Original Article Expression of Cell-Cycle Regulators Is Associated with Invasive Behavior and Poor Prognosis in Prolactinomas
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mir-15 and Mir-16 Are Direct Transcriptional Targets of E2F1 That Limit E2F-Induced Proliferation by Targeting Cyclin E
Molecular Cancer Cell Cycle, Cell Death, and Senescence Research miR-15 and miR-16 Are Direct Transcriptional Targets of E2F1 that Limit E2F-Induced Proliferation by Targeting Cyclin E Matan Ofir, Dalia Hacohen, and Doron Ginsberg Abstract microRNAs (miR) are small noncoding RNA molecules that have recently emerged as critical regulators of gene expression and are often deregulated in cancer. In particular, miRs encoded by the miR-15a, miR-16-1 cluster seem to act as tumor suppressors. Here, we evidence that the miR-15a, miR-16-1 cluster and related miR-15b, miR-16-2 cluster comprise miRs regulated by E2F1, a pivotal transcription factor that can induce both proliferation and cell death. E2F1 is a critical downstream target of the tumor suppressor retinoblastoma (RB). The RB pathway is often inactivated in human tumors resulting in deregulated E2F activity. We show that expression levels of the 4 mature miRs, miR-15a, miR-16-1 and miR-15b, miR-16-2, as well as their precursor pri- miRNAs, are elevated upon activation of ectopic E2F1. Moreover, activation of endogenous E2Fs upregulates expression of these miRs and endogenous E2F1 binds their respective promoters. Importantly, we corroborate that miR-15a/b inhibits expression of cyclin E, the latter a key direct transcriptional target of E2F pivotal for the G1/S transition, raising the possibility that E2F1, miR-15, and cyclin E constitute a feed-forward loop that modulates E2F activity and cell-cycle progression. In support of this, ectopic expression of miR-15 inhibits the G1/S transition, and, conversely, inhibition of miR-15 expression enhances E2F1-induced upregulation of cyclin E1 levels. -

Cyclin E2, a Novel Human G1 Cyclin and Activating Partner of CDK2 and CDK3, Is Induced by Viral Oncoproteins
Oncogene (1998) 17, 2787 ± 2798 ã 1998 Stockton Press All rights reserved 0950 ± 9232/98 $12.00 http://www.stockton-press.co.uk/onc Cyclin E2, a novel human G1 cyclin and activating partner of CDK2 and CDK3, is induced by viral oncoproteins Maimoona Zariwala1, Jidong Liu2 and Yue Xiong*,1,2,3 1Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina 27599-3280; 2Department of Biochemistry and Biophysics; University of North Carolina at Chapel Hill, Chapel Hill, North Carolina 27599- 3280; 3Program in Molecular Biology and Biotechnology, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina 27599-3280, USA G1 cyclin E controls the initiation of DNA synthesis by complexes with CDK4 or CDK6 to prevent the CDKs activating CDK2, and abnormally high levels of cyclin E from binding with and becoming activated by D-type expression have frequently been observed in human cyclins. The main function of CDK inhibitors is cancers. We have isolated a novel human cyclin, cyclin believed to couple diversi®ed growth inhibitory signals E2, that contains signi®cant homology to cyclin E. to the cell cycle clock. Cyclin E2 speci®cally interacts with CDK inhibitors of The decision to enter the replicative DNA synthesis the CIP/KIP family and activates both CDK2 and (S) phase or arrest in G1 is linked to diverse cellular CDK3. The expression of cyclin E2 mRNA oscillates processes such as signal transduction, cell differentia- periodically throughout the cell cycle, peaking at the tion, senescence, and oncogenic transformation G1/S transition, and exhibits a pattern of tissue (Hunter and Pines, 1994). -

