Carcinoid Tumor of the Minor Papilla in Complete Pancreas Divisum Presenting As Recurrent Abdominal Pain Yong Gil Kim, Tae Nyeun Kim*, Kyeong Ok Kim
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rectal Indomethacin Or I.V. Gabexate Mesylate As Prophylaxis for AP ERCP
European Review for Medical and Pharmacological Sciences 2017; 21: 5268-5274 Rectal indomethacin or intravenous gabexate mesylate as prophylaxis for acute pancreatitis post-endoscopic retrograde cholangiopancreatography V. GUGLIELMI, M. TUTINO, V. GUERRA, P. GIORGIO National Institute of Gastroenterology, “S. de Bellis” Research Hospital Castellana Grotte, Bari, Italy Abstract. – OBJECTIVE: We aimed to evaluate mechanisms of AP are obstruction of the com- the results in our case series of AP ERCP over mon bile duct by stones, and alcohol abuse. En- the last three years. The prophylaxis for acute doscopic retrograde cholangiopancreatography pancreatitis (AP) post-endoscopic retrograde (ERCP) is the most frequent iatrogenic cause. cholangiopancreatography (ERCP) consists of rectal indomethacin, but some studies are not Post-ERCP AP is the most common and fear concordant. some adverse event for this procedure. In the PATIENTS AND METHODS: We compared 241 United States this complication costs $150 mil- ERCP performed from January 2014 to February lion annually for American Healthcare2,3 and it 2015 with intravenous gabexate mesylate (Group is a common cause of endoscopy-related lawsu- A), with the 387 ERCP performed from March its against gastroenterologists in the world. It 2015 to December 2016 with rectal indometha- has a significant morbidity and rare mortality cin (Group B) as prophylaxis for AP post-ERCP. RESULTS: There were 8 (3.31%) AP post-ERCP rate. About 10% of post-ERCP AP is moderate in Group A vs. 4 (1.03%) in Group B. or severe. Post-ERCP severe AP is associated CONCLUSIONS: Rectal indomethacin shows a with a higher mortality than non-ERCP-indu- better statistically significant performance than ced pancreatitis, but without statistical eviden- intravenous gabexate mesylate in the prophylax- ce4. -

Anatomy of Small Intestine Doctors Notes Notes/Extra Explanation Please View Our Editing File Before Studying This Lecture to Check for Any Changes
Color Code Important Anatomy of Small Intestine Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives: At the end of the lecture, students should: List the different parts of small intestine. Describe the anatomy of duodenum, jejunum & ileum regarding: the shape, length, site of beginning & termination, peritoneal covering, arterial supply & lymphatic drainage. Differentiate between each part of duodenum regarding the length, level & relations. Differentiate between the jejunum & ileum regarding the characteristic anatomical features of each of them. Abdomen What is Mesentery? It is a double layer attach the intestine to abdominal wall. If it has mesentery it is freely moveable. L= liver, S=Spleen, SI=Small Intestine, AC=Ascending Colon, TC=Transverse Colon Abdomen The small intestines consist of two parts: 1- fixed part (no mesentery) (retroperitoneal) : duodenum 2- free (movable) part (with mesentery) :jejunum & ileum Only on the boys’ slides RELATION BETWEEN EMBRYOLOGICAL ORIGIN & ARTERIAL SUPPLY مهم :Extra Arterial supply depends on the embryological origin : Foregut Coeliac trunk Midgut superior mesenteric Hindgut Inferior mesenteric Duodenum: • Origin: foregut & midgut • Arterial supply: 1. Coeliac trunk (artery of foregut) 2. Superior mesenteric: (artery of midgut) The duodenum has 2 arterial supply because of the double origin The junction of foregut and midgut is at the second part of the duodenum Jejunum & ileum: • Origin: midgut • Arterial -

