Frede Olesen Former GP Professor, Drmedsci Research Unit for General Practice, Aarhus University
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Meta Analysis of County, Gender, and Year Specific Effects of Active Labour Market Programmes
A Meta Analysis of County, Gender, and Year Speci…c E¤ects of Active Labour Market Programmes Agne Lauzadyte Department of Economics, University of Aarhus E-Mail: [email protected] and Michael Rosholm Department of Economics, Aarhus School of Business E-Mail: [email protected] 1 1. Introduction Unemployment was high in Denmark during the 1980s and 90s, reaching a record level of 12.3% in 1994. Consequently, there was a perceived need for new actions and policies in the combat of unemployment, and a law Active Labour Market Policies (ALMPs) was enacted in 1994. The instated policy marked a dramatic regime change in the intensity of active labour market policies. After the reform, unemployment has decreased signi…cantly –in 1998 the unemploy- ment rate was 6.6% and in 2002 it was 5.2%. TABLE 1. UNEMPLOYMENT IN DANISH COUNTIES (EXCL. BORNHOLM) IN 1990 - 2004, % 1990 1992 1994 1996 1998 2000 2002 2004 Country 9,7 11,3 12,3 8,9 6,6 5,4 5,2 6,4 Copenhagen and Frederiksberg 12,3 14,9 16 12,8 8,8 5,7 5,8 6,9 Copenhagen county 6,9 9,2 10,6 7,9 5,6 4,2 4,1 5,3 Frederiksborg county 6,6 8,4 9,7 6,9 4,8 3,7 3,7 4,5 Roskilde county 7 8,8 9,7 7,2 4,9 3,8 3,8 4,6 Western Zelland county 10,9 12 13 9,3 6,8 5,6 5,2 6,7 Storstrøms county 11,5 12,8 14,3 10,6 8,3 6,6 6,2 6,6 Funen county 11,1 12,7 14,1 8,9 6,7 6,5 6 7,3 Southern Jutland county 9,6 10,6 10,8 7,2 5,4 5,2 5,3 6,4 Ribe county 9 9,9 9,9 7 5,2 4,6 4,5 5,2 Vejle county 9,2 10,7 11,3 7,6 6 4,8 4,9 6,1 Ringkøbing county 7,7 8,4 8,8 6,4 4,8 4,1 4,1 5,3 Århus county 10,5 12 12,8 9,3 7,2 6,2 6 7,1 Viborg county 8,6 9,5 9,6 7,2 5,1 4,6 4,3 4,9 Northern Jutland county 12,9 14,5 15,1 10,7 8,1 7,2 6,8 8,7 Source: www.statistikbanken.dk However, the unemployment rates and their evolution over time di¤er be- tween Danish counties, see Table 1. -
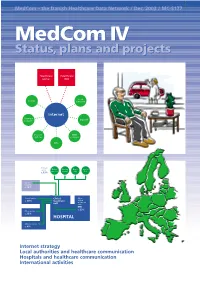
Medcom IV Status, Plans and Projects
MedCom – the Danish Healthcare Data Network / Dec. 2003 / MC-S177 MedComMedCom IV IV Status,Status, plans plans andand projectsprojects Healthcare Healthcare portal DIX Local County authority Internet Pharmacy Dan Net network Doctors’ KMD systems network KPLL Primary sector Medical Nursing Home Specia- practice homes care lists c. 13% Other hospitals c. 10% Clinical service Clinical Other c. 40% treatment clinical treatment unit units EPR c. 23% Other service c. 13% HOSPITAL Administration c. 4% ● Internet strategy ● Local authorities and healthcare communication ● Hospitals and healthcare communication ● International activities 2 MedCom IV – status, plans and projects Contents Aims of MedCom 2 The local authorities and healthcare communication 20 Introduction 3 The Hospital-Local Authority XML project 20 Healthcare on the move 3 The Hospital-Local Authority project and Common Language 22 History 4 Commentary: The Minister of Social Affairs, Henriette Kjær 22 The MedCom steering group 6 The LÆ form project 23 Commentary: The Minister of the Interior and Commentary: The Chairman of the National Health, Lars Løkke Rasmussen 7 Association of Local Authorities, Perspective: MedCom certifies communication 8 Ejgil W. Rasmussen 24 Perspective: The IT Lighthouse’s local authority- The Internet strategy 9 medical practice communication 24 The infrastructure project 9 The hospitals and Commentary: The Chairman of the Association of healthcare communication 25 County Councils, Kristian Ebbensgaard 12 Perspective: The Internet strategy and the From -

The Parliamentary Electoral System in Denmark
