ESPN Thematic Report on Inequalities in Access to Healthcare
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Swedish Foreign Fighters in Syria and Iraq
Swedish Foreign Fighters in Syria and Iraq An Analysis of open-source intelligence and statistical data Linus Gustafsson Magnus Ranstorp Swedish Foreign Fighters in Syria and Iraq An analysis of open-source intelligence and statistical data Swedish Foreign Fighters in Syria and Iraq An analysis of open-source intelligence and statistical data Authors: Linus Gustafsson Magnus Ranstorp Swedish Defence University 2017 Swedish Foreign Fighters in Syria and Iraq: An analysis of open-source intelligence and statistical data Linus Gustafsson & Magnus Ranstorp © Swedish Defence University, Linus Gustafsson & Magnus Ranstorp 2017 No reproduction, copy or transmission of this publication may be made without written permission. Swedish material law is applied to this book. The contents of the book has been reviewed and authorized by the Department of Security, Strategy and Leadership. Printed by: Arkitektkopia AB, Bromma 2017 ISBN 978-91-86137-64-9 For information regarding publications published by the Swedish Defence University, call +46 8 553 42 500, or visit our home page www.fhs.se/en/research/internet-bookstore/. Summary Summary The conflict in Syria and Iraq has resulted in an increase in the number of violent Islamist extremists in Sweden, and a significant increase of people from Sweden travelling to join terrorist groups abroad. Since 2012 it is estimated that about 300 people from Sweden have travelled to Syria and Iraq to join terrorist groups such as the Islamic State (IS) and, to a lesser extent, al-Qaeda affiliated groups such as Jabhat al-Nusra. Even though the foreign fighter issue has been on the political agenda for several years and received considerable media attention, very little is known about the Swedish contingent. -

Expert Talk Al-Shabaab's Tentacles Extend West
SEPTEMBER 2009 Expert Talk Al-Shabaab’s Tentacles Extend West by John Solomon, Head of Terrorism Research, World-Check Newsletter by World-Check, the recognised authority on reducing risk through intelligence. www.world-check.com/experttalk n recent months the US-Pakistan offensive on al-Qa’ida and the Taliban in the tribal areas of Pakistan has intensified I significantly. With the future of that terrorist sanctuary now in question, Waziristan in the Federally Administered Tribal Areas of Pakistan has been diminished in many would-be jihadists eyes as the premier destination for those seeking to join al-Qa’ida. The dimming of Waziristan has coincided with the elevation of Somalia as an alternative destination and hub for global jihad. The toll of the violence and instability on locals has been significant. Since the start Al-Shabaab of 2007, the fighting in Somalia has killed more than 18 000 people and displaced The al-Qa’ida-linked al-Shabaab 1.2 million civilians. Since May of this year alone, over 100 000 civilians have been movement is the key terrorist forced to flee their homes due to the shelling of civilian areas. And according to group operating in Somalia. the UNHCR, the UN refugee agency, some 300 000 have fled to camps in Dadaab The group was formed from in Kenya. For al-Shabaab, the instability sowed by conflict and state failure provides the former youth wing of it with a safe haven for its terrorist activities, which have international dimensions. the defunct Union of Islamic Courts and is ideologically While the Somali jihadist group operates mainly in a localized context, it has and operationally aligned with become increasingly globalised. -

Political Participation of Refugees the Case of Syrian and Somali Refugees in Sweden Political Participation of Refugees
Political Participation of Refugees The Case of Syrian and Somali Refugees in Sweden Political Participation of Refugees The Case of Syrian and Somali Refugees in Sweden Tarig Adan Lina Antara (series editor) As part of the Refugees, Asylum Seekers and Democracy project, this case study was made possible by funding from the Robert Bosch Stiftung. © 2018 International Institute for Democracy and Electoral Assistance International IDEA publications are independent of specific national or political interests. Views expressed in this publication do not necessarily represent the views of International IDEA, its Board or its Council members. The electronic version of this publication is available under a Creative Commons Attribute-NonCommercialShareAlike 3.0 (CC BY-NC-SA 3.0) licence. You are free to copy, distribute and transmit the publication as well as to remix and adapt it, provided it is only for non-commercial purposes, that you appropriately attribute the publication, and that you distribute it under an identical licence. For more information on this licence visit the Creative Commons website: <http://creativecommons.org/licenses/by-nc-sa/3.0/>. International IDEA Strömsborg SE–103 34 Stockholm Telephone: +46 8 698 37 00 Email: [email protected] Website: <http://www.idea.int> Cover illustration: Joshua Sowah Design and layout: International IDEA ISBN: 978-91-7671-162-0 Created with Booktype: <https://www.booktype.pro> International IDEA Contents Abbreviations ............................................................................................................................... -