Cyclin-Dependent Kinases and CDK Inhibitors in Virus-Associated Cancers Shaian Tavakolian, Hossein Goudarzi and Ebrahim Faghihloo*
Tavakolian et al. Infectious Agents and Cancer (2020) 15:27 https://doi.org/10.1186/s13027-020-00295-7 REVIEW Open Access Cyclin-dependent kinases and CDK inhibitors in virus-associated cancers Shaian Tavakolian, Hossein Goudarzi and Ebrahim Faghihloo* Abstract The role of several risk factors, such as pollution, consumption of alcohol, age, sex and obesity in cancer progression is undeniable. Human malignancies are mainly characterized by deregulation of cyclin-dependent kinases (CDK) and cyclin inhibitor kinases (CIK) activities. Viruses express some onco-proteins which could interfere with CDK and CIKs function, and induce some signals to replicate their genome into host’scells.By reviewing some studies about the function of CDK and CIKs in cells infected with oncoviruses, such as HPV, HTLV, HERV, EBV, KSHV, HBV and HCV, we reviewed the mechanisms of different onco-proteins which could deregulate the cell cycle proteins. Keywords: CDK, CIKs, Cancer, Virus Introduction the key role of the phosphorylation in the entrance of Cell division is controlled by various elements [1–10], the cells to the S phase of the cell cycle [19]. especially serine/ threonine protein kinase complexes, CDK genes are classified in mammalian cells into differ- called cyclin-dependent kinases (CDKs), and cyclins, ent classes of CDKs, especially some important regulatory whose expression is prominently regulated by the bind- ones (The regulatory CDKs play important roles in medi- ing to CDK inhibitors [11, 12]. In all eukaryotic species, ating cell cycle). Each of these CDKs could interact with a these genes are classified into different families. It is specific cyclin and thereby regulating the expression of well-established that the complexes of cyclin and CDK different genes [20, 21]. -

Reduction of Cdc25a Contributes to Cyclin E1-Cdk2 Inhibition at Senescence in Human Mammary Epithelial Cells
Oncogene (2000) 19, 5314 ± 5323 ã 2000 Macmillan Publishers Ltd All rights reserved 0950 ± 9232/00 $15.00 www.nature.com/onc Reduction of Cdc25A contributes to cyclin E1-Cdk2 inhibition at senescence in human mammary epithelial cells Charanjit Sandhu1, Jerey Donovan1, Nandita Bhattacharya1, Martha Stampfer2, Peter Worland3 and Joyce Slingerland*,1 1Cancer Research, Sunnybrook and Women's College Health Sciences Centre, Toronto, Ontario, Canada; 2Life Sciences Division, Lawrence Berkeley Laboratory, University of California Berkeley, Berkeley, California, CA 94720, USA; 3Mitotix Incorporated, Cambridge, Massachusetts, MA 02139, USA Replicative senescence may be an important tumor a phenomenon known as cellular senescence (Hay¯ick, suppressive mechanism for human cells. We investigated 1965). Senescence may function as a tumor suppression the mechanism of cell cycle arrest at senescence in mechanism since the proliferative constraint imposed human mammary epithelial cells (HMECs) that have by senescence limits the accumulation of genetic errors undergone a period of `self-selection', and as a in the progeny of a single cell (Vojta and Barrett, consequence exhibit diminished p16INK4A levels. As 1995). The progressive reduction in telomere length HMECs approached senescence, the proportion of cells that occurs with successive cell divisions may govern with a 2N DNA content increased and that in S phase the point at which cells enter replicative senescence decreased progressively. Cyclin D1-cdk4, cyclin E-cdk2 (Bodnar et al., 1998; de Lange, 1998). Cultured human and cyclin A-cdk2 activities were not abruptly inhibited, ®broblasts show a predominantly 2N DNA content at but rather diminished steadily with increasing population senescence, re¯ecting cell cycle arrest in G1 phase age. -

