Availability of Essential Medicines in a Country in Conflict: a Quantitative
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
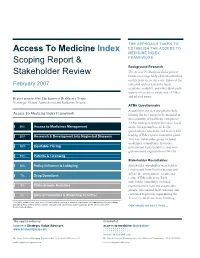
Access to Medicine Index Scoping Report & Stakeholder Review
THE APPROACH TAKEN TO Access To Medicine Index ESTABLISH THE ACCESS TO MEDICINE INDEX Scoping Report & FRAMEWORK Background Research The Access To Medicine Index project Stakeholder Review builds on a large body of work published on this issue in recent years. Innovest has February 2007 collected and reviewed the latest academic, industry, and other third-party reports on access to medicines (ATMs) and related issues. Report prepared by The Innovest Healthcare Team: Veronique Menou, Adam Savitz and Katharine Preston. ATMs Questionnaire A questionnaire was designed to help Access To Medicine Index Framework identify the key issues to be included in an evaluation of healthcare companies’ ATMs strategies and performance based 20% Access to Medicines Management on the background research. The questionnaire was delivered to over 200 20% Research & Development into Neglected Diseases leading ATMs experts around the globe. This key stakeholder group included academics, consultants, investors, 18% Equitable Pricing government representatives, and non- governmental organizations (NGOs). 15% Patents & Licensing Stakeholder Roundtables 10% Policy Influence & Lobbying Stakeholder roundtables were held in London and New York to discuss and debate the questionnaire results and 7% Drug Donations refine ATMs indicators. Each stakeholder roundtable included 5% Philanthropic Activities representatives from the stakeholder groups, who shared their expertise and 5% Ethical Promotion & Marketing Activities continued to provide input during the Access To Medicine Index building This table includes the eight most relevant criteria, ranked in order of importance, as indicated by the percentage weighting. This criteria will be used to evaluate each pharmaceutical company’s performance during the CONTINUED ON NEXT PAGE… benchmarking phase. -

Security Council Distr.: General 27 January 2020
United Nations S/2020/70 Security Council Distr.: General 27 January 2020 Original: English Letter dated 27 January 2020 from the Panel of Experts on Yemen addressed to the President of the Security Council The members of the Panel of Experts on Yemen have the honour to transmit herewith the final report of the Panel, prepared in accordance with paragraph 6 of resolution 2456 (2019). The report was provided to the Security Council Committee established pursuant to resolution 2140 (2014) on 27 December 2019 and was considered by the Committee on 10 January 2020. We would appreciate it if the present letter and the report were brought to the attention of the members of the Security Council and issued as a document of the Council. (Signed) Dakshinie Ruwanthika Gunaratne Coordinator Panel of Experts on Yemen (Signed) Ahmed Himmiche Expert (Signed) Henry Thompson Expert (Signed) Marie-Louise Tougas Expert (Signed) Wolf-Christian Paes Expert 19-22391 (E) 070220 *1922391* S/2020/70 Final report of the Panel of Experts on Yemen Summary After more than five years of conflict, the humanitarian crisis in Yemen continues. The country’s many conflicts are interconnected and can no longer be separated by clear divisions between external and internal actors and events. Throughout 2019, the Houthis and the Government of Yemen made little headway towards either a political settlement or a conclusive military victory. In a continuation from 2018, the belligerents continued to practice economic warfare: using economic obstruction and financial tools as weapons to starve opponents of funds or materials. Profiteering from the conflict is endemic. -