In the Ghetto
SWEDEN IN THE GHETTO ©Alessandro Gandolfi Overview of Stockholm’s residential district of Kista, with the Husby district on the far right and, on the left, Tensta and Rinkeby neighbourhoods In Sweden, Rinkeby is a symbol. In this district located at the north of Stockholm the 95% of people come from abroad. It’s a kaleidoscope of 60 ethnic groups and 40 different languages: there are people from Somalia, Iraq, Syria but even from Lebanon, Ethiopia, Turkey, Bosnia, Romania, Bengal, Peru. In Sweden, places like Rinkeby are scaring: locals avoid them, the news picture them as dangerous. Rinkeby, Tensta, Husby, Akulla are real ghettos, born in the Sixties of last century to host Swedish workers and then house to political refugees. Here unemployment shows an high percentage and petty crimes are huge, still Rinkeby is a golden, Ikea style ghetto: there are public libraries, green gardens with playgrounds for kids, clean roads, good schools and public transports. It’s an area where the word multicultural means exchange, creativity, new energies expressing themselves through art and music. Rinkeby is an interesting cohabitation lab, a “world village” mirroring a new country. Sweden never really faced integration matters and now – with almost 2 millions strangers out of 10 millions of residents – discover itself vaguely intolerant. The Swedish extrem right party, called ‘Sverigedemokraterna’ reached the 15% at the last election, making Sweden a country where a stranger start to be seen as a danger and no more as a resource. Tensta (Sweden), a Pentecostal Church Sunday service held in the city hall Rinkeby (Sweden), Akram Hassam, 15 yo, from Eritrea, grief over a missed goal during a football match Skogås (Sweden), the Devotion performs in a community centre of the district. -

SWEDEN and Literature Survey
Muslims in the EU: Cities Report Preliminary research report SWEDEN and literature survey 2007 Researcher: Dr Göran Larsson, Department of Religious Studies, Theology and Classical Philology, University of Göteborg, Sweden Email address: [email protected] Table of Contents Background 4 Executive Summary 5 PART I: RESEARCH AND LITERATURE ON MUSLIMS 8 1. Population 8 1.1 Availability of data on Muslims in Sweden 8 1.2 Muslim population estimates 9 1.3 The main waves of Muslim immigration to Sweden 12 1.4 Patterns of settlement 14 2. Identity 15 2.1 Muslim ethnic identities in Sweden 15 2.2 Religious identities 15 2.3 Converts to Islam 16 2.4 Muslim female identity 17 2.5 Other areas of research 18 3. Education 19 3.1 Muslims and the Swedish education system 19 3.2 Muslims and educational attainment 19 3.3 Religious education in schools 21 3.4 Independent Islamic schools 21 3.5 Education programmes for the training of imams 23 4. Employment 24 4.1 Access to the labour market for people in Sweden born outside the EU 24 4.2 Discrimination in the labour market and other barriers to employment 25 5. Housing 27 5.1 The housing situation of Muslims in Sweden 27 6. Health and social protection 29 6.1 The health status of Muslims 29 7. Policing and security 31 7.1 Muslims’ experiences in the army 31 7.2 Muslims’ experiences in relation to criminal justice and policing 31 8. Participation and citizenship 33 8.1 Muslim participation in politics and policy-making 33 PART II: POLICY CONTEXT 35 1. -