Cyclin E1 and Rb Modulation As Common Events at Time of Resistance to Palbociclib in Hormone Receptor-Positive Breast Cancer
www.nature.com/npjbcancer ARTICLE OPEN Cyclin E1 and Rb modulation as common events at time of resistance to palbociclib in hormone receptor-positive breast cancer Cristina Guarducci1, Martina Bonechi1, Matteo Benelli2, Chiara Biagioni2,3, Giulia Boccalini1, Dario Romagnoli2, Roberto Verardo4, Rachel Schiff5,6,7,8, C. Kent Osborne5,6,7,8, Carmine De Angelis5,6,8, Angelo Di Leo3, Luca Malorni1,3 and Ilenia Migliaccio1 CDK4/6 inhibitors represent a new treatment standard for hormone receptor-positive (HR+), HER2-negative advanced breast cancer (BC) patients. Although efficacious, resistance to these agents is universal. Here, we profiled a large panel of HR+ BC cell lines with conditioned resistance to the CDK4/6 inhibitor palbociclib, and analyzed cell cycle-related markers by gene expression profiles (GEP) and western blot (WB). GEP showed high molecular heterogeneity among the models, with E2F targets being significantly enriched both during treatment and at the time of resistance. By both WB and GEP, a common molecular feature at the time of palbociclib resistance was the concomitant overexpression of cyclin E1 and down-regulation of Rb. CCNE1 was the only significantly up-regulated gene among E2F targets at resistance with CCNE1 genomic amplification being observed in two resistant models. Rb was downregulated in all resistant models; a reduction of RB1 copy number was observed in three resistant cell lines. In silico analyses showed that CCNE1/RB1 ratio correlated with palbociclib IC50 in different datasets of both breast and non-breast cancer cell lines, performing better than CCNE1 or RB1 taken separately. Finally, the CCNE1/RB1 ratio was shown to be an adverse prognostic factor in patients with ER+ BC and to be able to discriminate palbociclib-sensitive versus resistant among patients enrolled in the NeoPalAna trial, a neoadjuvant trial testing palbociclib, performing better than CCNE1 or RB1 alone. -

Upregulation of CDKN2A and Suppression of Cyclin D1 Gene
European Journal of Endocrinology (2010) 163 523–529 ISSN 0804-4643 CLINICAL STUDY Upregulation of CDKN2A and suppression of cyclin D1 gene expressions in ACTH-secreting pituitary adenomas Yuji Tani, Naoko Inoshita1, Toru Sugiyama, Masako Kato, Shozo Yamada2, Masayoshi Shichiri3 and Yukio Hirata Department of Clinical and Molecular Endocrinology, Tokyo Medical and Dental University Graduate School, 1-5-45, Yushima, Bunkyo-ku, Tokyo 113-8519, Japan, Departments of 1Pathology and 2Hypothalamic and Pituitary Surgery, Toranomon Hospital, Tokyo 105-8470, Japan and 3Department of Endocrinology, Diabetes and Metabolism, School of Medicine, Kitasato University, Kanagawa 252-0375, Japan (Correspondence should be addressed to Y Hirata; Email: [email protected]) Abstract Objective: Cushing’s disease (CD) is usually caused by ACTH-secreting pituitary microadenomas, while silent corticotroph adenomas (SCA) are macroadenomas without Cushingoid features. However, the molecular mechanism(s) underlying their different tumor growth remains unknown. The aim of the current study was to evaluate and