Small & Large Intestine
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Anatomy of the Rectum and Anal Canal
BASIC SCIENCE identify the rectosigmoid junction with confidence at operation. The anatomy of the rectum The rectosigmoid junction usually lies approximately 6 cm below the level of the sacral promontory. Approached from the distal and anal canal end, however, as when performing a rigid or flexible sigmoid- oscopy, the rectosigmoid junction is seen to be 14e18 cm from Vishy Mahadevan the anal verge, and 18 cm is usually taken as the measurement for audit purposes. The rectum in the adult measures 10e14 cm in length. Abstract Diseases of the rectum and anal canal, both benign and malignant, Relationship of the peritoneum to the rectum account for a very large part of colorectal surgical practice in the UK. Unlike the transverse colon and sigmoid colon, the rectum lacks This article emphasizes the surgically-relevant aspects of the anatomy a mesentery (Figure 1). The posterior aspect of the rectum is thus of the rectum and anal canal. entirely free of a peritoneal covering. In this respect the rectum resembles the ascending and descending segments of the colon, Keywords Anal cushions; inferior hypogastric plexus; internal and and all of these segments may be therefore be spoken of as external anal sphincters; lymphatic drainage of rectum and anal canal; retroperitoneal. The precise relationship of the peritoneum to the mesorectum; perineum; rectal blood supply rectum is as follows: the upper third of the rectum is covered by peritoneum on its anterior and lateral surfaces; the middle third of the rectum is covered by peritoneum only on its anterior 1 The rectum is the direct continuation of the sigmoid colon and surface while the lower third of the rectum is below the level of commences in front of the body of the third sacral vertebra. -

Crohn's Disease of the Colon
Gut, 1968, 9, 164-176 Gut: first published as 10.1136/gut.9.2.164 on 1 April 1968. Downloaded from Crohn's disease of the colon V. J. McGOVERN AND S. J. M. GOULSTON From the Royal Prince Alfred Hospital, Sydney, Australia The fact that Crohn's disease may involve the colon never affected unless there had been surgical inter- either initially or in association with small bowel ference. There was no overt manifestation of mal- disease is now firmly established due largely to the absorption in any of these patients. evidence presented by Lockhart-Mummery and In 18 cases the colon alone was involved. Five had Morson (1960, 1964) and Marshak, Lindner, and universal involvement, five total involvement with Janowitz (1966). This entity is clearly distinct from sparing of the rectum, two involvement of the ulcerative colitis and other forms of colonic disease. descending colon only, two the transverse colon only, Our own experience with this disorder reveals many and in the other four there was variable involvement similarities with that published from the U.K. and of areas of large bowel (Fig. 2). the U.S.A. Thirty patients with Crohn's disease involving the large bowel were seen at the Royal CLINICAL FEATURES Prince Alfred Hospital during the last decade, the majority during the past five years. The criteria for The age incidence varied from 6 to 69 years when the inclusion were based on histological examination of patient was first seen, the majority being between the operative specimens in 28 and on clinical and radio- ages of 11 and 50. -

Anatomy of Major Duodenal Papilla Influences ERCP Outcomes
Journal of Clinical Medicine Article Anatomy of Major Duodenal Papilla Influences ERCP Outcomes and Complication Rates: A Single Center Prospective Study Gheorghe G. Balan 1 , Mukul Arya 2, Adrian Catinean 3, Vasile Sandru 4,*, Mihaela Moscalu 1 , Gabriel Constantinescu 5, Anca Trifan 1 , Gabriela Stefanescu 1,* and Catalin Victor Sfarti 1 1 Faculty of Medicine, Grigore T. Popa University of Medicine and Pharmacy, 700115 Iasi, Romania; [email protected] (G.G.B.); [email protected] (M.M.); [email protected] (A.T.); [email protected] (C.V.S.) 2 New York Presbitarian Brooklyn Methodist Hospital, New York, NY 11215, USA; [email protected] 3 Faculty of Medicine, Iuliu Hatieganu University of Medicine and Pharmacy, 400012 Cluj-Napoca, Romania; [email protected] 4 Department of Gastroenterology, Clinical Emergency Hospital of Bucharest, 014461 Bucharest, Romania 5 Faculty of Medicine, Carol Davila University of Medicine and Pharmacy, 020021 Bucharest, Romania; [email protected] * Correspondence: [email protected] (V.S.); [email protected] (G.S.) Received: 27 March 2020; Accepted: 25 May 2020; Published: 28 May 2020 Abstract: Background: Endoscopic retrograde cholangiopancreatography (ERCP) has been one of the most intensely studied endoscopic procedures due to its overall high complication rates when compared to other digestive endoscopy procedures. The safety and outcome of such procedures have been linked to multiple procedure- or patient-related risk factors. The aim of our study is to evaluate whether the morphology of the major duodenal papilla influences the ERCP outcomes and complication rates. Methods: A total of 322 patients with a native papilla have been included in the study over an eight month period. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