Frey Operation for Chronic Pancreatitis Associated with Pancreas Divisum: Case Report and Review of the Literature
Case report Frey operation for chronic pancreatitis associated with pancreas divisum: case report and review of the literature Magdalena Skórzewska1, Tomasz Romanowicz2, Jerzy Mielko1, Andrzej Kurylcio1, Jan Pertkiewicz3, Robert Zymon2, Wojciech P. Polkowski1 1Department of Surgical Oncology, Medical University of Lublin, Poland 2Department of General and Oncological Surgery, Pope John Paul II Regional Hospital, Zamosc, Poland 3Olympus Endotherapy, Warsaw, Poland Prz Gastroenterol 2014; 9 (3): 175–178 DOI: 10.5114/pg.2014.43581 Key words: pancreas divisum, chronic pancreatitis, surgery. Address for correspondence: Prof. Wojciech P. Polkowski MD, PhD, Department of Surgical Oncology, Medical University of Lublin, 11 Staszica St, 20-081 Lublin, Poland, phone: +48 81 534 43 13, fax: +48 81 532 23 95, e-mail: [email protected] Abstract Pancreas divisum (PD) is the most common congenital anomaly of the pancreas, which increases susceptibility to recurrent pancreatitis. Usually, after failure of initial endoscopic therapies, surgical treatment combining pancreatic resection or drainage is used. The Frey procedure is used for chronic pancreatitis, but it has not been reported to be applied in an adult patient with PD-associated pancreatitis. The purpose of the paper was to describe effective treatment of this rare condition by the Frey procedure after failure of interventional endoscopic treatment. A 39-year-old female patient was initially treated for recurrent acute pancreatitis. After endoscopic diagnosis of PD, the minor duodenal papilla was incised and a plastic stent was inserted into the dorsal pancreatic duct. During the following 36 months, the patient was hospitalised several times because of recur- rent episodes of pancreatitis. Thereafter, local resection of the pancreatic head combined with lateral pancreaticojejunostomy was performed with no complications. -

A Gastric Duplication Cyst with an Accessory Pancreatic Lobe
Turk J Gastroenterol 2014; 25 (Suppl.-1): 199-202 An unusual cause of recurrent pancreatitis: A gastric duplication cyst with an accessory pancreatic lobe xxxxxxxxxxxxxxx Aysel Türkvatan1, Ayşe Erden2, Mehmet Akif Türkoğlu3, Erdal Birol Bostancı3, Selçuk Dişibeyaz4, Erkan Parlak4 1Department of Radiology, Türkiye Yüksek İhtisas Hospital, Ankara, Turkey 2Department of Radiology, Ankara University Faculty of Medicine, Ankara, Turkey 3Department of Gastroenterological Surgery, Türkiye Yüksek İhtisas Hospital, Ankara, Turkey 4Department of Gastroenterology, Türkiye Yüksek İhtisas Hospital, Ankara, Turkey ABSTRACT Congenital anomalies of pancreas and its ductal drainage are uncommon but in general surgically correctable causes of recurrent pancreatitis. A gastric duplication cyst communicated with an accessory pancreatic lobe is an extremely rare cause of recurrent pancreatitis, but an early and accurate diagnosis of this anomaly is important because suitable surgical treatment may lead to a satisfactory outcome. Herein, we presented multidetector com- puted tomography and magnetic resonance imaging findings of a gastric duplication cyst communicating with an accessory pancreatic lobe via an aberrant duct in a 29-year-old woman with recurrent acute pancreatitis and also reviewed other similar cases reported in the literature. Keywords: Aberrant pancreatic duct, accessory pancreatic lobe, acute pancreatitis, gastric duplication cyst, multi- detector computed tomography, magnetic resonance imaging INTRODUCTION Herein, we presented multidetector CT and MRI find- Report Case Congenital causes of recurrent pancreatitis include ings of a gastric duplication cyst communicating with anomalies of the biliary or pancreatic ducts, espe- an accessory pancreatic lobe via an aberrant duct in a cially pancreas divisum. A gastric duplication cyst 29-year-old woman with recurrent acute pancreatitis communicating with an aberrant pancreatic duct is and also reviewed other similar cases reported in the an extremely rare but curable cause of recurrent pan- literature. -