Maximising Access to Essential Medicines for Church Health
Maximizing access to essential medicines for church health services and their clients in Malawi: A baseline study Ecumenical Pharmaceutical Network (EPN) 1 INTRODUCTION Church health services (CHS) in Malawi provide approximately 37% of available health care. The Christian Health Association of Malawi (CHAM) reports that church health care facilities in Malawi number 33 hospitals and 132 clinics at the time of research. The government pays all health personnel salaries in CHSs and some allowances such as housing and transport. Government facilities offer free health care (including consultation and medications), while the CHSs charge. In many areas, the CHS is the sole provider of health care. This study used four methods to discover more about the situation: Tool 1 Church health service self-assessment survey (35 responses). Tool 2 Desk review. Tool 3 Guided self-assessment workshop and focus group for 10 hospitals, including spider diagrams, force field analysis, and problem trees. Tool 4 Drug supply organization self-assessment survey. 1.1 Identifying guidelines for increasing access Step 1: Each EPN country focal point was asked to identify the strengths and weaknesses of the CHSs in their country. From the combined responses, a list of common factors was drawn up. Step 2: A specialist working group then examined these factors in detail against the following criteria: What factors affect the cost of pharmaceuticals to the CHS? Factors are external to the CHS? Factors are internal to the CHS? What factors affect the cost of pharmaceuticals to patients? Which of the resulting factors can EPN and CHSs address? What are the initial values of indicators for these guidelines? Step 3: The results of the working group were presented to a larger meeting of 16 drug supply organizations and EPN Board members, who together agreed to add a number of guidelines, prioritized their importance, and addressed the search for indicators for each of the guidelines. -