Sporadic (Nonhereditary) Colorectal Cancer: Introduction
Sporadic (Nonhereditary) Colorectal Cancer: Introduction Colorectal cancer affects about 5% of the population, with up to 150,000 new cases per year in the United States alone. Cancer of the large intestine accounts for 21% of all cancers in the US, ranking second only to lung cancer in mortality in both males and females. It is, however, one of the most potentially curable of gastrointestinal cancers. Colorectal cancer is detected through screening procedures or when the patient presents with symptoms. Screening is vital to prevention and should be a part of routine care for adults over the age of 50 who are at average risk. High-risk individuals (those with previous colon cancer , family history of colon cancer , inflammatory bowel disease, or history of colorectal polyps) require careful follow-up. There is great variability in the worldwide incidence and mortality rates. Industrialized nations appear to have the greatest risk while most developing nations have lower rates. Unfortunately, this incidence is on the increase. North America, Western Europe, Australia and New Zealand have high rates for colorectal neoplasms (Figure 2). Figure 1. Location of the colon in the body. Figure 2. Geographic distribution of sporadic colon cancer . Symptoms Colorectal cancer does not usually produce symptoms early in the disease process. Symptoms are dependent upon the site of the primary tumor. Cancers of the proximal colon tend to grow larger than those of the left colon and rectum before they produce symptoms. Abnormal vasculature and trauma from the fecal stream may result in bleeding as the tumor expands in the intestinal lumen. -

Anatomy of Small Intestine Doctors Notes Notes/Extra Explanation Please View Our Editing File Before Studying This Lecture to Check for Any Changes
Color Code Important Anatomy of Small Intestine Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives: At the end of the lecture, students should: List the different parts of small intestine. Describe the anatomy of duodenum, jejunum & ileum regarding: the shape, length, site of beginning & termination, peritoneal covering, arterial supply & lymphatic drainage. Differentiate between each part of duodenum regarding the length, level & relations. Differentiate between the jejunum & ileum regarding the characteristic anatomical features of each of them. Abdomen What is Mesentery? It is a double layer attach the intestine to abdominal wall. If it has mesentery it is freely moveable. L= liver, S=Spleen, SI=Small Intestine, AC=Ascending Colon, TC=Transverse Colon Abdomen The small intestines consist of two parts: 1- fixed part (no mesentery) (retroperitoneal) : duodenum 2- free (movable) part (with mesentery) :jejunum & ileum Only on the boys’ slides RELATION BETWEEN EMBRYOLOGICAL ORIGIN & ARTERIAL SUPPLY مهم :Extra Arterial supply depends on the embryological origin : Foregut Coeliac trunk Midgut superior mesenteric Hindgut Inferior mesenteric Duodenum: • Origin: foregut & midgut • Arterial supply: 1. Coeliac trunk (artery of foregut) 2. Superior mesenteric: (artery of midgut) The duodenum has 2 arterial supply because of the double origin The junction of foregut and midgut is at the second part of the duodenum Jejunum & ileum: • Origin: midgut • Arterial -

6-Physiology of Large Intestine.Pdf
LARGE INTESTINE COLON MOTILITY Color index • Important • Further explanation 1 Contents . Mind map.......................................................3 . Colon Function…………………………………4 . Physiology of Colon Regions……...…………6 . Absorption and Secretion…………………….8 . Types of motility………………………………..9 . Innervation and motility…………………….....11 . Defecation Reflex……………………………..13 . Fecal Incontinence……………………………15 Please check out this link before viewing the file to know if there are any additions/changes or corrections. The same link will be used for all of our work Physiology Edit 2 Mind map 3 COLON FUNCTIONS: Secretions of the Large Intestine: Mucus Secretion. • The mucosa of the large intestine has many crypts of 3 Colon consist of : Lieberkühn. • Absence of villi. • Ascending • Transverse • The epithelial cells contain almost no enzymes. • Descending • Presence of goblet cells that secrete mucus (provides an • Sigmoid adherent medium for holding fecal matter together). • Rectum • Anal canal • Stimulation of the pelvic nerves1 from the spinal cord can cause: Functions of the Large Intestine: o marked increase in mucus secretion. o This occurs along with increase in peristaltic motility 1. Reabsorb water and compact material of the colon. into feces. 2. Absorb vitamins produced by bacteria. • During extreme parasympathetic stimulation, so much 3. Store fecal matter prior to defecation. mucus can be secreted into the large intestine that the person has a bowel movement of ropy2 mucus as often as every 30 minutes; this mucus often contains little or no 1: considered a part of parasympathetic in large intestine . fecal material. 2: resembling a rope in being long, strong, and fibrous 3: anatomical division. 4 ILEOCECAL VALVE It prevents backflow of contents from colon into small intestine. -

