and your partner to share. -

Maternal Movement and Position Changes to Facilitate Labor Progress Have Been Discussed in the Literature for Decades
ELAINE ZWELLING, PHD, RN, LCCE, FACCE Abstract The benefi ts of maternal movement and position changes to facilitate labor progress have been discussed in the literature for decades. Recent routine interventions such as amniotomy, induction, fetal monitoring, and epidural anesthesia, as well as an increase in maternal obesity, have made position changes during labor challenging. The lack of maternal changes in position throughout labor can contribute to dystocia and increase the risk of cesarean births for failure to progress or descend. This article provides a historical review of the research fi ndings related to the effects of maternal positioning on the labor process and uses six physiological principles as a framework to offer sug- gestions for maternal positioning both before and after epidural anesthesia. Key Words Birth; Childbirth; Labor, fi rst stage; Labor, second stage; Maternity nursing; Obstetrical nursing; Maternal postures; Maternal positioning. Overcoming the Challenges: Maternal Movement 72 volume 35 | number 2 March/April 2010 or centuries laboring women chose to remain dural anesthesia, found that women who were able to mobile and upright, using positions such as change positions regularly or maintain upright positions standing, sitting, kneeling, hands and knees, or during labor were more comfortable and required less Fsquatting (Gupta & Nikodem, 2000; Johnson, pain medication (Atwood, 1976; de Jong et al., 1997; En- Johnson, & Gupta, 1991). Today immobility throughout gelmann, 1977; Johnson et al., 1991). For instance, Ada- the labor process has become a common occurrence for chi, Shimada, and Usul (2003) found in their study of 58 many childbearing women. Increased medical manage- laboring women that a sitting position decreased labor ment, obesity, lack of patient understanding about the pain in contrast with supine positioning. -

Know the Signs of Labor
Know the Signs of Labor Learn the signs of labor so that you know when to call your doctor and go to the hospital for delivery. Mucus plug Some women have a release of cervical mucus that may have a slight pink color, or blood- tinged. This is called passing a mucus plug or a bloody show. This may be a sign that your body is preparing for delivery, but you do not need to call your health care provider. Rupture of membranes (water breaks) Rupture of membranes is the medical term for your water breaking. This is your amniotic fluid. It can be a gush or a slow trickle and should be a clear, slightly yellow color. Often, a woman will go into labor soon after her water breaks. If this doesn’t happen, your health care provider may talk with you about helping your labor along with medicine. If you think your water has broken, call your doctor and go to the hospital. Do not take a bath or put anything into your vagina. You may wear a pad. Contractions Contractions are the tightening and relaxing of muscles in the uterus. When labor starts, these muscles tighten and relax at a regular pace. They will get closer together and stronger, letting your body know that your baby is about to be born. Sometimes, these muscle contractions are not regular, and they start and stop. They do not seem to get stronger and closer together, but stay about the same intensity. Your health care provider may describe these contractions as Braxton-Hicks or signs of false labor. -

Variation in Fetal Presentations and Positions Among Women in Warri, Delta State, Nigeria
World Research Journal of Obstetrics and Gynecology ISSN: 2277-6001, Volume 2, Issue 1, 2013, pp.-10-12. Available online at http://www.bioinfopublication.org/jouarchive.php?opt=&jouid=BPJ0000126 VARIATION IN FETAL PRESENTATIONS AND POSITIONS AMONG WOMEN IN WARRI, DELTA STATE, NIGERIA OLANIYAN O.T.1*, MERAIYEBU A.B.1, ALELE J.Y.1, DARE J.B.2, ATSUKWEI D.1 AND ADELAIYE A.B.1 1Department of Physiology, Bingham University, Karu, Nasarawa, Nigeria. 2Department of Anatomy, Bingham University, Karu, Nasarawa, Nigeria. *Corresponding Author: Email- [email protected] Received: November 21, 2013; Accepted: December 23, 2013 Abstract- This study investigates the various fetal presentations among women in Warri and the various predisposing factors which may have possibly brought about these variations; the major positions considered were cephalic, breech and transverse, with the considered influencing factors being gestational age of the fetus, maternal age, amniotic fluid volume, parity, and method of previous deliveries. A total of 105 ultra- sound fetal biometries with a total of 108 fetuses, between 15-40 weeks of gestational age, and maternal age between 19 and 40 were used for this study. Fetal ultrasound biometry was used to find out information about the fetus including gestational age, amniotic fluid volume, presentation of the fetus and a questionnaire was used to take information about the mother including maternal age, parity, and method of previous delivery (ies). The result showed that a total of 82 fetuses (75.9%) were Cephalic babies, 19 (17.6%) were Breech and 7 (6.5%) are transverse. Out of the 105 women, there were 102 (77.1% cephalic, 18.3% breech, 4.8% transverse) women with adequate amniotic fluid volume and 1 woman (with a cephalic fetus) with average amniotic fluid volume and 2 women (with transverse foetuses) with low amniotic fluid volume. -

Your Pregnancy Guide IMPORTANT CONTACTS
Your Pregnancy Guide IMPORTANT CONTACTS FILL IN THIS INFORMATION SO YOU HAVE IT WHEN YOU NEED IT. Healthcare Provider Phone Address City After Hours Phone Hospital Phone Address Health Department Phone Address Maternity Care Coordinator Phone In Case of Emergency, Contact: Name Phone Name Phone MY PRENATAL APPOINTMENTS USE THIS SPACE TO WRITE DOWN YOUR PRENATAL APPOINTMENTS. WEEK DATE TIME WEEK DATE TIME 1 to 4 33 to 34 5 to 8 35 to 36 9 to 12 37 13 to 16 38 17 to 20 39 21 to 24 Due Date ? 25 to 28 40 29 to 30 41 31 to 32 42 If you can’t keep an Childbirth Class Date: Time: appointment, Breastfeeding Class Date: Time: remember to RESCHEDULE. My Postpartum Visit Date: Time: CONGRATULATIONS! You are going to be a mother! You may feel like you have no control over what’s happening to your body and emotions anymore. But you do! What you do during your pregnancy will make a difference. It’s important to take care of yourself physically and emotionally. The more you know about what’s happening and the more you let others know how you feel, the more in control you will be. This book answers lots of questions pregnant women ask. But remember, every pregnancy is different. Even if you’ve been pregnant before, this pregnancy can be very different. When you are pregnant, you will have many prenatal appointments with your healthcare providers. Prenatal is a term that refers to when you are pregnant. Pre = before and natal = birth.