The War in Yemen: 2011-2018: the Elusive Road to Peace
Working Paper 18-1 By Sonal Marwah and Tom Clark The War in Yemen: 2011-2018 The elusive road to peace November 2018 The War in Yemen: 2011-2018 The elusive road to peace By Sonal Marwah and Tom Clark Working Paper 18-1 Library and Archives Canada Cataloguing in Publications Data The War in Yemen: 2011-2018: The elusive road to peace ISBN 978-1-927802-24-3 © 2018 Project Ploughshares First published November 2018 Please direct enquires to: Project Ploughshares 140 Westmount Road North Waterloo, Ontario N2L 3G6 Canada Telephone: 519-888-6541 Email: [email protected] Editing: Wendy Stocker Design and layout: Tasneem Jamal Table of Contents Glossary of Terms i List of Figures ii Acronyms and Abbreviations iii Acknowledgements v Executive Summary 1 Introduction 2 Background 4 Participants in the Conflict 6 Major local actors 6 Foreign and regional actors 7 Major arms suppliers 7 Summary of the Conflict (2011-2018) 8 Civil strife breaks out (January 2011 to March 2015) 8 The internationalization of conflict (2015) 10 An influx of weapons and more human-rights abuses (2016) 10 A humanitarian catastrophe (2017- June 2018) 13 The Scale of the Forgotten War 16 Battle-related deaths 17 Forcibly displaced persons 17 Conflict and food insecurity 22 Infrastructural collapse 23 Arming Saudi Arabia 24 Prospects for Peace 26 Regulation of Arms Exports 30 The Path Ahead and the UN 32 Conclusion 33 Authors 34 Endnotes 35 Photo Credits 41 Glossary of Terms Arms Trade Treaty: A multilateral treaty, which entered into force in December 2014, that establishes -
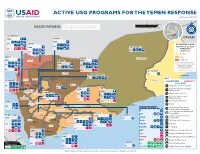
USG Yemen Complex Emergency Program
ACTIVE USG PROGRAMS FOR THE YEMEN RESPONSE Last Updated 02/12/20 0 50 100 mi INFORMA Partner activities are contingent upon access to IC TI PH O A N R U G SAUDI ARABIA conict-aected areas and security concerns. 0 50 100 150 km N O I T E G U S A A D ID F /DCHA/O AL HUDAYDAH IOM AMRAN OMAN IOM IPs SA’DAH ESTIMATED FOOD IPs SECURITY LEVELS IOM HADRAMAWT IPs THROUGH IPs MAY 2020 IPs Stressed HAJJAH Crisis SANA’A Hadramawt IOM Sa'dah AL JAWF IOM Emergency An “!” indicates that the phase IOM classification would likely be worse IPs Sa'dah IPs without current or planned IPs humanitarian assistance. IPs Source: FEWS NET Yemen IPs AL MAHRAH Outlook, 02/20 - 05/20 Al Jawf IP AMANAT AL ASIMAH Al Ghaedha IPs KEY Hajjah Amran Al Hazem AL MAHWIT Al Mahrah USAID/OFDA USAID/FFP State/PRM Marib IPs Hajjah Amran MARIB Agriculture and Food Security SHABWAH IPs IBB Camp Coordination and Camp Al Mahwit IOM IPs Sana'a Management Al Mahwit IOM DHAMAR Sana'a IPs Cash Transfers for Food Al IPs IPs Economic Recovery and Market Systems Hudaydah IPs IPs Food Voucher Program RAYMAH IPs Dhamar Health Raymah Al Mukalla IPs Shabwah Ataq Dhamar COUNTRYWIDE Humanitarian Coordination Al Bayda’ and Information Management IP Local, Regional, and International Ibb AD DALI’ Procurement TA’IZZ Al Bayda’ IOM Ibb ABYAN IOM Al BAYDA’ Logistics Support and Relief Ad Dali' OCHA Commodities IOM IOM IP Ta’izz Ad Dali’ Abyan IPs WHO Multipurpose Cash Assistance Ta’izz IPs IPs UNHAS Nutrition Lahij IPs LAHIJ Zinjubar UNICEF Protection IPs IPs WFP Ready-to-Use Therapeutic Food IOM Al-Houta ADEN FAO Refugee and Migrant Assistance IPs Aden IOM UNICEF Risk Management Policy and Practice Shelter and Settlements IPs WFP SOCOTRA DJIBOUTI, ETHIOPIA, U.S. -
Struggle for Citizenship.Indd
From the struggle for citizenship to the fragmentation of justice Yemen from 1990 to 2013 Erwin van Veen CRU Report From the struggle for citizenship to the fragmentation of justice FROM THE STRUGGLE FOR CITIZENSHIP TO THE FRAGMENTATION OF JUSTICE Yemen from 1990 to 2013 Erwin van Veen Conflict Research Unit, The Clingendael Institute February 2014 © Netherlands Institute of International Relations Clingendael. All rights reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the copyright holders. Clingendael Institute P.O. Box 93080 2509 AB The Hague The Netherlands Email: [email protected] Website: http://www.clingendael.nl/ Table of Contents Executive summary 7 Acknowledgements 11 Abbreviations 13 1 Introduction 14 2 Selective centralisation of the state: Commerce and security through networked rule 16 Enablers: Tribes, remittances, oil and civil war 17 Tools: Violence, business and religion 21 The year 2011 and the National Dialogue Conference 26 The state of justice in 1990 and 2013 28 3 Trend 1: The ‘instrumentalisation’ of state-based justice 31 Key strategies in the instrumentalisation of justice 33 Consequences of politicisation and instrumentalisation 34 4 Trend 2: The weakening of tribal customary law 38 Functions and characteristics of tribal law 40 Key factors that have weakened tribal law 42 Consequences of weakened tribal law 44 Points of connection -

A New Model for Defeating Al Qaeda in Yemen
A New Model for Defeating al Qaeda in Yemen Katherine Zimmerman September 2015 A New Model for Defeating al Qaeda in Yemen KATHERINE ZIMMERMAN SEPTEMBER 2015 A REPORT BY AEI’S CRITICAL THREATS PROJECT TABLE OF CONTENTS Executive Summary ....................................................................................................................................... 1 Introduction ................................................................................................................................................. 3 Part I: Al Qaeda and the Situation in Yemen ................................................................................................. 5 A Broken Model in Yemen ...................................................................................................................... 5 The Collapse of America’s Counterterrorism Partnership ........................................................................ 6 The Military Situation in Yemen ........................................................................................................... 10 Yemen, Iran, and Regional Dynamics ................................................................................................... 15 The Expansion of AQAP and the Emergence of ISIS in Yemen ............................................................ 18 Part II: A New Strategy for Yemen ............................................................................................................. 29 Defeating the Enemy in Yemen ............................................................................................................ -