compare the gene expression profile of cell cycle regulators and cell growth-related transcription factors in CD, SCA, and non-functioning adenomas (NFA). Design and methods: Tumor tissue specimens resected from 43 pituitary tumors were studied: CD (nZ10), SCA (nZ11), and NFA (nZ22). The absolute transcript numbers of the following genes were quantified with real-time quantitative PCR assays: CDKN2A (or p16INK4a), cyclin family (A1, B1, D1, and E1), E2F1, RB1, BUB1, BUBR1, ETS1, and ETS2. Protein expressions of p16 and cyclin D1 were semi-quantitatively evaluated by immunohistochemical study. Results and conclusion: CDKN2A gene expression was about fourfold greater in CD than in SCA and NFA. -

Inhibition of CDK4/6 As Therapeutic Approach for Ovarian Cancer Patients: Current Evidences and Future Perspectives
cancers Review Inhibition of CDK4/6 as Therapeutic Approach for Ovarian Cancer Patients: Current Evidences and Future Perspectives Alessandra Dall’Acqua 1,†, Michele Bartoletti 2,3,† , Nastaran Masoudi-Khoram 1,‡, Roberto Sorio 2, Fabio Puglisi 2,3 , Barbara Belletti 1 and Gustavo Baldassarre 1,* 1 Molecular Oncology Unit, Centro di Riferimento Oncologico di Aviano (CRO), IRCCS, National Cancer Institute, 33081 Aviano, Italy; [email protected] (A.D.); [email protected] (N.M.-K.); [email protected] (B.B.) 2 Medical Oncology and Cancer Prevention Molecular Oncology Unit, Centro di Riferimento Oncologico di Aviano (CRO), IRCCS, National Cancer Institute, 33081 Aviano, Italy; [email protected] (M.B.); [email protected] (R.S.); [email protected] (F.P.) 3 Department of Medicine (DAME), University of Udine, 33100 Udine, Italy * Correspondence: [email protected]; Tel.: +39-0434-659779; Fax: +39-0434-659429 † These authors equally contributed to the work. ‡ Present address: Department of Biophysics, Faculty of Biological Sciences, Tarbiat Modares University, Tehran, Iran. Simple Summary: Altered regulation of the cell cycle is a hallmark of cancer. The recent clinical success of the inhibitors of CDK4 and CDK6 has convincingly demonstrated that targeting cell cycle components may represent an effective anti-cancer strategy, at least in some cancer types. However, possible applications of CDK4/6 inhibitors in patients with ovarian cancer is still under evaluation. Citation: Dall’Acqua, A.; Bartoletti, M.; Masoudi-Khoram, N.; Sorio, R.; Here, we describe the possible biological role of CDK4 and CDK6 complexes in ovarian cancer and Puglisi, F.; Belletti, B.; Baldassarre, G. provide the rationale for the use of CDK4/6 inhibitors in this pathology, alone or in combination Inhibition of CDK4/6 as Therapeutic with other drugs. -

D3-Deficient Mice Is Compensated by Cyclin D2 in Cyclin of Normal B-1A
Disruption of Cyclin D3 Blocks Proliferation of Normal B-1a Cells, but Loss of Cyclin D3 Is Compensated by Cyclin D2 in Cyclin D3-Deficient Mice This information is current as of September 28, 2021. Jennifer M. Mataraza, Joseph R. Tumang, Maria R. Gumina, Sean M. Gurdak, Thomas L. Rothstein and Thomas C. Chiles J Immunol 2006; 177:787-795; ; doi: 10.4049/jimmunol.177.2.787 Downloaded from http://www.jimmunol.org/content/177/2/787 References This article cites 51 articles, 21 of which you can access for free at: http://www.jimmunol.org/ http://www.jimmunol.org/content/177/2/787.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 28, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2006 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Disruption of Cyclin D3 Blocks Proliferation of Normal B-1a Cells, but Loss of Cyclin D3 Is Compensated by Cyclin D2 in Cyclin D3-Deficient Mice1 Jennifer M. -