Digestive System
Naziha Sultan Ahmed, BVMS, MSc Scientific degree (Assis. Prof.), Department of Anatomy College of Veterinary Medicine, University of Mosul, Mosul, Iraq https://orcid.org/0000-0002-2856-8277 https://www.researchgate.net/profile/Naziha_Ahmed Anatomy | Part 18| 2nd year 2019 Digestive System Fixation of the liver (Ligaments of the liver): 1-Lesser omentum: consist of two parts: a/Hepatogastric ligament: connect between hepatic porta and lesser curvature of the stomach . b/Hepatoduodenal ligament: connect between hepatic porta and the cranial part of the duodenum. 2-Coronary ligament: connect between the parietal (diaphragmatic ) surface of liver, with the diaphragm and the caudal vena cava. 3-Falciform ligament: connect between the notch of round ligament in the liver and the sternal part of the diaphragm. 4-Round ligament: the residue (remnants) of the umbilical vein of the fetus. 5-Hepatorenal ligament: connect between the right lobe of liver and the right kidney. 6-Right & left triangular ligaments: connect between the dorsal border of right and left lobes of the liver and the diaphragm . Both ligaments continue medially with the coronary ligament. CouAnatomy | Digestive system | Assis. Prof. Naziha Sultan Ahmed Page | 1 The pancreas: Pancreas has V-shape. It consists of base and two limbs (right & left limbs). *In horse: large pancreas body perforated by portal vein and long left limb, with short right limb (because of large size of cecum in horse ). The horse pancreas has two ducts: 1-Chief pancreatic duct: opens with bile duct at the major duodenal papilla. 2-Accessory pancreatic duct: opens at the minor duodenal papilla. *In dog: pancreas notched by the portal vein. -

Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and Main Principals Of
Yagenich L.V., Kirillova I.I., Siritsa Ye.A. Latin and main principals of anatomical, pharmaceutical and clinical terminology (Student's book) Simferopol, 2017 Contents No. Topics Page 1. UNIT I. Latin language history. Phonetics. Alphabet. Vowels and consonants classification. Diphthongs. Digraphs. Letter combinations. 4-13 Syllable shortness and longitude. Stress rules. 2. UNIT II. Grammatical noun categories, declension characteristics, noun 14-25 dictionary forms, determination of the noun stems, nominative and genitive cases and their significance in terms formation. I-st noun declension. 3. UNIT III. Adjectives and its grammatical categories. Classes of adjectives. Adjective entries in dictionaries. Adjectives of the I-st group. Gender 26-36 endings, stem-determining. 4. UNIT IV. Adjectives of the 2-nd group. Morphological characteristics of two- and multi-word anatomical terms. Syntax of two- and multi-word 37-49 anatomical terms. Nouns of the 2nd declension 5. UNIT V. General characteristic of the nouns of the 3rd declension. Parisyllabic and imparisyllabic nouns. Types of stems of the nouns of the 50-58 3rd declension and their peculiarities. 3rd declension nouns in combination with agreed and non-agreed attributes 6. UNIT VI. Peculiarities of 3rd declension nouns of masculine, feminine and neuter genders. Muscle names referring to their functions. Exceptions to the 59-71 gender rule of 3rd declension nouns for all three genders 7. UNIT VII. 1st, 2nd and 3rd declension nouns in combination with II class adjectives. Present Participle and its declension. Anatomical terms 72-81 consisting of nouns and participles 8. UNIT VIII. Nouns of the 4th and 5th declensions and their combination with 82-89 adjectives 9. -
Digestive System
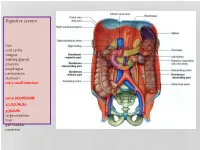
Digestive system Lips oral cavity tongue salivary glands pharynx esophagus peritoneum stomach m6-7 small intestine: cm25 DEODENUM: 2/5JEJUNUM: 3/5ILIUM: large intestine liver gall bladder pancreas :Duodenum Sup. Part Descending part Horizontal part Ascending part Major duodenal papilla Minor duodenal papilla : JEJUNUM / ILIUM From duodenojejunal curvature To Iliocecal Different jejunum & ilium 3Tenia coli: sigmoid 2 / rectum 0 Houstra / saccule Appendices epiploicae : No in Appendix / cecum / rectum Many in sigmoid DIFFERENT BETWEEN SMALL AND LARGE INTESTINE large intestine 1.5m Cecum appendix ascending colon transverse colon descending colon sigmoid colon rectum anal canal McBurneys point ascending colon transverse colon descending colon sigmoid colon :Rectum cm 12 Sacral flexure Puborectalis muscle Perineal flexure Rectum Ampulla : Anal canal cm 4 sup. = anal column / anal valve / anal sinus / pectinate line 2/3 Hiltons white line .inf 1/3 :Anal sphincter Internal sphincter External sphincter: deep / superficial / subcutaneous Liver: 1.5 kgr Located in Rt. & lf. Hypochondriac & epigastric region Surfaces: Sup. Anterior Surface: falciform ligament Inf. Surface: H shape fissure / porta hepatis / quadrate lobe / qudate lobe Post. Surface: bare area Rt. Surface: ribs 7-11 / Rt. lung Liver viewed from posterior Liver viewed from inferior Liver viewed from inferior Liver viewed from posterior :Liver vasculature 20%Hepatic artery 80%Portal vein Supra hepatic vein IVC :Nerve Sympathetic Parasympathetic From Vagus+ Phernic + celiac :Gall bladder Located in inf. Surface of liver cm7-10 Length: cm3-4 Wide: :Structure Fundus Body Infundibulum Neck Systic duct :Pancreas 2–L1 L cm15-20 Length: cm3Wide: cm2 Thickness: gram 90 :Structure Head :Uncinate process / sup. Mesenteric artery Neck: portal vein / sup. -