In South Africa: Access to Medicines in the Neoliberal Era an Insight Into the Public Market of Antiretroviral Treatments in South Africa
Angles New Perspectives on the Anglophone World 8 | 2019 Neoliberalism in the Anglophone World How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era An insight into the public market of antiretroviral treatments in South Africa Charlotte Pelletan Electronic version URL: http://journals.openedition.org/angles/613 DOI: 10.4000/angles.613 ISSN: 2274-2042 Publisher Société des Anglicistes de l'Enseignement Supérieur Electronic reference Charlotte Pelletan, « How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era », Angles [Online], 8 | 2019, Online since 01 April 2019, connection on 28 July 2020. URL : http://journals.openedition.org/angles/613 ; DOI : https://doi.org/10.4000/angles.613 This text was automatically generated on 28 July 2020. Angles. New Perspectives on the Anglophone World is licensed under a Creative Commons Attribution- NonCommercial-ShareAlike 4.0 International License. How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the... 1 How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era An insight into the public market of antiretroviral treatments in South Africa Charlotte Pelletan Introduction “I am not using strong words; I am using appropriate words. This is genocide”. Health Minister Aaron Motsoaledi (De Wet 2014) When the Minister of Health talks left… 1 In 1997, while the AIDS epidemic was spreading, the South African government explored changes to its regulation of patents in the Medicines Act and its National Drug Policy. It triggered a world-famous law case pitting the South African state against a coalition of pharmaceutical companies: the Medicines Act case, which concluded in 2001, also known as the Pretoria trial. -

Eastern Mediterranean La Revue De Santé De La Health Journal Méditerranée Orientale
Eastern Mediterranean La Revue de Santé de la Health Journal Méditerranée orientale Nurses make up the largest group of health-care providers and are the first point of contact in health service delivery of diabetes in terms of detection, treatment and rehabilitation. This year’s World Diabetes Day coincides with the International Year of the Nurse and the Midwife, as designated by the World Health Assembly, and looks to focus on and promote the role of nurses in the prevention and management of diabetes. المجلد السادس والعشرون / عدد Volume 26 / No. 11 2020 11 نوفمبر/تشرين الثاني November/Novembre Eastern Mediterranean Health Journal Members of the WHO Regional Committee for the Eastern Mediterranean IS the official health journal published by the Eastern Mediterranean Regional Office of the World Health Organization. It is a forum for Afghanistan . Bahrain . Djibouti . Egypt . Islamic Republic of Iran . Iraq . Jordan . Kuwait . Lebanon the presentation and promotion of new policies and initiatives in public health and health services; and for the exchange of ideas, concepts, Libya . Morocco . Oman . Pakistan . Palestine . Qatar . Saudi Arabia . Somalia . Sudan . Syrian Arab Republic epidemiological data, research findings and other information, with special reference to the Eastern Mediterranean Region. It addresses Tunisia . United Arab Emirates . Yemen all members of the health profession, medical and other health educational institutes, interested NGOs, WHO Collaborating Centres and individuals within and outside the Region. البلدان أعضاء اللجنة اإلقليمية ملنظمة الصحة العاملية لرشق املتوسط املجلة الصحية لرشق املتوسط األردن . أفغانستان . اإلمارات العربية املتحدة . باكستان . البحرين . تونس . ليبيا . مجهورية إيران اإلسالمية هىاملجلة الرسمية التى تصدر عن املكتب اإلقليمى لرشق املتوسط بمنظمة الصحة العاملية. -

