Draft Outline
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anloung Lvea Primary School E Ducation
B roadening A ccess to S ustainable Anloung Lvea Primary School E ducation Facts Description Name Anloung Lvea In spite of its flourishing tourism, Cambodia is still one of the poorest and least developed countries in Southeast Type of facility Primary School Asia. Development is not evenly distributed in the country and many rural communities remain poverty-stricken No. of students 145 (63 boys, 82 girls) as corruption and self-interest impedes the country’s growth. Anloung Lvea Primary School is located in Sangkae No. of teachers 6 (3 male, 3 female) District of Battambang Province. The local community has a population of 1,432, where the main source of No. of classrooms 1 school building with 4 income originates from subsistence farming. The school offers education from Primary 1 to Primary 6, and has classrooms & 1 toilet 145 students, aged 6 – 12, in attendance. The current school building was constructed in 1995 and is now under Size of building 288 m2 great risk of collapsing. Due to the potential of the building falling apart on students, classes were relocated to a Budget USD 49,045 local villager’s basement. With insufficient space and little protection from the rain and dust, students cannot Construction period May - December 2015 fully benefit from their education in such a restrictive environment. By providing a new school building with four Project manager Mr. Sinoeuy My fully furnished classrooms, we will be addressing the lack of proper school infrastructure, enabling children to Location (Province) Anloung Lvea Village, learn and grow in real and safe classrooms. -

Appendix J.2.3)
Supplementary Appendix H.1 NORTHWEST IRRIGATION SECTOR PROJECT LINK CANAL SUBPROJECT RESETTLEMENT PLAN List of Contents Page 1. The Project 3 2. Impact on Structures and Land Acquisition 4 3. Mitigating Project Impact 5 4. Socio-Economic Situation in the Project Area. 6 4.1 Project Socioeconomic Surveys 6 4.2 Socio-Economic Characteristics Of The Wider Project Area 6 5. Objectives, Policy Framework and Entitlements 16 6. Mitigating Impact and Ensuring the Restoration of Livelihoods of APs 18 7. Participation, Information and Consultation and Grievance Redress 21 7.1 AP Participation 21 7.2 Disclosure of Information to APs 21 7.3 The Grievance Process 22 8. Management and Organisation 24 9. Resettlement Budget 26 10.Implementation Schedule 28 11.Monitoring and Evaluation 28 List of Tables: Number Title Page No. 3.1 Development Agents Working in Area 7 4.1 Demographics of Subproject Area 8 4.2 Village Demographics 8 4.3 Age-Sex distribution of APs 9 4.4 Size of AP households 9 4.5 Incidence of Overall Poverty in Subproject Area 9 4.6 APs Deficit in rice production for household 9 4.7 APs Duration of Rice Deficit last year (months) 9 4.8 Literacy of household head and spouse 10 i Supplementary Appendix H.1 4.9 School attendance of children of primary school age 10 4.10 Reason for non-attendance school 10 4.11 Attendance of school age children: Lower secondary 10 4.12 Reason for non-attendance at secondary school 10 4.13 Village Land, Farming System, Non-Farming Occupations and Mines or UXO Pesence 12 4.14 Bavel District, Kdol Commune, Villages -
DC-Cam 2015 Annual Report
mCÄmNÐlÉkßrkm<úCa DOCUMENTATION CENTER OF CAMBODIA Phnom Penh, Cambodia DC-Cam Annual Report: January 1, 2015-December 31, 2015 Prepared and Compiled by Dr. Kok-Thay ENG and Dara VANTHAN Deputy Directors Edited by Cindy Coleman SRI Board Meeting at Stanford University Second from left Professor Ron Slye, Professor John Ciorciari, Professor Jaya Ramji-Nogales, Professor Beth van Schaack, Youk Chhang, and Dr. Markus Zimmer Documentation Center of Cambodia Searching for the Truth: Memory & Justice EsVgrkKrBitedIm, IK rcg©MnigyutþiFm‘’ 66 Preah Sihanouk Blvd.P.O.Box 1110Phnom PenhCambodia t(855-23) 211-875f (855-23) 210-358 [email protected] www.dccam.org TABLE OF CONTENTS DOCUMENTATION CENTER OF CAMBODIA ............................................................................... 