The Parliamentary Electoral System in Denmark GUIDE TO THE DANISH ELECTORAL SYSTEM 00 Contents 1 Contents Preface ....................................................................................................................................................................................................3 1. The Parliamentary Electoral System in Denmark ..................................................................................................4 1.1. Electoral Districts and Local Distribution of Seats ......................................................................................................4 1.2. The Electoral System Step by Step ..................................................................................................................................6 1.2.1. Step One: Allocating Constituency Seats ......................................................................................................................6 1.2.2. Step Two: Determining of Passing the Threshold .......................................................................................................7 1.2.3. Step Three: Allocating Compensatory Seats to Parties ...........................................................................................7 1.2.4. Step Four: Allocating Compensatory Seats to Provinces .........................................................................................8 1.2.5. Step Five: Allocating Compensatory Seats to Constituencies ...............................................................................8 -

Screening for Chlamydia Trachomatis in Denmark
Screening for Chlamydia trachomatis in Denmark Attitudes among professionals and youth towards a strategy for sexual and reproductive health The potential of ‘The Aarhus Model’ for healthy public policy Master of Public Health Thesis Mette Kjer Kaltoft Date: 23rd of December 2003 Supervisor: Michael Væth, professor of biostatistics, Ph.d., Aarhus University Master of Public Health, Aarhus University, Denmark 2003 I Table of Contents Acknowledgements III English summary IV Danish summary VII Background 1 Aim of study 10 Part I. Danish public policy towards sexual & reproductive health 11 Material and Method 11 Result and discussion 11 Part II. Doctors 2001 study 16 Material and Method 16 Results 19 Discussion 21 Part III. Youth99 study 26 Material and Method 26 Results 29 Discussion 41 General discussion and conclusions 48 Reference list 59 List over tables 67 Appendices 68 II Acknowledgements I wish to express my gratitude and thanks to the following persons that enabled finishing my MPH thesis, each by a different route: project leader Bjarne Rasmussen who was responsible for ‘Youth 99 - a sexual profile’ study for granting access to the data; project leader and members of the national HTA Chlamydia research group, Lars Østergaard, Berit Andersen, Jens Kleist Møller, and Frede Olesen for letting me join their team and providing a superb and supportive work environment and last not least my MPH supervisor Michael Vaeth, professor of biostatistics, University of Aarhus, for human, humorous and literally numerous advice, in particular with the recoding of data and statistical analysis. Also, I want to send warm thoughts and thanks to all 7355 pupils who answered the ’youth 99’ questionnaire and the 401 physicians who despite not being reimbursed answered the questionnaire ‘doctors 2001’. -

University of Copenhagen
Determinants of Recent Immigrants¿ Location Choices Quasi-Experimental Evidence Damm, Anna Piil Publication date: 2005 Document version Publisher's PDF, also known as Version of record Citation for published version (APA): Damm, A. P. (2005). Determinants of Recent Immigrants¿ Location Choices: Quasi-Experimental Evidence. Department of Economics, University of Copenhagen. Download date: 26. Sep. 2021 CAM Centre for Applied Microeconometrics Department of Economics University of Copenhagen http://www.econ.ku.dk/CAM/ Determinants of Recent Immigrants’ Location Choices: Quasi-Experimental Evidence Anna Piil Damm 2005-17 The activities of CAM are financed by a grant from The Danish National Research Foundation Determinants of Recent Immigrants’ Location Choices: Quasi-Experimental Evidence∗ Anna Piil Damm† October 14, 2005 Abstract This paper exploits a Danish spatial dispersal policy on refugees which can be regarded a natural experiment to investigate the influence of regional factors on recent immigrants’ location choices. The main push factors are lack of co-ethnics and presence of immigrants. Addi- tional push factors are lack of access to jobs, education and housing which explain why recent immigrants are attracted to large cities. Finally, placed refugees are sen- sitive to regional unemployment and some evidence of welfare seeking is presented as well. JEL classifications: J15, R15 and H0. Keywords: Location Choices, Push Factors, Immigrants. 1 Introduction It is a common international phenomenon that the immigrant population is geographically concentrated. In 1990, 63% of the foreign born population in the United States were clustered in the four most populous states, California, New York, Florida and Texas, where only 31% of the overall population lived (Zavodny 1997). -