Delivery of Immunization Services for Refugees and Migrants Technical Guidance the Migration and Health Programme
Delivery of immunization services for refugees and migrants Technical guidance The Migration and Health programme The Migration and Health programme, the first fully fledged programme on migration and health within WHO was established at the WHO Regional Office for Europe to support Member States to strengthen the health sector’s capacity to provide evidence- informed responses to the public health challenges of refugee and migrant health. The programme operates under the umbrella of the European health policy framework Health 2020, providing support to Member States under four pillars: technical assistance; health information, research and training; partnership building; and advocacy and communication. The programme promotes a collaborative intercountry approach to migrant health by facilitating cross-country policy dialogue and encouraging homogeneous health interventions along the migration routes to promote the health of refugees and migrants and protect public health in the host community. Delivery of immunization services for refugees and migrants Technical guidance Abstract This technical guidance outlines current best practice, evidence and knowledge in order to support policy and programme development for vaccination of refugees and migrants in the WHO European Region. It highlights key principles, summarizes priority actions and challenges, maps available resources and tools, and provides practical policy considerations to improve vaccination coverage and immunization service delivery for these groups. In particular, it highlights the provision of immunization services to newly arrived refugees and migrants, the incorporation of routine delivery of immunization for refugees and migrants into mainstream health services, and tailoring of programmes for more targeted delivery. The intended audience includes those with a central role in policy-making at local, national and regional levels, and across all sectors of governance, not just those within the health, migration or immunization sectors. -
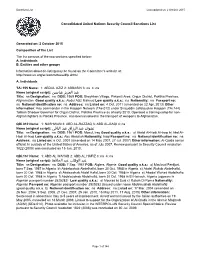
Name (Original Script): ﻦﯿﺳﺎﺒﻋ ﺰﻳﺰﻌﻟا ﺪﺒﻋ ﻧﺸﻮان ﻋﺒﺪ اﻟﺮزاق ﻋﺒﺪ
Sanctions List Last updated on: 2 October 2015 Consolidated United Nations Security Council Sanctions List Generated on: 2 October 2015 Composition of the List The list consists of the two sections specified below: A. Individuals B. Entities and other groups Information about de-listing may be found on the Committee's website at: http://www.un.org/sc/committees/dfp.shtml A. Individuals TAi.155 Name: 1: ABDUL AZIZ 2: ABBASIN 3: na 4: na ﻋﺒﺪ اﻟﻌﺰﻳﺰ ﻋﺒﺎﺳﯿﻦ :(Name (original script Title: na Designation: na DOB: 1969 POB: Sheykhan Village, Pirkowti Area, Orgun District, Paktika Province, Afghanistan Good quality a.k.a.: Abdul Aziz Mahsud Low quality a.k.a.: na Nationality: na Passport no: na National identification no: na Address: na Listed on: 4 Oct. 2011 (amended on 22 Apr. 2013) Other information: Key commander in the Haqqani Network (TAe.012) under Sirajuddin Jallaloudine Haqqani (TAi.144). Taliban Shadow Governor for Orgun District, Paktika Province as of early 2010. Operated a training camp for non- Afghan fighters in Paktika Province. Has been involved in the transport of weapons to Afghanistan. QDi.012 Name: 1: NASHWAN 2: ABD AL-RAZZAQ 3: ABD AL-BAQI 4: na ﻧﺸﻮان ﻋﺒﺪ اﻟﺮزاق ﻋﺒﺪ اﻟﺒﺎﻗﻲ :(Name (original script Title: na Designation: na DOB: 1961 POB: Mosul, Iraq Good quality a.k.a.: a) Abdal Al-Hadi Al-Iraqi b) Abd Al- Hadi Al-Iraqi Low quality a.k.a.: Abu Abdallah Nationality: Iraqi Passport no: na National identification no: na Address: na Listed on: 6 Oct. 2001 (amended on 14 May 2007, 27 Jul. -