1 TABLE OF CONTENTS ........................................................................................................................ 2 ACRONYMS ................................................................................................................................ 3 Summary .................................................................................................................................... 4 AUGMENT AND MAINTAIN A PUBLICALLY ACCESSIBLE HISTORICAL RECORD OF THE KR PERIOD ...................... 4 SUPPORT THE KRT .......................................................................................................................... 5 INCREASE CAMBODIA’S PUBLIC KNOWLEDGE OF THE KR PERIOD ............................................................. -

44321-013: Climate Resilient Rice Commercialization Sector
Initial Environmental Examination Project Number: 44321-013 November 2019 Cambodia: Climate Resilient Rice Commercialization Sector Development Program Loans 3006/3007/8271-CAM Grants 0349/0350-CAM Prepared by Ministry of Economy and Finance for the Royal Government of Cambodia and the Asian Development Bank. This initial environmental examination is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. KINGDOM OF CAMBODIA Nation Religion King Ministry of Economy and Finance Climate-Resilient Rice Commercialization Sector Development Program ADB Loans 3006/3007/8271 and Grants 0349/0350-CAM Initial Environmental Examination for Establishment of Paddy Drying and Storage Facility at Phou Poy Rice Mill in Chumnik Village, Anlong Vil Commune, Sangkae District, Battambang Province November 2019 CURRENCY EQUIVALENTS (November 2019) Currency Unit – riel (KR) KR1.00 = $0.00025 $1.00 = KR4, 000 ABBREVIATIONS ADB Asian Development Bank CLAC Commune Land Acquisition Committee DD & CS Detailed Design and Construction Supervision EHS Environmental, Health and Safety EIA Environmental Impact Assessment EMP Environmental Management Plan -

A Future for Cambodia's Children: My Journey to the Villages of Battambang Cerise Fritsch
Public Interest Law Reporter Volume 13 Article 6 Issue 2 Spring 2008 2008 A Future for Cambodia's Children: My Journey to the Villages of Battambang Cerise Fritsch Follow this and additional works at: http://lawecommons.luc.edu/pilr Part of the Human Rights Law Commons Recommended Citation Cerise Fritsch, A Future for Cambodia's Children: My Journey to the Villages of Battambang, 13 Pub. Interest L. Rptr. 141 (2008). Available at: http://lawecommons.luc.edu/pilr/vol13/iss2/6 This Article is brought to you for free and open access by LAW eCommons. It has been accepted for inclusion in Public Interest Law Reporter by an authorized administrator of LAW eCommons. For more information, please contact [email protected]. Fritsch: A Future for Cambodia's Children: My Journey to the Villages of B No. 2 * Spring 2008 A FUTURE FOR CAMBODIA'S CHILDREN: MY JOURNEY TO THE VILLAGES OF BATTAMBANG by CERISE FRITSCH my knowledge of the school in the United States and M lawsy first affecting year of lawchildren in conflict with the law in Cambodia proved inadequate in preparing me for my journey to the northeastern villages of Cambodia, a country marked by a history of civil war, turmoil and genocide by the Khmer Rouge. In a Battambang Province court room, a 9-year-old boy sat next to his brother, swaying his feet back and forth. He appeared small for his age, his clothes were torn and stained, his bare feet were infected with sores, and his head 141 Published by LAW eCommons, 2008 1 Public Interest Law Reporter, Vol. -

Cambodia PRASAC Microfinance Institution