Accountability Practices in the History of Danish Primary Public Education from the 1660S to the Present Christian Ydesen & Karen E
SPECIAL ISSUE The Comparative and International History of School Accountability and Testing education policy analysis archives A peer-reviewed, independent, open access, multilingual journal epaa aape Arizona State University Volume 22 Number 120 December 8th, 2014 ISSN 1068-2341 Accountability Practices in the History of Danish Primary Public Education from the 1660s to the Present Christian Ydesen & Karen E. Andreasen Aalborg University Denmark Citation: Ydesen, C., & Andreasen, K. E. (2014). Accountability practices in the history of Danish primary public education from the 1660s to the present. Education Policy Analysis Archives, 22(120). http://dx.doi.org/10.14507/epaa.v22.1618. This article is part of EPAA/AAPE’s Special Issue on The Comparative and International History of School Accountability and Testing, Guest Co-Edited by Dr. Sherman Dorn and Dr. Christian Ydesen. Abstract: This paper focuses on primary education accountability as a concept and as an organizational practice in the history of Danish public education. Contemporary studies of education policy often address questions of accountability, but the manifestations of school accountability differ significantly between different national settings. Furthermore, accountability measures and practices have an impact on both the ways and means by which societies approach their educational systems. Hence there is a need to clarify the characteristics and traits connected with the concept. One way of approaching this endeavor is to turn to the history of education, because the discourse and practice of accountability incorporates numerous historical antecedents, technologies, and arguments. Based on primary as well as secondary sources this article presents the case of Denmark, analyzing the period from 1660 to the present. -

Pain in Patients with Multiple Sclerosis a Population-Based Study
ORIGINAL CONTRIBUTION Pain in Patients With Multiple Sclerosis A Population-Based Study Kristina Bacher Svendsen, MD; Troels Staehelin Jensen, MD; Kim Overvad, PhD; Hans Jacob Hansen, MD; Nils Koch-Henriksen, MD; Flemming W. Bach, MD Background: Pain is an important symptom in pa- Results: Response rates for MS patients and reference sub- tients with multiple sclerosis (MS). The estimated pain jects were 81.3% and 63.3%, respectively. Pain in the month prevalence varies between 30% and 90%. To our knowl- preceding assessment occurred in 79.4% of MS patients and edge, previous studies do not include a whole popula- in 74.7% of reference subjects (prevalence proportion ra- tion sample of patients with MS. tio, 1.06; 95% confidence interval, 0.99-1.13). Patients with MS had a higher pain intensity (“when pain is at its least” Objective: To assess pain prevalence and its clinical char- median visual analog scale score, 20.0 vs 11.0 mm [PϽ.01]; acteristics and impact on daily life in a population sample and “when pain is at its worst” median visual analog scale of MS patients and in a reference group. score, 68.0 vs 55.0 mm [PϽ.01]). Daily intake of analge- sics occurred in 24.4% of MS patients and 9.0% of refer- Design: Postal survey. ence subjects (prevalence proportion ratio, 2.7; 95% con- fidence interval, 2.0-3.6). Patients with MS more often Setting: Aarhus County, Denmark. reported that pain interfered with daily life “most of the time” or “all the time.” Participants: The population of patients with definite MS in Aarhus County (n=771) and a sex- and age-stratified ref- Conclusions: The frequency of reported pain in MS patients erence group from the general population (n=769). -
Jutland-Funen, Denmark