Intraductal Papillary Mucinous Carcinoma of The
Nishi et al. BMC Gastroenterology (2015) 15:78 DOI 10.1186/s12876-015-0313-3 CASE REPORT Open Access Intraductal papillary mucinous carcinoma of the pancreas associated with pancreas divisum: a case report and review of the literature Takeshi Nishi1,2*, Yasunari Kawabata2, Noriyoshi Ishikawa3, Asuka Araki3, Seiji Yano2, Riruke Maruyama3 and Yoshitsugu Tajima2 Abstract Background: Pancreas divisum, the most common congenital anomaly of the pancreas, is caused by failure of the fusion of the ventral and dorsal pancreatic duct systems during embryological development. Although various pancreatic tumors can occur in patients with pancreas divisum, intraductal papillary mucinous neoplasm is rare. Case presentation: A 77-year-old woman was referred to our hospital because she was incidentally found to have a cystic tumor in her pancreas at a regular health checkup. Contrast-enhanced abdominal computed tomography images demonstrated a cystic tumor in the head of the pancreas measuring 40 mm in diameter with slightly enhancing mural nodules within the cyst. Endoscopic retrograde pancreatography via the major duodenal papilla revealed a cystic tumor and a slightly dilated main pancreaticductwithanabruptinterruptionattheheadofthe pancreas. The orifice of the major duodenal papilla was remarkably dilated and filled with an abundant extrusion of mucin, and the diagnosis based on pancreatic juice cytology was “highly suspicious for adenocarcinoma”. Magnetic resonance cholangiopancreatography depicted a normal, non-dilated dorsal pancreatic duct throughout the pancreas. The patient underwent a pylorus-preserving pancreaticoduodenectomy under the diagnosis of intraductal papillary mucinous neoplasm with suspicion of malignancy arising in the ventral part of the pancreas divisum. A pancreatography via the major and minor duodenal papillae on the surgical specimen revealed that the ventral and dorsal pancreatic ducts were not connected, and the tumor originated in the ventral duct, i.e., the Wirsung’s duct. -

Small & Large Intestine
Small & Large Intestine Gastrointestinal block-Anatomy-Lecture 6,7 Editing file Objectives Color guide : Only in boys slides in Green Only in girls slides in Purple important in Red At the end of the lecture, students should be able to: Notes in Grey ● List the different parts of small intestine. ● Describe the anatomy of duodenum, jejunum & ileum regarding: (the shape, length, site of beginning & termination, peritoneal covering, arterial supply & lymphatic drainage) ● Differentiate between each part of duodenum regarding the length, level & relations. ● Differentiate between the jejunum & ileum regarding the characteristic anatomical features of each of them. ● List the different parts of large intestine. ● List the characteristic features of colon. ● Describe the anatomy of different parts of large intestine regarding: (the surface anatomy, peritoneal covering, relations, arterial & nerve supply) Small intestine The small intestine divided into : Fixed Part (No Mesentery): Free (Movable) Part (With Parts Duodenum* Mesentery): Jejunum & Ileum Shape C-shaped loop coiled tube Length 10 inches 6 meters (20 feet) Transverse Colon separates the Beginning At pyloro-duodenal junction at duodeno-jejunal flexure stomach/liver from the jejunum/ileum Termination At duodeno-jejunal flexure at ileo-ceacal flexure Peritoneal Covering Retroperitoneal mesentery of small intestine Divisions 4 parts --------- Foregut (above bile duct opening in 2nd part )& Midgut Embryological origin Midgut (below bile duct opening in 2nd part) So 2nd part has double -

Digestive System
Naziha Sultan Ahmed, BVMS, MSc Scientific degree (Assis. Prof.), Department of Anatomy College of Veterinary Medicine, University of Mosul, Mosul, Iraq https://orcid.org/0000-0002-2856-8277 https://www.researchgate.net/profile/Naziha_Ahmed Anatomy | Part 18| 2nd year 2019 Digestive System Fixation of the liver (Ligaments of the liver): 1-Lesser omentum: consist of two parts: a/Hepatogastric ligament: connect between hepatic porta and lesser curvature of the stomach . b/Hepatoduodenal ligament: connect between hepatic porta and the cranial part of the duodenum. 2-Coronary ligament: connect between the parietal (diaphragmatic ) surface of liver, with the diaphragm and the caudal vena cava. 3-Falciform ligament: connect between the notch of round ligament in the liver and the sternal part of the diaphragm. 4-Round ligament: the residue (remnants) of the umbilical vein of the fetus. 5-Hepatorenal ligament: connect between the right lobe of liver and the right kidney. 6-Right & left triangular ligaments: connect between the dorsal border of right and left lobes of the liver and the diaphragm . Both ligaments continue medially with the coronary ligament. CouAnatomy | Digestive system | Assis. Prof. Naziha Sultan Ahmed Page | 1 The pancreas: Pancreas has V-shape. It consists of base and two limbs (right & left limbs). *In horse: large pancreas body perforated by portal vein and long left limb, with short right limb (because of large size of cecum in horse ). The horse pancreas has two ducts: 1-Chief pancreatic duct: opens with bile duct at the major duodenal papilla. 2-Accessory pancreatic duct: opens at the minor duodenal papilla. *In dog: pancreas notched by the portal vein. -