London Roundtable
2018 LONDON ROUNDTABLE Dr. Virginie Andre Understanding the Impact of Terrorist Event Reporting on Countering Violent Extremism: From A Practitioner’s Perspective PREFACE This report presents the key findings from the London Roundtable on “Understanding the Im- pact of Terrorist Event Reporting on Countering Violent Extremism”. The event was held at the Australian High Commission in London on 30-31 January 2018. The roundtable brought to- gether media practitioners, CVE and PVE front line practitioners, policy-makers and academics drawn from Australia, the United Kingdom, Belgium, France, Germany, Sweden, Norway, Fin- land and the United States of America. Other attendees included representatives from various Australian and British Government departments and New Scotland Yard. This report provides summaries of each of the panel discussions that were delivered at the roundtable, before drawing out the key themes, which emerged and policy recommendations. 1 2 ACKNOWLEDGEMENTS We would like to express our gratitude to the following for their support for this roundtable and associated activities: the Australian Department of Foreign Affairs and Trade; New Scot- land Yard; the Egmont Royal Institute for International Relations; the European Union Radicali- sation Awareness Network and Exit Sweden. A special thanks goes to roundtable co-convenors Bill Elischer and Abid Raja, roundtable facili- tator Benjamin Mols and research assistant Elena Pinot. 3 4 TABLE OF CONTENTS 01 Preface Session Two: Policing 44 Implications of Media Covered Terrorism -

The Nordic Countries of Denmark, Finland, Norway and Sweden: the Recommended Approach in Practice
Legislative Landscape Review: Legislative Approaches to Immunization across the European Region December 2018 The Nordic countries of Denmark, Finland, Norway and Sweden: The recommended approach in practice European Region Matrix: Immunization Legislation COUNTRY Is the right Is it Is it Does the Is Are there Has the Does the to health mandatory mandatory government immunization penalties judiciary of government in this for the for the verify required for in cases of the country finance country’s government people to be that the attending an noncompli- ruled on immuni- constitu- to provide immunized? individual educational ance? mandatory zation? tion? immuni- has been institution? immuni- zation? immunized? zation? Denmark NO YES NO YES NO NO NO YES COVERAGE DTP3 98% MEASLES (cases, 7/2017–6/2018) INDICATORS IPV N/A 6 Finland YES YES NO YES NO NO NO YES COVERAGE DTP3 89% MEASLES (cases, 7/2017–6/2018) INDICATORS IPV N/A 13 Norway NO YES NO YES NO NO NO YES COVERAGE DTP3 96% MEASLES (cases, 7/2017–6/2018) INDICATORS IPV N/A 8 Sweden NO YES NO NO NO NO NO YES COVERAGE DTP3 97% MEASLES (cases, 7/2017–6/2018) INDICATORS IPV N/A 49 Answer Verified by Authoritative Secondary Sources Answer Verified by Survey WHO-UNICEF estimates of immunization coverage. World Health Organization [data from 2017] [cited july 2018]. Available from: http://apps.who.int/immunization_monitoring/globalsummary/timeseries/tswucoveragebcg.html Introduction Using the “Likert Scale: Assessing Levels of Immunization Legislation” developed by the Sabin Vaccine Institute (Sabin) for this study, the Nordic countries of Denmark, Finland, Norway and Sweden all receive the recommended classification. -

Voices from Tensta Report of a Pilot Project in Tensta, a Suburb of Stockholm
Voices From Tensta Report of a pilot project in Tensta, a suburb of Stockholm Photo credit: Interpeace. March 2014. Voices From Voices Tensta Title: Voices From Tensta, Report of a Pilot Project in Tensta, a suburb of Stockholm Authors: Interpeace Editing: Christelle Mestre; Renée Lariviere; Valeria Gholizadeh Date: August 2014 Published by: Interpeace © Interpeace, 2014 All rights reserved Produced in Switzerland The views expresses in this publication are those of the key stakeholders consulted and do not necessarily represent those of the sponsors. Reproduction of figures or short excerpts from this report is authorized free of charge and without formal written permission provided that the original source is properly acknowledged, with mention of the complete name of the report, the publisher and the numbering of the page(s) or the figure(s). Permission can only be granted to use the material exactly as it is in the repot. Please be aware that figures cannot be altered in any way, including the full legend. For media use, it is sufficient to cite the source while using the original graphic or figure. “In Tensta, everyone knows each other (the ethnic communities, the elders, the youth, etc.) and maintains close relationships with his/her neighbor and friends. Despite their various identities, which complement each other, the people of Tensta all have one thing in common: exclusion.” Consultation with a young person, Tensta, February 2014 About Interpeace Interpeace is an independent, international peacebuilding organization that is recognized for a proven methodology to help resolve conflict and build peace. Interpeace believes that peace is possible. -