OECD/IMHE project Supporting the Contribution of Higher Education Institutions to Regional Development Self-Evaluation Report: Jutland-Funen, Denmark Søren Kerndrup March 2006 0. INTRODUCTION 5 1. OVERVIEW OF THE REGION 7 1.1. The Jutland-Funen Co-operation of Business Development 7 1.2. Geographical situation 7 1.3. Demographic situation 8 1.3.1. Population growth 8 1.4. The economic and social situation in Jutland-Funen 9 1.4.1. Education 9 1.4.2. Personal income 10 1.4.3 Employment 10 1.5. Occupational structure 10 1.5.1. Resource area geographical specialization 11 1.6. Research and development in the public and private sectors 14 1.6.1. Innovation 15 1.6.2. The interaction between knowledge institutions and local industries 15 1.6.3. Use of highly qualified labour force 15 1.6.4. Knowledge based entrepreneurs 15 1.7. The Danish system of government 16 1.7.1. Public sector financing in Denmark 16 1.7.2. Distribution of public sector services in Denmark 16 1.7.3. Distribution of health services 17 1.7.4. Distribution of responsibilities in relation to the promotion of industry and economic development 17 1.7.5. The distribution of responsibilities for educational services 18 1.7.6. Responsibilities for cultural initiatives 20 1.7.7. Financing of the educational system in Denmark 21 1.7.8. Regional influence on higher education and research 22 1.7.9. The Jutland-Funen Co-operation of Business Development 22 1.7.10. The Science and Enterprise Network 22 2. -
The Aquatic Environment in Denmark 1996-1997
Environmental Investigations No. 4 2000 Redegørelse fra Miljøstyrelsen The Aquatic Environment in Denmark 1996-1997 State of Danish freshwaters and inlets in 1996 and 1997 CONTENTS: Foreword 1. Introduction 2. Point sources 3. Freshwater 4. Water courses 5. Lakes 6. Fjords Foreword Since 1990, the results of the monitoring programme of the Action Plan for the Aquatic Environment have been reported in the form of an annual review of the aquatic environment. Nutrients Inputs and concentrations of nutrients and their impact on the aquatic environment are included in the monitoring programme of the Action Plan for the Aquatic Environment. Consequently, these subjects are the core matters of this report. Environmental contaminants and heavy metals In order to produce a more complete picture of the state of the aquatic environment, information has also been obtained about environmental factors beyond the monitoring programme of the Plan. They, for instance, include heavy metals and contaminants. Since 1994, the reports have been thematic. In this report, the theme is the environmental conditions of and developments in Danish freshwater systems and estuaries and fjords. Unfavourable physical conditions and waste water from sparsely populated areas Unfavourable conditions and the input of waste water from sparsely populated areas have great impact on the state of the environment. For this reason it is unlikely that reductions of the nutrient loading of the aquatic environment agreed as a part of the Action Plan for the Aquatic Environment will have any significant influence on the environmental conditions of streams. Phosphorus loading from the countryside has strong influence on lakes In lakes, current and previous discharges of phosphorus from the open country in particular have decisive influence on the state of the environment. -

The Returns to Nursing: Evidence from a Parental Leave Program
NBER WORKING PAPER SERIES THE RETURNS TO NURSING: EVIDENCE FROM A PARENTAL LEAVE PROGRAM Benjamin U. Friedrich Martin B. Hackmann Working Paper 23174 http://www.nber.org/papers/w23174 NATIONAL BUREAU OF ECONOMIC RESEARCH 1050 Massachusetts Avenue Cambridge, MA 02138 February 2017 We thank seminar participants at Aarhus University and Penn State, conference participants at the Junior Health Economics Summit, MHEC, NBER SI Health Care 2016 and AEA HERO Session 2017 as well as Joseph Altonji, John Asker, Craig Garthwaite, Francois Geerolf, Jonathan Gruber, Amanda Kowalski, Adriana Lleras-Muney, Costas Meghir and Mark Pauly for their comments and suggestions. We thank the Labor Market Dynamics Group (LMDG), Department of Economics and Business, Aarhus University and in particular Henning Bunzel and Kenneth Soerensen for invaluable support and making the data available. LMDG is a Dale T. Mortensen Visiting Niels Bohr professorship project sponsored by the Danish National Research Foundation. The views expressed herein are those of the authors and do not necessarily reflect the views of the National Bureau of Economic Research. NBER working papers are circulated for discussion and comment purposes. They have not been peer-reviewed or been subject to the review by the NBER Board of Directors that accompanies official NBER publications. © 2017 by Benjamin U. Friedrich and Martin B. Hackmann. All rights reserved. Short sections of text, not to exceed two paragraphs, may be quoted without explicit permission provided that full credit, including © notice, is given to the source. The Returns to Nursing: Evidence from a Parental Leave Program Benjamin U. Friedrich and Martin B. Hackmann NBER Working Paper No. -