Maybank Money Express (MME) Agent - Cambodia PRASAC Microfinance Institution Branch Location Last Update: 02/02/2015 NO NAME OF AGENT REGION / PROVINCE ADDRESS CONTACT NUMBER OPERATING HOUR 1 PSC Head Office PHNOM PENH #25, Str 294&57, Boeung Kengkang1,Chamkarmon, Phnom Penh, Cambodia 023 220 102/213 642 7.30am-4pm National Road No.5, Group No.5, Phum Ou Ambel, Krong Serey Sophorn, Banteay 2 PSC BANTEAY MEANCHEY BANTEAY MEANCHEY Meanchey Province 054 6966 668 7.30am-4pm 3 PSC POAY PET BANTEAY MEANCHEY Phum Kilometre lek 4, Sangkat Poipet, Krong Poipet, Banteay Meanchey 054 63 00 089 7.30am-4pm Chop, Chop Vari, Preah Net 4 PSC PREAH NETR PREAH BANTEAY MEANCHEY Preah, Banteay Meanchey 054 65 35 168 7.30am-4pm Kumru, Kumru, Thmor Puok, 5 PSC THMAR POURK BANTEAY MEANCHEY Banteay Meanchey 054 63 00 090 7.30am-4pm No.155, National Road No.5, Phum Ou Khcheay, Sangkat Praek Preah Sdach, Krong 6 PSC BATTAMBANG BATTAMBANG Battambang, Battambang Province 053 6985 985 7.30am-4pm Kansai Banteay village, Maung commune, Moung Russei district, Battambang 7 PSC MOUNG RUESSEI BATTAMBANG province 053 6669 669 7.30am-4pm 8 PSC BAVEL BATTAMBANG Spean Kandoal, Bavel, Bavel, BB 053 6364 087 7.30am-4pm Phnom Touch, Pech Chenda, 9 PSC PHNOM PROEK BATTAMBANG Phnum Proek, BB 053 666 88 44 7.30am-4pm Boeng Chaeng, Snoeng, Banan, 10 PSC BANANN BATTAMBANG Battambang 053 666 88 33 7.30am-4pm No.167, National Road No.7 Chas, Group No.10 , Phum Prampi, Sangkat Kampong 11 PSC KAMPONG CHAM KAMPONG CHAM Cham, Krong Kampong Cham, Kampong Cham Province 042 6333 000 7.30am-4pm -

Community Self-Reliance and Flood Risk Reduction (Financed by the Poverty Reduction Cooperation Fund)
Technical Assistance Consultant’s Report Project Number: 37290 September 2007 Kingdom of Cambodia: Community Self-Reliance and Flood Risk Reduction (Financed by the Poverty Reduction Cooperation Fund) Prepared by Asian Disaster Preparedness Center Bangkok, Thailand For Ministry of Water Resources and Meteorology This consultant’s report does not necessarily reflect the views of ADB or the Government concerned, and ADB and the Government cannot be held liable for its contents. Table of Contents A Background of the TA………………………………………………………………………...03 B Executive Summary of significant activities under the project……………………....05 C Details for each activity under the two phases of the TA………………………………08 1. Designing the community participation model…………………………………………09 1.1 Understanding NGO interventions in Flood Risk Reduction 1.1.1 Description of NGO projects in Cambodia 1.1. 2 NGO projects on flood risk reduction in 4 TA target provinces 1.1. 3 NGO approaches to flood risk reduction 1.1.4 Typical constraints to effectiveness of NGO interventions 1.2 Developing a simple GIS……………………………………………………………………21 1.2.1 Development of a Flood Vulnerability GIS Application 1.2.2 Flood vulnerability GIS – Atlas Interpretation Guide 1.2.3 GIS Maps for ready reference 1.3 Undertaking a brief survey within target provinces for identifying key community needs in flood and drought risk reduction………………………………………………………26 1.4 Identification of target areas and prioritizing areas for future interventions……..27 1.5 Selecting NGOs for undertaking pilot community based flood risk reduction action in the target areas identified………………………………………………………………………28 1.6 Developing a Community Based Disaster Risk Reduction (CBDRR) Strategy……29 1.7 Workshop on CBDRR Strategy…………………………………………………………….33 1.7.1 Consultative workshop on CBDRR Strategy 1.7.2 6th Meeting of the Cambodia Disaster Risk Reduction Forum 2. -

Correspondence with the Cambodian Government