Istraživanje Migracija I Integracije Imigranata Quality of Life Among Turkish Immigrants in Sweden: a Study for Assessing the M
IstražIvanje MIgracIja I IntegracIje IMIgranata Migracijske i etničke teme 27 (2011), 1: 39–55 UDK: 159.923.2-054.72(485=512.161) 316.7(485=512.161) Izvorni znanstveni rad Primljeno: 21. 02. 2011. Prihvaćeno: 14. 04. 2011. nuran BaYraM Uludag University, Faculty of Economics and Administrative Sciences, Department of Econometrics, Bursa [email protected] Daniel tHOrBUrn Stockholm University, Department of Statistics, Stockholm [email protected] nazan BILgeL Uludag University, Faculty of Medicine, Department of Family Medicine, Bursa [email protected] Quality of Life among Turkish Immigrants in Sweden: a Study for Assessing the Measurement Properties of the World Health Organization’s Quality of Life 100 Instrument SUMMARY Many instruments have been developed to measure the multidimensional construct of quality of life. One of them has been developed by the World Health Organization (WHOQOL-100) and adapted into different languages and cultures around the world. The authors of this study wanted to assess the measurement properties of the Turkish version of WHOQOL-100, to find out the latent factors underlying quality of life, and to determine the direction and magni- tude of the interdependent effects among these factors by using structural equation modeling (SEM). The measurement properties of the Turkish version of WHOQOL-100 scale were as- sessed on 520 voluntary participants who were immigrants in Stockholm/Sweden. SEM gave us one second-order factor QOL and the five correlated first-order factors labelled: physical, social relations, psychological, environment and independence. In the model for total par- ticipants, all the factor loadings were high (ranging from 0.60 to 0.92 except for “sexuality” which was 0.47), indicating a strong association between each of the latent factors and their respective items. -

Somalis in Malmo
Somalis-cover-final-MALMO_Layout 1 2014.01.20. 9:18 Page 1 AT HOME IN EUROPE SOMALIS SOMALIS IN Minority communities – whether Muslim, migrant or Roma – continue to come under MALMÖ intense scrutiny in Europe today. This complex situation presents Europe with one its greatest challenges: how to ensure equal rights in an environment of rapidly expanding diversity. IN MALMÖ At Home in Europe, part of the Open Society Initiative for Europe, Open Society Foundations, is a research and advocacy initiative which works to advance equality and social justice for minority and marginalised groups excluded from the mainstream of civil, political, economic, and, cultural life in Western Europe. Somalis in European Cities Muslims in EU Cities was the project’s first comparative research series which examined the position of Muslims in 11 cities in the European Union. Somalis in European cities follows from the findings emerging from the Muslims in EU Cities reports and offers the experiences and challenges faced by Somalis across seven cities in Europe. The research aims to capture the everyday, lived experiences as well as the type and degree of engagement policymakers have initiated with their Somali and minority constituents. somalis-malmö_incover-publish-2014-0120_publish.qxd 2014.01.21. 22:27 Page 1 Somalis in Malmö At Home in Europe somalis-malmö_incover-publish-2014-0120_publish.qxd 2014.01.21. 22:27 Page 2 ©2014 Open Society Foundations This publication is available as a pdf on the Open Society Foundations website under a Creative Commons license that allows copying and distributing the publication, only in its entirety, as long as it is attributed to the Open Society Foundations and used for noncommercial educational or public policy purposes.