Early Adaptation and Acquired Resistance to CDK4/6 Inhibition In
Published OnlineFirst March 28, 2016; DOI: 10.1158/0008-5472.CAN-15-0728 Cancer Therapeutics, Targets, and Chemical Biology Research Early Adaptation and Acquired Resistance to CDK4/6 Inhibition in Estrogen Receptor–Positive Breast Cancer Maria Teresa Herrera-Abreu1, Marta Palafox2, Uzma Asghar1, Martín A. Rivas3, Rosalind J. Cutts1, Isaac Garcia-Murillas1, Alex Pearson1, Marta Guzman2, Olga Rodriguez2, Judit Grueso2, Meritxell Bellet4, Javier Cortes 4, Richard Elliott1, Sunil Pancholi1, Jose Baselga5, Mitch Dowsett1,6, Lesley-Ann Martin1, Nicholas C. Turner1,7, and Violeta Serra2 Abstract Small-molecule inhibitors of the CDK4/6 cell-cycle kinases apy, CDK4/6, and PI3K inhibition was more effective than have shown clinical efficacy in estrogen receptor (ER)-positive paired combinations, provoking rapid tumor regressions in a metastatic breast cancer, although their cytostatic effects are PDX model. Mechanistic investigations showed that acquired limited by primary and acquired resistance. Here we report that resistance to CDK4/6 inhibition resulted from bypass of cyclin ER-positive breast cancer cells can adapt quickly to CDK4/6 D1–CDK4/6 dependency through selection of CCNE1 ampli- inhibition and evade cytostasis, in part, via noncanonical cyclin fication or RB1 loss. Notably, although PI3K inhibitors could D1-CDK2–mediated S-phase entry. This adaptation was pre- prevent resistance to CDK4/6 inhibitors, they failed to resen- vented by cotreatment with hormone therapies or PI3K inhi- sitize cells once resistance had been acquired. However, we bitors, which reduced the levels of cyclin D1 (CCND1)and found that cells acquiring resistance to CDK4/6 inhibitors due other G1–S cyclins, abolished pRb phosphorylation, and inhib- to CCNE1 amplification could be resensitized by targeting ited activation of S-phase transcriptional programs. -

Cyclin E1, GST-Tagged, Human (SRP5345)
Cyclin E1, GST-tagged, human recombinant, expressed in Sf9 cells Catalog Number SRP5345 Storage Temperature –70 °C Synonyms: CCNE1, CCNE Figure 1. SDS-PAGE Gel of Typical Lot: Product Description ³70% (SDS-PAGE, densitometry) Cyclin E1 belongs to the highly conserved cyclin family, whose members are characterized by a dramatic periodicity in protein abundance through the cell cycle that functions as regulators of CDK kinases. Cyclin E1 activity is required for centrosome duplication during S phase and this mechanism could coordinate centrosome reproduction with cycles of DNA synthesis and mitosis.1 The downregulation of cyclin E-CDK2 kinase activity following the G1/S-phase transition is necessary for the maintenance of karyotypic stability. Cyclin E also has a modular centrosomal-targeting Precautions and Disclaimer domain, which is essential for promoting S phase entry 2 This product is for R&D use only, not for drug, in a Cdk2-independent manner. household, or other uses. Please consult the Material Safety Data Sheet for information regarding hazards Recombinant full-length human Cyclin E1 was and safe handling practices. expressed by baculovirus in Sf9 insect cells using an N-terminal GST-tag. The gene accession number is Storage/Stability NM_001238. It is supplied in 50 mM Tris-HCl, pH 7.5, The product ships on dry ice and storage at –70 °C is 150 mM NaCl, 10 mM glutathione, 0.1 mM EDTA, recommended. After opening, aliquot into smaller 0.25 mM DTT, 0.1 mM PMSF, and 25% glycerol. quantities and store at –70 °C. Avoid repeated handling and multiple freeze/thaw cycles. -