H U M A N “They Treat Us Like Animals” R I G H T S Mistreatment of Drug Users and “Undesirables” in Cambodia’s WATCH Drug Detention Centers “They Treat Us Like Animals” Mistreatment of Drug Users and “Undesirables” in Cambodia’s Drug Detention Centers Copyright © 2013 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-62313-0817 Cover design by Rafael Jimenez Human Rights Watch is dedicated to protecting the human rights of people around the world. We stand with victims and activists to prevent discrimination, to uphold political freedom, to protect people from inhumane conduct in wartime, and to bring offenders to justice. We investigate and expose human rights violations and hold abusers accountable. We challenge governments and those who hold power to end abusive practices and respect international human rights law. We enlist the public and the international community to support the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org DECEMBER 2013 978-1-62313-0817 “They Treat Us Like Animals” Mistreatment of Drug Users and “Undesirables” in Cambodia’s Drug Detention Centers Map 1: Closed Drug Detention Centers and the Planned National Center .............................. i Map 2: Current Drug Detention Centers in Cambodia .......................................................... ii Summary ........................................................................................................................... 1 Recommendations .............................................................................................................. 7 To the Government of Cambodia .............................................................................................. -
!I !I !I !I !I !I !I
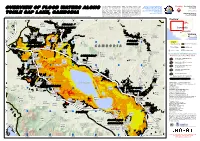
This map presents potential standing waters is uncertain because of the Disaster coverage by the International Flooding Production Date: flood waters/ flood affected land over relatively low spatial resolution of the Charter 'Space and Major Disasters'. For 10/11/2011 the affected area surrounding Tonle satellite sensors used for this analysis, more information on the Charter, which is Sap Lake, Cambodia following recent Detected water bodies likely reflect an about assisting the disaster relief heavy rainy season. This analysis underestimation of all flood-affected organizations with multi-satellite data and Version 2.0 information, visit !, indicates that flood waters have areas within the map extent. This www.disasterscharter.org ! expanded in the lake area between 28 analysis has not yet been validated in UNOSAT Activation: August and 27th October 2011. Please the field. Please send ground feedback FL20111012KHM Flood Analysis with ENVISAT ASAR WSM imagery recorded on 28 August, 27 & 30 September, 27 October 2011 over Tonle Sap Lake, Cambodia note that the exact limit of the flood!( to UNITAR / UNOSAT. !( !( 102°55'0"E 103°20'0"E 103°45'0"E !( 104°10'0"E 104°35'0"E 105°0'0"E Thailand !( !( ¤£348 !( Map !( !( Prasat Phumi Extent !( !( Banteay Char !( Chhmar !( Phumi !( Cambodia Phumi Thnong !(Skov !( Khang Cheung PHNOM PENH !( !( ¥¦¬ Phumi!( 68 !( ¤£ Treas !( Phumi Vietnam !( !( !( !( !( Svay !( Pou PHUMI !( Roessei Ho Chi Minh City !( Phumi Phumi !(Kulen !( !( Chek 68 Sre Noy MLU PREY!( !(!( ¤£ !(Thum !( Bahal !( Pheas Phumi !( !( -
Activity Report
Kingdom of Cambodia The Project for Strengthening Capacity for Maintenance of Roads and Bridges Activity Report February 2018 MINISTRY OF PUBLIC WORKS AND TRANSPORTS JAPAN INTERNATIONAL COOPERATION AGENCY Location Map List of Abbreviation AC Asphalt Concrete ADB Asian Development Bank AusAID Australian Agency for International Development BOQ Bill of Quantities C/P Counter Part CAMRA Cambodia Road Association CAMTA Cambodia Truck Association CD Critical Damage CDC Council for the Development of Cambodia CFC Carbon Fiber Cloth CTIE CTI Engineering Co.Ltd., CTII CTI Engineering International Co.Ltd., D Damaged DB Database DBST Double Bituminous Surface Treatment DPWT Provincial Department of Public Works and Transport DRIMS Dynamic Response Intelligent Monitoring System DTC Department of Technical and Transport EC Executing Committee EOJ Embassy of Japan EXMID Expressway and Mega Bridge and Investment Department FWD Falling