COLON RESECTION (For TUMOR)
GASTROINTESTINAL PATHOLOGY GROSSING GUIDELINES Specimen Type: COLON RESECTION (for TUMOR) Procedure: 1. Measure length and range of diameter or circumference. 2. Describe external surface, noting color, granularity, adhesions, fistula, discontinuous tumor deposits, areas of retraction/puckering, induration, stricture, or perforation. 3. Measure the width of attached mesentery if present. Note any enlarged lymph nodes and thrombosed vessels or other vascular abnormalities. 4. Open the bowel longitudinally along the antimesenteric border, or opposite the tumor if tumor is located on the antimesenteric border, i.e. try to avoid cutting through the tumor. 5. Measure any areas of luminal narrowing or dilation (location, length, diameter or circumference, wall thickness), noting relation to tumor. 6. Describe tumor, noting size, shape, color, consistency, appearance of cut surface, % of circumference of the bowel wall involved by the tumor, depth of invasion through bowel wall, and distance from margins of resection (radial/circumferential margin, mesenteric margin, closest proximal or distal margin). a. If resection includes mesorectum, gross evaluation of the intactness of mesorectum must be included. For rectum, the location of the tumor must also be oriented: anterior, posterior, right lateral, left lateral. b. If a rectal tumor is close to distal margin, the distance of tumor to the distal margin should be measured when specimen is stretched. This is usually done during intraoperative gross consultation when specimen is fresh. c. If the tumor is in a retroperitoneal portion of the bowel (e.g. rectum), radial/retroperitoneal margin must be inked and one or more sections must be obtained (a shave margin, if tumor is far from the radial margin; and perpendicular sections showing the relationship of the tumor to the inked radial margin, if tumor is close to the radial margin). -

Carcinoid Tumor of the Minor Papilla in Complete Pancreas Divisum Presenting As Recurrent Abdominal Pain Yong Gil Kim, Tae Nyeun Kim*, Kyeong Ok Kim
Kim et al. BMC Gastroenterology 2010, 10:17 http://www.biomedcentral.com/1471-230X/10/17 CASE REPORT Open Access Carcinoid tumor of the minor papilla in complete pancreas divisum presenting as recurrent abdominal pain Yong Gil Kim, Tae Nyeun Kim*, Kyeong Ok Kim Abstract Background: Tumors of the minor papilla of the duodenum are extremely rare, and they are mostly neuroendocrine tumors, such as somatostatinomas and carcinoid tumors. However, true incidence of carcinoid tumors in minor papilla might be much higher, because patients with minor papillary tumors usually remain asymptomatic. We report a very unusual case of carcinoid tumor in a patient with complete pancreas divisum with a review of the literature. Case presentation: A 56-year-old female patient was referred for evaluation of pancreatic duct dilatation noted on abdominal ultrasonography and computerized tomography. She complained of intermittent epigastric pain for 6 months. A MRCP and ERCP revealed complete pancreas divisum with dilatation of the main pancreatic duct. On duodenoscopy, a small, yellows, subepithelial nodule was visualized at the minor papilla; biopsy of this lesion revealed a carcinoid tumor. She underwent a pylorus-preserving pancreaticoduodenectomy. The histologic evaluation showed a single nodule, 1 cm in diameter, in the submucosa with duodenal and vascular invasion and metastasis to the regional lymph nodes. Conclusion: Although the size of the carcinoid tumor was small and the tumor was hormonally inactive, the concomitant pancreas divisum led to an early diagnosis, the tumor had aggressive behavior. Carcinoid tumors of the minor papilla should be included in the differential diagnosis of recurrent abdominal pain or pancreatitis of unknown cause.