Albany Med Conditions and Treatments
Albany Med Conditions Revised 3/28/2018 and Treatments - Pediatric Pediatric Allergy and Immunology Conditions Treated Services Offered Visit Web Page Allergic rhinitis Allergen immunotherapy Anaphylaxis Bee sting testing Asthma Drug allergy testing Bee/venom sensitivity Drug desensitization Chronic sinusitis Environmental allergen skin testing Contact dermatitis Exhaled nitric oxide measurement Drug allergies Food skin testing Eczema Immunoglobulin therapy management Eosinophilic esophagitis Latex skin testing Food allergies Local anesthetic skin testing Non-HIV immune deficiency disorders Nasal endoscopy Urticaria/angioedema Newborn immune screening evaluation Oral food and drug challenges Other specialty drug testing Patch testing Penicillin skin testing Pulmonary function testing Pediatric Bariatric Surgery Conditions Treated Services Offered Visit Web Page Diabetes Gastric restrictive procedures Heart disease risk Laparoscopic surgery Hypertension Malabsorptive procedures Restrictions in physical activities, such as walking Open surgery Sleep apnea Pre-assesment Pediatric Cardiothoracic Surgery Conditions Treated Services Offered Visit Web Page Aortic valve stenosis Atrial septal defect repair Atrial septal defect (ASD Cardiac catheterization Cardiomyopathies Coarctation of the aorta repair Coarctation of the aorta Congenital heart surgery Congenital obstructed vessels and valves Fetal echocardiography Fetal dysrhythmias Hypoplastic left heart repair Patent ductus arteriosus Patent ductus arteriosus ligation Pulmonary artery stenosis -
Pancreas Divisum: Evaluation and Treatment of a Persistently Controversial Anatomic Finding
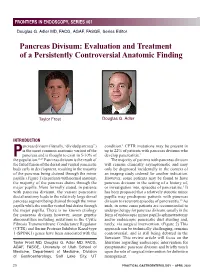
FRONTIERS IN ENDOSCOPY, SERIES #61 FRONTIERS IN ENDOSCOPY, SERIES #61 Douglas G. Adler MD, FACG, AGAF, FASGE, Series Editor Pancreas Divisum: Evaluation and Treatment of a Persistently Controversial Anatomic Finding Taylor Frost Douglas G. Adler INTRODUCTION ancreas divisum (literally, “divided pancreas”) condition.1 CFTR mutations may be present in is the most common anatomic variant of the up to 22% of patients with pancreas divisum who pancreas and is thought to exist in 5-10% of develop pancreatitis.2 P 36,37 the population. Pancreas divisum is the result of The majority of patients with pancreas divisum the failed fusion of the dorsal and ventral pancreatic will remain clinically asymptomatic and may buds early in development, resulting in the majority only be diagnosed incidentally in the context of of the pancreas being drained through the minor an imaging study ordered for another indication. papilla. (Figure 1) In patients with normal anatomy, However, some patients may be found to have the majority of the pancreas drains through the pancreas divisum in the setting of a history of, major papilla. More formally stated, in patients or investigation into, episodes of pancreatitis.3 It with pancreas divisum, the variant pancreatic has been proposed that a relatively stenotic minor ductal anatomy leads to the relatively large dorsal papilla may predispose patients with pancreas pancreas segment being drained through the minor divisum to recurrent episodes of pancreatitis.15 As papilla while the smaller ventral bud drains through such, in some cases patients are recommended to the major papilla. There is no known etiology undergo therapy for pancreas divisum, usually in the for pancreas divisum however, some genetic form of endoscopic minor papilla sphincterotomy abnormalities including mutations in the Cystic and/or endoscopic pancreatic duct stenting and, Fibrosis Transmembrane Conductance Regulator rarely, via surgical intervention. -
Digestive System
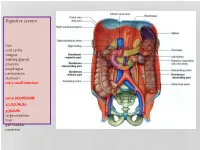
Digestive system Lips oral cavity tongue salivary glands pharynx esophagus peritoneum stomach m6-7 small intestine: cm25 DEODENUM: 2/5JEJUNUM: 3/5ILIUM: large intestine liver gall bladder pancreas :Duodenum Sup. Part Descending part Horizontal part Ascending part Major duodenal papilla Minor duodenal papilla : JEJUNUM / ILIUM From duodenojejunal curvature To Iliocecal Different jejunum & ilium 3Tenia coli: sigmoid 2 / rectum 0 Houstra / saccule Appendices epiploicae : No in Appendix / cecum / rectum Many in sigmoid DIFFERENT BETWEEN SMALL AND LARGE INTESTINE large intestine 1.5m Cecum appendix ascending colon transverse colon descending colon sigmoid colon rectum anal canal McBurneys point ascending colon transverse colon descending colon sigmoid colon :Rectum cm 12 Sacral flexure Puborectalis muscle Perineal flexure Rectum Ampulla : Anal canal cm 4 sup. = anal column / anal valve / anal sinus / pectinate line 2/3 Hiltons white line .inf 1/3 :Anal sphincter Internal sphincter External sphincter: deep / superficial / subcutaneous Liver: 1.5 kgr Located in Rt. & lf. Hypochondriac & epigastric region Surfaces: Sup. Anterior Surface: falciform ligament Inf. Surface: H shape fissure / porta hepatis / quadrate lobe / qudate lobe Post. Surface: bare area Rt. Surface: ribs 7-11 / Rt. lung Liver viewed from posterior Liver viewed from inferior Liver viewed from inferior Liver viewed from posterior :Liver vasculature 20%Hepatic artery 80%Portal vein Supra hepatic vein IVC :Nerve Sympathetic Parasympathetic From Vagus+ Phernic + celiac :Gall bladder Located in inf. Surface of liver cm7-10 Length: cm3-4 Wide: :Structure Fundus Body Infundibulum Neck Systic duct :Pancreas 2–L1 L cm15-20 Length: cm3Wide: cm2 Thickness: gram 90 :Structure Head :Uncinate process / sup. Mesenteric artery Neck: portal vein / sup. -