IFMSA Policy Document Access to Medicines
IFMSA Policy Document Access to Medicines Proposed by Team of Officials Adopted by IFMSA General Assembly March Meeting 2019, in Portorož, Slovenia. Policy Statement Introduction: Access to affordable medicines and vaccines is an essential part of achieving Universal Health Coverage (UHC) and resilient health systems, as mentioned in Sustainable Development Goal (SDG) 3, Target 3.8. However, 2 billion people worldwide currently do not have access to essential medicines. IFMSA position: The International Federation of Medical Students' Associations (IFMSA), strongly believes that access to affordable, effective, and safe technologies is a human right. We believe that the current research and development (R&D) system lacks transparency and is driven by commercial interests rather than public health needs, which is in turn reducing the availability of affordable medicines. Publicly funded research, with its publicly-oriented incentives, makes an essential contribution to the development of medicines which should not be appropriated for commercial profit. Global patent monopolies for the protection of intellectual property (IP), as well as Free Trade Agreements (FTAs), such as Trade- Related Aspects of Intellectual Property Rights (TRIPS), are one of the most important barriers to generic medicine production. Additionally, TRIPS plus provisions, included in smaller FTAs, grant data exclusivity which stifles market approval for lower-cost alternatives. We support the use of TRIPS flexibilities as an internationally accepted tool to mitigate -

Missing Medicines in Malawi: Campaigning Against Stock-Outs of Essential Drugs Oxfam Programme Insights
Missing Medicines in Malawi Campaigning against ‘stock-outs’ of essential drugs A community march to protest about the lack of basic medicines at the local clinic. The march was followed by an event to discuss health issues with partner organizations and local leaders. Photo: Word Alive Commission for Relief and Development (WACRAD), Malawi. Malawi is one of the poorest countries in the world. The government has introduced some measures to improve the health of its people, but a number of major problems remain. One of these is the lack of essential medicines in government health clinics – known as ‘stock-outs’. These medicines should be free to poor people, but most find that they have to pay. This paper looks at an innovative campaign which aimed to tackle this problem by enhancing the capacity of local communities and civil society organizations to demand the right to access these medicines. The campaign also lobbied for a commitment to ensure increased availability and accessibility in rural areas and carried out budget and resource tracking. This paper looks at the difficulties the Programme Insights Programme campaign faced and outlines the factors that contributed to its success. Introduction Malawi is one of the poorest countries in the world, with more than half its population living on less than a dollar a day. Local-level campaigning on access to medicines took place in six districts in the southern part of the country. ‘Access to essential medicines is a human right and a 1 cornerstone of an effective primary health care system.’ Malawi is one of the poorest countries in the world. -

Access to Essential Medicines As a Component of the Right to Health Stephen P
Health: A Human Rights Perspective 82 ACCESS TO ESSENTIAL MEDICINES AS A COMPONENT OF THE RIGHT TO HEALTH Stephen P. Marks Introduction In Human Rights Obligations of Non-State Actors, Andrew Clapham wrote, “Perhaps the most obvious threat to human rights has come from the in- ability of people to achieve access to expensive medicine, particularly in the context of HIV and AIDS.”1 He was referring to threats to human rights from intellectual property agreements under the World Trade Organiza- tion, which are often seen as obeying a different – and many would say ut- terly incompatible – logic than human rights. The right to health, in the interpretation of the Committee on Economic Social and Cultural Rights, means that “States Parties … have a duty to prevent unreasonably high costs for access to essential medicines.”2 This chapter will explain the significance and place of the human right to essential medicines as a derivative right within the broader right to the highest attainable standard of physical and mental health. As a component of the right to health, the right to essential medicines depends not only on the production, distribution, and pricing of medicines, but also on the in- centives for research and development of drugs needed to treat diseases in developing countries, functioning health systems so that drugs are part of a rational system of quality treatment and care, as well as on infrastructure, Access to Essential Medicines as a Component of the Right to Health 83 so that they can be delivered to all areas where they are needed. Consider- ing that these broader issues are examined in other chapters, this chap- ter will focus more on the impediment to the realization of the right to essential medicines caused by the protection of intellectual property.