Modelling Regional Variation of First-Time Births in Denmark 1980-1994 by an Age-Period-Cohort Model
Demographic Research a free, expedited, online journal of peer-reviewed research and commentary in the population sciences published by the Max Planck Institute for Demographic Research Konrad-Zuse Str. 1, D-18057 Rostock · GERMANY www.demographic-research.org DEMOGRAPHIC RESEARCH VOLUME 13, ARTICLE 23, PAGES 573-596 PUBLISHED 07 DECEMBER 2005 http://www.demographic-research.org/Volumes/Vol13/23/ DOI: 10.4054/DemRes.2005.13.23 Descriptive Findings Modelling regional variation of first-time births in Denmark 1980-1994 by an age-period-cohort model Lau Caspar Thygesen Lisbeth B. Knudsen Niels Keiding © 2005 Max-Planck-Gesellschaft. Table of Contents 1 Introduction 574 2 Data 575 3 Methods 579 4 Results 580 4.1 Modelling the effects of age, period and cohort 581 4.2 Regional variation 584 5 Discussion 589 6 Conclusion 593 References 594 Demographic Research: Volume 13, Article 23 descriptive findings Modelling regional variation of first-time births in Denmark 1980-1994 by an age-period-cohort model Lau Caspar Thygesen 1 Lisbeth B. Knudsen 2 Niels Keiding 3 Abstract Despite the fact that Denmark is a small country, historically there have been fairly consistent regional differences in fertility rates. We apply the statistical age-period- cohort model to include the effect of these three time-related factors to concisely illuminate the regional differences in first-time births in Denmark. From the Fertility of Women and Couples Dataset we obtain data on the number of births by nulliparous women by year (1980-1994), age (15-45) and county of residence. We show that the APC-model describes the fertility rates of nulliparous women satisfactorily. -

Climate Adaptation in Local Governance: Institutional Barriers in Danish Municipalities
CLIMATE ADAPTATION IN LOCAL GOVERNANCE: INSTITUTIONAL BARRIERS IN DANISH MUNICIPALITIES Scientifi c Report from DCE – Danish Centre for Environment and Energy No. 104 2016 AARHUS AU UNIVERSITY DCE – DANISH CENTRE FOR ENVIRONMENT AND ENERGY [Blank page] CLIMATE ADAPTATION IN LOCAL GOVERNANCE: INSTITUTIONAL BARRIERS IN DANISH MUNICIPALITIES Scientifi c Report from DCE – Danish Centre for Environment and EnergyNo. 104 2016 Anne Jensen Helle Ørsted Nielsen Maria Lilleøre Nielsen Aarhus University, Department of Environmental Science AARHUS AU UNIVERSITY DCE – DANISH CENTRE FOR ENVIRONMENT AND ENERGY Data sheet Series title and no.: Scientific Report from DCE – Danish Centre for Environment and Energy No. 104 Title: Climate adaptation in local governance: Institutional barriers in Danish municipalities Authors: Anne Jensen, Helle Ørsted Nielsen, Maria Lilleøre Nielsen Institution: Aarhus University, Department of Environmental Science Publisher: Aarhus University, DCE – Danish Centre for Environment and Energy © URL: http://dce.au.dk/en Year of publication: January 2016 Editing completed: December 2015 Referee: Berit Hasler Quality assurance, DCE: Anja Skjoldborg Hansen Financial support: No external financial support Please cite as: Jensen, A., Nielsen, H.Ø. & Nielsen, M.L. 2016. Climate adaptation in local governance: Institutional barriers in Danish municipalities. Aarhus University, DCE – Danish Centre for Environment and Energy, 102 pp. Scientific Report from DCE – Danish Centre for Environment and Energy No. 104 http://dce2.au.dk/pub/SR104.pdf Reproduction permitted provided the source is explicitly acknowledged Abstract: Climate change and climate adaptation constitutes a key challenge for contemporary planning and politics. In Denmark, climate adaptation policy is formulated nationally, but implemented primarily at the municipal level. This study therefore examines the ability of climate adaptation capacity of local governments, aiming to uncover institutional barriers for adaptation to climate change.