The Gallbladder
The Gallbladder Anatomy of the gallbladder Location: Right cranial abdominal quadrant. In the gallbladder fossa of the liver. o Between the quadrate and right medial liver lobes. Macroscopic: Pear-shaped organ Fundus, body and neck. o Neck attaches, via a short cystic duct, to the common bile duct. Opens into the duodenum via sphincter of Oddi at the major duodenal papilla. Found on the mesenteric margin of orad duodenum. o 3-6 cm aboral to pylorus. 1-2cm of distal common bile duct runs intramural. Species differences: Dogs: o Common bile duct enters at major duodenal papilla. Adjacent to pancreatic duct (no confluence prior to entrance). o Accessory pancreatic duct enters at minor duodenal papilla. ± 2 cm aboral to major duodenal papilla. MAJOR conduit for pancreatic secretions. Cats: o Common bile duct and pancreatic duct converge before opening at major duodenal papilla. Thus, any surgical procedure that affects the major duodenal papilla can affect the exocrine pancreatic secretions in cats. o Accessory pancreatic duct only seen in 20% of cats. 1 Gallbladder wall: 5 histologically distinct layers. From innermost these include: o Epithelium, o Submucosa (consisting of the lamina propria and tunica submucosa), o Tunica muscularis externa, o Tunica serosa (outermost layer covers gallbladder facing away from the liver), o Tunica adventitia (outermost layer covers gallbladder facing towards the liver). Blood supply: Solely by the cystic artery (derived from the left branch of the hepatic artery). o Susceptible to ischaemic necrosis should its vascular supply become compromised. Function: Storage reservoir for bile o Concentrated (up to 10-fold), acidified (through epithelial acid secretions) and modified (by the addition of mucin and immunoglobulins) before being released into the gastrointestinal tract at the major duodenal. -

Aandp2ch25lecture.Pdf
Chapter 25 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction • Most nutrients we eat cannot be used in existing form – Must be broken down into smaller components before body can make use of them • Digestive system—acts as a disassembly line – To break down nutrients into forms that can be used by the body – To absorb them so they can be distributed to the tissues • Gastroenterology—the study of the digestive tract and the diagnosis and treatment of its disorders 25-2 General Anatomy and Digestive Processes • Expected Learning Outcomes – List the functions and major physiological processes of the digestive system. – Distinguish between mechanical and chemical digestion. – Describe the basic chemical process underlying all chemical digestion, and name the major substrates and products of this process. 25-3 General Anatomy and Digestive Processes (Continued) – List the regions of the digestive tract and the accessory organs of the digestive system. – Identify the layers of the digestive tract and describe its relationship to the peritoneum. – Describe the general neural and chemical controls over digestive function. 25-4 Digestive Function • Digestive system—organ system that processes food, extracts nutrients, and eliminates residue • Five stages of digestion – Ingestion: selective intake of food – Digestion: mechanical and chemical breakdown of food into a form usable by