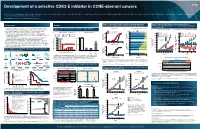
Development of a Selective CDK2-E Inhibitor in CCNE-Aberrant Cancers 1279
Development of a selective CDK2-E inhibitor in CCNE-aberrant cancers 1279 Yoon J. Choi1, Steve Wenglowsky1 , Victoria Brown1 , Neil Bifulco1, Yeon S. Choi1, Jian Guo1, Megan Hatlen1, Joseph Kim1, Tim LaBranche1, Riadh Lobbardi1, Emanuele Perola1, Emily Rozsahegyi1, Michelle Maynard1, Phil Ramsden1, Grace Silva1, Faith Stevison1, Richard Vargas1, Ruduan Wang1, Doug Wilson1, Rich Woessner1, Dean Zhang1, Rob Meissner1, Klaus Hoeflich1, Marion Dorsch1 1Blueprint Medicines Corporation, Cambridge, Massachusetts, USA Figure 5: Selective CDK2 inhibitor, BLU0298 selectively inhibits (A) Figure 7: Selective CDK2 inhibitor achieves similar efficacy to 1296P Background Results proliferation in CCNE1-amplified cells by (B) arresting cells in G1/S PF-06873600, a CDK2/4/6 inhibitor, or to chemotherapy, but maintains stable body weight • Cyclin E1 and E2 are core cell cycle regulators, that when bound activate CDK2 Figure 3: CDK2 catalytic activity is essential in CCNE1-amplified A. Proliferation B. Cell cycle profile in OVCAR-3 cells 1 A. In vivo efficacy in OVCAR-3 B. BLU1954-treated mice maintained healthy BW (cyclin-dependent kinase 2), driving G1/S progression of the cell cycle (Figure 1A) cell lines [nM] G1 S G2/M • A broad range of aggressive cancers overexpress and/or harbor CCNE gene OVCAR-3 CCNE1-AMP amplifications, thus CDK2 is a potentially impactful therapeutic target A. Genetic validation of dependency B. Catalytic dependency 100 TOV-21G CCNE1 WT 25 4000 Vehicle 15 Vehicle PO BID (28 Days) – In subsets of gynecological, breast, gastric, and other cancers, CCNE amplification 1. TOV21G 4. HCC1569 7. KURAMOCHIa BLU1954 100 mg/kg QD BLU1954 100 mg/kg PO QD (28 Days) correlates with overexpression (Figure 1B)2 and has been associated with poor survival in 2. -

Cyclin E2 Promotes Whole Genome Doubling in Breast Cancer
cancers Article Cyclin E2 Promotes Whole Genome Doubling in Breast Cancer Christine Lee 1, Kristine J. Fernandez 1, Sarah Alexandrou 1,2, C. Marcelo Sergio 1 , Niantao Deng 1,2, Samuel Rogers 3,4, Andrew Burgess 5,6 and C. Elizabeth Caldon 1,2,* 1 The Kinghorn Cancer Centre, Garvan Institute of Medical Research, Sydney, NSW 2010, Australia; [email protected] (C.L.); [email protected] (K.J.F.); [email protected] (S.A.); [email protected] (C.M.S.); [email protected] (N.D.) 2 St. Vincent’s Clinical School, Faculty of Medicine, UNSW Sydney, Sydney, NSW 2052, Australia 3 Children’s Medical Research Institute, The University of Sydney, Westmead, NSW 2145, Australia; [email protected] 4 Faculty of Medicine and Health, University of Sydney, Sydney, NSW 2006, Australia 5 ANZAC Research Institute, Concord, NSW 2139, Australia; [email protected] 6 The University of Sydney Concord Clinical School, Faculty of Medicine and Health Concord, Sydney, NSW 2139, Australia * Correspondence: [email protected]; Tel.: + 612-9355-5878; Fax: +612-9295-8110 Received: 5 July 2020; Accepted: 4 August 2020; Published: 13 August 2020 Abstract: Genome doubling is an underlying cause of cancer cell aneuploidy and genomic instability, but few drivers have been identified for this process. Due to their physiological roles in the genome reduplication of normal cells, we hypothesised that the oncogenes cyclins E1 and E2 may be drivers of genome doubling in cancer. We show that both cyclin E1 (CCNE1) and cyclin E2 (CCNE2) mRNA are significantly associated with high genome ploidy in breast cancers.