Weight Defelectometer FY Fiscal Year GDI General Department of Inspection GDPW General Department of Public Works GIS Geological Information System GMS Greater Mekong Subregion GOC Government of Cambodia GPS Global Positioning System HDM4 Highway Development and Maintenance. Management System 4 HEC Heavy Equipment Center HERCD Heavy Equipment and Road Construction Department HSWIM High Speed Weigh in Motion, Fast WIM HV Heavy Vehicle IDA International Development Association IRI International Roughness Index ITC Institute of Technology of Cambodia JCC Joint Coordination Committee JCI Japan Concrete Institute JICA Japan -

Location Map of Flood Damaged Rural Roads in Kampong Cham Province
Project Number: 46009-001 October 2012 Cambodia: Flood Damage Emergency Reconstruction Project Location Map of Flood Damaged Rural Roads in Kampong Cham Province Prepared by: Ministry of Rural Development By making any designation of or reference to a particular territory or geographical area, or by using the term "country" in the website, ADB does not intend to make any judgment as to the legal or other status of any territory or area. Boundaries, colors, denominations or any other information shown on maps do not imply, on the part of ADB, any judgment on the legal status of any territory, or any endorsement or acceptance of such boundaries, colors, denominations, or information. Location Map of Flood Damaged Rural Roads in Kampong Cham Province 480000 487500 495000 502500 510000 517500 525000 532500 540000 547500 555000 562500 570000 577500 585000 592500 600000 607500 615000 622500 630000 637500 645000 652500 660000 m Tho 1375000 g 1375000 pon #0 Legend Kam #0 Tuol Sambuor #0 Ou Mlu Ta Prok #0 #0 Flood Damaged Rural Road 1367500 1367500 Dang Kdar Areaks Tnaot #0 #0 Cheyyou National Roads Chamkar Andoung Lvea Leu #0#0 2 1$ Spueu 2 2 tu K #0 #0 Krouch#0 Chhmar#0 Preah Andoung ra Ckhum 1360000 Chamkar#0 Leu t 1360000 Me Sar Chrey #0 1$Peam Kaoh#0 Sna #0 ie Svay Teab Krouch Chhmar #0 Preaek Kak #0 Khpob Ta Nguon Roka Khnaor 1$ Csrok Soupheas 1$ Svay Khleang#0 2 #0 #0 #0C #0 1 K tu7#0 Stueng TrangTrea Peus Pir UV Chumnik Peus Muoy .! Ckhet 1352500 1352500 Ta Ong #0 Tuol Preah Khleang #0 #0 Water way #0 Preaek Bak #0 #0 Preaek a Chi Sampong -
Resettlement Categorization Report (CW08)
Uplands Irrigation and Water Resources Management Sector Project ADB Loan No. 3289 CAM (SF) MOWRAM Prek Chik Secondary Canal Package 2 KINGDOM OF CAMBODIA Nation Religion King MINISTRY OF WATER RESOURCE AND METHODOLOGY ASIAN DEVELOPMENT BANK ADB Loan No 3289-CAM UPLANDS IRRIGATION AND WATER RESOURCES MANAGEMENT SECTOR PROJECT, CAMBODIA (MOWRAM-CW08)/ Upgrading, modernizing and extending the secondary and tertiary canals of Prek Chik (PC) irrigation system in Battambang RESETTLEMENT CATEGORIZATION REPORT CW08 - PREK CHIK SECONDARY CANAL PACKAGE 2 December 2016 1 Uplands Irrigation and Water Resources Management Sector Project ADB Loan No. 3289 CAM (SF) MOWRAM Prek Chik Secondary Canal Package 2 CONTENTS I. INTRODUCTION ..................................................................................................... 1 A Background................................................................................................... 1 II. SUB-PROJECT DESCRIPTION ............................................................................. 1 A Location......................................................................................................... 1 B Scope of Works ............................................................................................ 4 C Sub-project Screening and Classification ................................................. 5 FIGURES & TABLES FIGURE 1 SUB-PROJECT LOCATION ............................................................................... .2 FIGURE 2 SUB-PROJECT LOCATION PLAN .....................................................................